Information Links
Related Conferences
Current Issue Volume 10, Issue 1 - 2025
An Integrated Image-Guided/Adaptive Radiotherapy Workflow
CM Charlie Ma*, Ahmed Eldib, J Panetta, Lili Chen
Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, USA
*Corresponding author: Dr. CM Charlie Ma, Ph.D, Radiation Oncology Department, Fox Chase Cancer Center, 333 Cottman Avenue, Philadelphia, PA 19111, USA, Tel: (215) 728-2996, Fax: (215) 728-4789, Email: [email protected]
Received Date: April 18, 2025
Published Date: June 25, 2025
Citation: Ma C-M, et al. (2025). An Integrated Image-Guided/Adaptive Radiotherapy Workflow. Mathews J Cancer Sci. 10(1):53.
Copyrights: Ma C-M, et al. © (2025).
ABSTRACT
Specialized adaptive radiotherapy (ART) systems have been developed and clinically implemented, which are either cost-ineffective such as MR-linacs or inflexible in workflow such as the Ethos system, affecting their widespread clinical use. This work investigates a new workflow that integrates ART into the routine IGRT workflow seamlessly. The new workflow uses the same treatment simulation and planning process as in routine IGRT. During a treatment session, the patient will be set up and CBCT imaged, and the patient’s anatomy will be compared with the planned dose distribution to decide whether ART is needed. If so, new contours and treatment plans will be generated. Independent dosimetry verification will be performed before and after the dose delivery. Two novel strategies make the new workflow more effective and efficient: (1) the use of pre-selected isodose lines rather than the planning contours to match the patient’s anatomy, which can improve the target localization accuracy, thus reducing the need for re-planning, and (2) the use of direct-aperture optimization and MLC shape/weight adjustment to improve planning efficiency and plan quality over the scheduled plan. Results showed that strategy (1) can significantly improve the target localization accuracy and reduce the necessity of re-planning from 36.7% to 19.4% for 98 prostate fractions, and strategy (2) can significantly improve heterogeneity index and conformity index for the target and dose-volume parameters for lung, liver, kidney, bladder and rectum for 15 patients. The new workflow integrates ART into routine IGRT on existing clinical CBCT linacs, which can significantly improve the effectiveness and efficiency of IGRT/ART with the use of two novel strategies.
Keywords: Image-Guided Radiation Therapy (IGRT), Adaptive Radiation Therapy (ART), CT Simulation, Structure Contouring, Plan Optimization, Plan QA, Target Localization, Radiotherapy Workflow.
INTRODUCTION
Image guided radiation therapy (IGRT) has been implemented clinically with different imaging techniques including 2D and 3D kV and MV x-ray imaging with fiducial markers, 2D and 3D ultrasound imaging, MR imaging and electromagnetic transponder systems [1-11]. Advanced 3D imaging systems can provide diagnostic image quality for structure delineation and dose calculation/reconstruction in treatment assessment and adaptive radiotherapy (ART) [12-14]. Recent RT developments in advanced delivery techniques such as intensity modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT) and proton and carbon ion therapy together with precise target localization techniques have enabled dose escalation and hypo-fractionation clinical trials that also utilized stereotactic body radiation therapy (SBRT) techniques [15-17] with both IGRT and ART workflows.
The workflow for conventional IGRT on an x-ray cone-beam CT (CBCT) linac consists of two stages: (1) pre-treatment simulation and treatment planning, and (2) clinical treatment with image guidance. As shown in figure 1, a patient is set up with proper immobilization devices and treatment simulation is performed with different image modalities such as CT, MR and PET. Treatment targets and organs at risk (OAR) are contoured on these images, which are used in treatment plan optimization to achieve optimal tumor control and normal tissue sparing. Dosimetric plan quality assurance (QA) is carried out to ensure accurate dose delivery. During a clinical treatment session, the patient is set up with the same immobilization devices and a CBCT is performed. The patient’s anatomy on the treatment CBCT is fused with that on the simulation CT by rigid registration. The target and OAR contours may be used to facilitate the alignment (or the best match) of the patient’s anatomy between the simulation CT and the treatment CBCT. Couch rotations/shifts may be performed based on the fusion results to correct for the setup error and/or inter-fractional organ motion effect as much as possible before the treatment. The same treatment plan is used for all treatment fractions ignoring the dosimetric effect of any residual anatomy mismatch between simulation and treatment.
.png)
Figure 1. The conventional workflow for image-guided radiation therapy (IGRT), which consists of two stages: (1) pre-treatment simulation and planning and (2) clinical treatment with image-guidance. The same treatment plan is used for all treatment fractions.
Special ART machines developed by different vendors implemented their own workflows for ART based on the image modalities used, e.g., MRI or CBCT [18-22]. The Ethos system (Varian Medical Systems, Palo Alto, CA) allows both IGRT and ART treatment on the treatment machine with two separate workflows. As shown in Figure 2, the IGRT workflow is the same as that described in Figure 1. For ART, the pre-treatment simulation and planning process is the same as that of IGRT to generate a reference treatment plan. During an ART treatment session, the patient is set up and a CBCT is performed. The target and OARs are recontoured based on the patient’s anatomy on the CBCT and a new adaptive plan is generated using the same beam arrangements and target/OAR dose constraints as used in the original optimization process for the reference plan. The reference plan is also re-calculated based on the CBCT (and the new contours) and the isocenter shift needed based on a rigid registration between the simulation CT and the CBCT, to generate a scheduled plan, which is then compared to the new adaptive plan according to the pre-set clinical goals and dose constraints. If a clinical decision is made to use the adaptive plan, an independent plan QA is performed for the adaptive plan before proceeding to the treatment.
.png)
Figure 2. The Ethos workflow for IGRT and ART. The pre-treatment simulation and planning stage is the same as that of conventional IGRT but separate treatment workflows are used for IGRT and ART, which are not interchangeable.
ART is a time-consuming treatment procedure because structure contouring, plan optimization, evaluation and QA may all take a significant amount of time. Typical x-ray CBCT based ART sessions took 15-30 minutes for prostate treatment and 30-50 minutes for abdominal sites while MRI-linacs would take a longer amount of time [18-22]. Thus, ART will not be suitable for most IGRT treatment sessions in which patient’s setup errors and/or inter-fractional organ motion effects are generally small and can be easily corrected satisfactorily (e.g., with couch shifts and/or rotations). ART is only needed for those treatment sessions in which significant dosimetric benefits can be achieved through re-planning. However, the current ART workflows on exiting special ART machines are not flexible. If a patient is selected for ART on the Ethos, for example, one must go through the entire ART workflow for every treatment session even if there are negligible changes in the treatment geometry. The only step that can be saved is plan QA if a scheduled plan is selected. On the other hand, if a patient is selected for IGRT, which is a decision to be made during treatment planning, one cannot switch to ART even if significant anatomy changes occurred in a treatment session.
In this paper, a new workflow is proposed to combine both IGRT and ART in the same treatment procedure. Patients undergoing IGRT treatments can be treated effectively and efficiently if their setup errors and/or inter-fractional target/organ motion effects can be corrected satisfactorily. ART is only applied to treatment sessions in which the treatment geometry on daily CBCT is significantly different from that on the simulation CT, thus re-planning is necessary to improve the target coverage and normal structure sparing. Two useful strategies are introduced into the workflow to reduce the need for ART and to simplify the optimization process if ART is necessary but the change in treatment geometry is only moderate. A full-blown plan optimization is only needed for large variations of anatomical structures such as the stomach or bowel in the abdomen or the bladder and rectum in the pelvis that significantly change the target shape and location relative to the nearby critical structures, resulting in deteriorated target dose coverage and/or normal tissue doses.
MATERIALS AND METHODS
This study describes a simple workflow that integrates ART into the routine IGRT treatment procedure, which allows adaptive re-planning for treatment sessions with large setup errors and inter-fractional target/organ variations outside the clinical tolerance. Figure 3 shows the pre-treatment simulation and planning workflow, which is the same as that of conventional IGRT, and the modified treatment workflow, which is the same as that of IGRT if the setup error or patient’s inter-fractional organ motion effect can be corrected satisfactorily through isocenter movement or couch rotation. An important improvement in this workflow is the introduction of a strategy to perform a dosimetry evaluation rather than a simple anatomy matchup based on the daily CBCT so that for treatment sessions with large setup and/or anatomical/dosimetric changes for which re-planning is deemed necessary, ART will be initiated. This dosimetry-guided procedure not only improves the dose distributions received by the patients but also reduces the need for re-planning, thus improving both clinical effectiveness and efficiency.
.png)
(a) (b)
Figure 3. An integrated IGRT/ART workflow proposed in this work. The pre-treatment simulation and planning stage is the same as that of conventional IGRT and the treatment stage is the same as that of IGRT except for treatment sessions with large setup and/or anatomical/dosimetric changes for which re-planning is deemed necessary.
The strategy to match the initial plan dose distribution with the patient’s anatomy on the treatment CBCT was based on our early work [23]. Conventional target localization based on anatomy matching has established population-based target margins for IGRT but not effective for those patients with large setup errors (especially rotational errors) and/or large inter-fractional organ motion (especially organ deformation). For such outliers, the target volume can only be matched partially (e.g., the best match of the contours in 3 major planes), which does not always result in the best dose distribution for the treatment geometry. However, if target localization is done by aligning the prescription isodose surface with the treatment geometry, both the target coverage and normal tissue doses can be evaluated for the best outcome. The advantage of the new localization method is to have a complete set of tools including structure contours and isodose lines available to align the treatment geometry in this process. Different percentage isodose lines can be used to achieve a compromise between target coverage and normal tissue sparing. The original plan dose distribution together with the structure contours based on the simulation CT are transferred via the DICOM/RT plan object and used for the dosimetry assessment. However, fast GPU-based Monte Carlo dose calculation can be performed to provide more accurate dose distribution based on the treatment CBCT of the day depending on the implementation and dose calculation speed. An automatic match can also be performed for optimal target localization and dosimetry assessment for ART recommendation.
Our new ART workflow also follows the same steps as described in Figures 2 and 3 for currently available adaptive machines except for the treatment plan optimization process in which a two-tier optimization strategy is introduced. A drawback of existing ART systems is that the adaptive optimization process always starts completely from scratch, which is time consuming and often unnecessary as changes in treatment geometry are small. To reduce the optimization time needed, fast optimization algorithms are used, which do not always find the global minimum although the same clinical goals and dose constraints are used as established for the reference plan. Sometimes, the quality of the adaptive plan may be inferior to that of the scheduled plan, which is not only a disappointment but also futile and unproductive. This problem can be completely avoided using our new strategy. The first tier of the optimization process is a direct-aperture optimization (DAO) that simply modifies the shapes and weights of the MLC segments [24-29] using the same objective function and the optimization parameters as used for the reference plan. However, if the treatment geometry has drastic changes and a better adaptive plan cannot be found through DAO, a change of the objective function or some optimization parameters may be necessary, which will trigger the second-tier optimization. Such a change effectively defines a new solution space that may provide an adaptive plan to meet the clinical acceptance criteria, which is a step forward compared to existing ART systems that would not allow any changes of the clinical goals and dose constraints.
To investigate the potential improvement of the first strategy, a retrospective data analysis was performed to estimate the possible reduction in IGRT treatment sessions that require adaptive replanning due to large setup errors and/or inter-factional organ motion. Treatment plans and imaging data of 30 previously treated prostate, lung and liver patients were de-archived and reanalyzed to determine the number of treatment fractions that failed our clinical treatment plan acceptance criteria using conventional anatomy-based target localization or using our new prescription isodose guided target localization. The IGRT treatment workflow was the same as described in figure 1 except that the images were from a CT-on-rails system instead of a CBCT. The prostate target was aligned with the simulation CT geometry and an isocenter shift was made based on the best match of the prostate volume prior to the treatment (i.e., the conventional method). For this study, a retrospective target localization was performed using the new isodose based method, which usually resulted in a different isocenter shift. The dose distributions for these treatment fractions were recalculated based on the two different target localization methods and the associated isocenter shift values. These are equivalent to the “scheduled” dose distributions for the Varian Ethos system. The cumulative dose received by 95% of the clinical target volume (CTV), D95%, and the minimal cumulative dose in the CTV, Dmin, were compared with those for the planning target volume (PTV) in the original treatment plans for the two methods. Other dosimetric parameters included the conformity index (CI), which is defined as the ratio of the prescription isodose volume to PTV, V1350, V4000 and V6500, which are the OAR volumes receiving doses 13.5 Gy, 40 Gy and 56 Gy, respectively. The details of the treatment simulation, planning, target alignment and plan analysis have been reported in a separate publication [23].
The RT-Pro treatment planning system (version 5.60.4657, Prowess Inc., Concord, CA) was used as an independent ART workstation, to implement the new adaptive workflow in this study, which employs the DAO optimization algorithm in both the first- and second-tier optimization process for the adaptive therapy application. The dose calculation was performed using the collapsed cone convolution (CCC) algorithm [30] and radiobiological dose conversion was enabled for different dose fractionation [31]. When replanning is deemed necessary, auto-contouring and replanning (either first- or second-tier optimization) will be performed. If an adaptive plan is selected for treatment, an independent plan QA will be carried out using a GPU-based Monte Carlo dose calculation tool. To further improve the optimization results for the RT-Pro TPS, a novel MLC leaf adjustment method was developed that works effectively with the DAO algorithm [29]. A retrospective analysis of the plan quality was performed based on 15 previously treated patients to estimate the gain in DAO optimization. The details of the leaf adjustment methods and the treatment planning/optimization process have been reported in a previous publication [29].
RESULTS
This work investigates a new workflow that integrates ART into the routine IGRT workflow seamlessly to improve effectiveness and efficiency. During a treatment session, the patient will be set up and CBCT imaged, and the patient’s anatomy will be compared with the planned dose distribution to assess the dosimetric impact of any inter-fractional anatomical changes and therefore to decide whether treatment re-planning is necessary. The novel aspects of the new ART workflow are the strategies to best align the target/critical organs with the scheduled dose distribution to reduce the need for re-planning and, if indeed replanning is needed, to use the two-tier optimization to improve the effectiveness and efficiency of ART treatment re-planning.
Table 1 shows the prescription dose Dp to 95% of the PTV and the minimal dose Dmin inside the PTV based on the initial treatment plan for 15 prostate patients investigated in our retrospective study. The prescription dose Dp was 76 Gy given to 95% of the PTV and our clinical acceptance criterion was Dmin ≥ 90% of Dp. The lowest Dmin for the original plan was 70.7 Gy for patient No. 13 and the mean Dmin for the original plans of all patients was 72 Gy, which is much higher than our acceptance criterion of 68.4 Gy. The cumulative dose received by 95% of the CTV based on the reconstructed dose distributions using CT-on-rails images on the treatment day (i.e., the scheduled treatment plans) is also shown in Table 1 for these patients together with the minimal cumulative dose inside the CTV, Dmin. The cumulative CTV doses D95% deviated from the originally planned doses by less than 3% (74.0 Gy – 78.2 Gy) no matter which target localization method was used. The cumulative Dmin, however, varied significantly depending on the localization method used, which resulted in different isocenter shifts, thus different scheduled dose distributions. The mean Dmin was 67.1 Gy using the conventional localization method of anatomy matching, and 70.5% using the new localization method by aligning the prescription isodose distribution with the treatment geometry, respectively. If we use Dmin < 68.4 Gy as a criterion for ART, 8 out of the 15 patients will need adaptive treatments using the conventional localization method, but no patients will need ART using the new localization method as shown in Table 1. This means that an effective target localization method may greatly improve the accuracy of IGRT dose delivery and therefore improve the IGRT treatment efficiency by reducing the need for adaptive therapy.
Table 1. Target dose comparison between the original treatment plan and the scheduled treatment plans when different target localization methods were used. Dmin is the minimal dose and D95% is the dose to 95% of the target volume. The cumulative dose was calculated based on the scheduled treatment plans applying isocenter shifts according to the target localization method used for individual treatment fractions
|
Patient No. |
Original Plan: PTV Dose (Gy) |
Scheduled Plans: Cumulative CTV Dose (Gy) |
||||
|
Conventional Localization |
New Localization |
|||||
|
D95% |
Dmin |
D95% |
Dmin |
D95% |
Dmin |
|
|
1 |
76.0 |
71.6 |
77.6 |
62.9 |
75.9 |
70.3 |
|
2 |
76.0 |
71.2 |
75.5 |
69.8 |
75.3 |
70.4 |
|
3 |
76.0 |
72.7 |
75.6 |
69.8 |
75.6 |
70.6 |
|
4 |
76.0 |
72.3 |
75.1 |
69.2 |
75.1 |
70.4 |
|
5 |
76.0 |
71.4 |
76.6 |
64.5 |
78.2 |
71.3 |
|
6 |
76.0 |
73.4 |
75.5 |
71.6 |
75.5 |
71.6 |
|
7 |
76.0 |
72.6 |
75.8 |
56.0 |
76.4 |
69.8 |
|
8 |
76.0 |
71.8 |
75.5 |
66.8 |
75.4 |
71.1 |
|
9 |
76.0 |
73.5 |
75.8 |
67.4 |
75.3 |
71.3 |
|
10 |
76.0 |
71.9 |
75.5 |
70.9 |
75.4 |
71.0 |
|
11 |
76.0 |
72.4 |
75.0 |
70.0 |
75.1 |
70.9 |
|
12 |
76.0 |
72.0 |
74.0 |
66.7 |
74.0 |
69.7 |
|
13 |
76.0 |
70.7 |
75.2 |
68.8 |
74.9 |
68.4 |
|
14 |
76.0 |
71.9 |
75.4 |
69.1 |
75.4 |
70.8 |
|
15 |
76.0 |
70.8 |
74.6 |
61.9 |
75.5 |
70.1 |
|
Mean |
76.0 |
72.0 |
75.5 |
67.1 |
75.5 |
70.5 |
.png)
Figure 4. The total number of treatment CT-on-rails scans (blue bars) used for the fractional dose reconstruction for each patient, and the number of fractions in which the minimum fractional dose inside the CTV was less than 90% of fractional Dp (red bars for the conventional anatomy matching method and green bars for the new method with prescription isodose surface matching).
The Prowess RT Pro system is flexible for implementing the two-tier optimization process using the DAO algorithm. The first tier of the optimization process simply modifies the shapes and weights of the MLC segments using the same objective function and the optimization parameters as used for the reference plan. This is more suitable for relatively small changes in treatment geometry as demonstrated in figure 5, where the target volume increased slightly but the relationship between the prostate and adjacent critical structures remained consistent (e.g., similar boundary shapes). Since DAO is a random sampling approach, which searches the global minimum in the given solution space, any accepted changes in the MLC segment shape and weight that correspond to an improvement in the objective function will result in a better dose distribution, thus ensuring that the new adaptive plan is always better than or at least equal to the scheduled plan. The second tier of the optimization process allows the planner to alter the objective function or some optimization parameters to deal with large changes in the volume and shape of the target and/or critical structures as demonstrated in figure 6, where the position, volume and shape of the target, large bowel and stomach varied drastically between the original simulation CT and the CBCT on the treatment day. This is equivalent to starting an optimization process with a new solution space that may provide an adaptive plan to meet the clinical acceptance criteria. Otherwise, more changes can be introduced to continue the optimization process until an acceptable plan is generated. Figure 7 shows the much-improved dose distribution for a prostate SBRT plan adapting to the significant changes of the target and rectal geometry in comparison to the scheduled plan. This two-tier optimization is a step forward compared to existing ART systems (e.g., Ethos) that would not allow any changes to the clinical goals and/or dose constraints.
.png)
Figure 5. Comparison of CBCT on the treatment day (left) and simulation CT (right) images showing small changes in the target geometry (red contours) and the boundary shape between the prostate and the adjacent critical structures (e.g., bladder: yellow contours, rectum: blue contours).
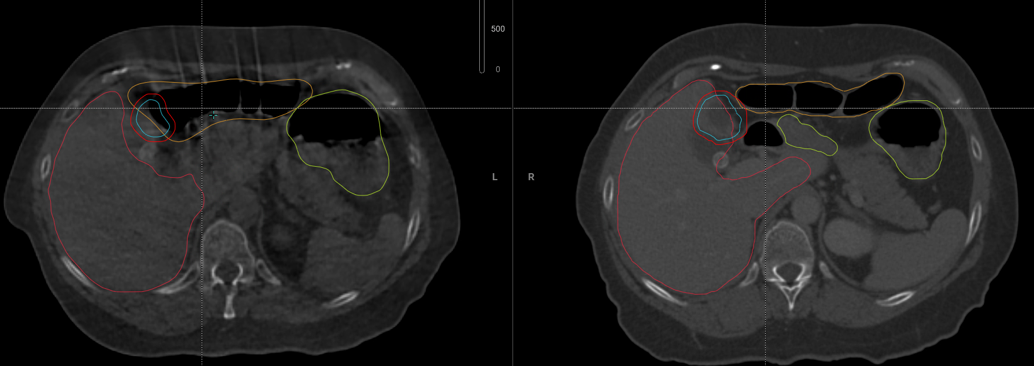
Figure 6. Comparison of CBCT on the treatment day (left) and simulation CT (right) images showing significant changes in the shape and volume of the target (red contours) and adjacent critical structures (e.g., stomach: yellow contours, large bowel: brown contours).
.png)
.png)
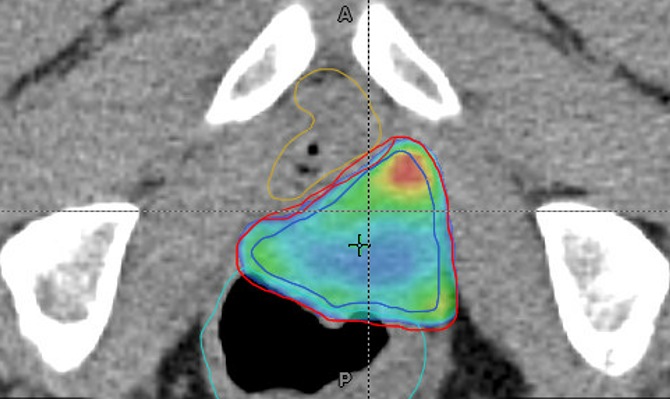
Figure 7. Comparison of CBCT on the treatment day (left and middle) and simulation CT (right) images showing significant changes in the target (red contours), rectum (blue contours) and bladder (yellow contours) and improved target and rectal doses in the adaptive plan (left) and deteriorated target and rectal doses in the scheduled plan (middle) with respect to the original reference plan (right).
As presented earlier, the treatment geometry in many radiotherapy fractions does not vary significantly from the simulation geometry, thus allowing quick modifications of the beam apertures to achieve satisfactory fractional dose distributions. Detailed dosimetric comparisons are made between the original 15 Prowess RT Pro plans and the retrospectively improved new plans with quick MLC leaf adjustments. Table 2 shows the maximum dose (D1%), minimum dose (D99%) and dose conformity index (CI) for the PTV of all treatment plans investigated. It is apparent that MLC leaf adjustment can effectively reduce target hot and cold spots and significantly improve target dose conformity and heterogeneity for Prowess RT Pro plans. All treatment plans show similar target dose maximum and minimum, but the MLC shape/weight adjustment improved D1% and D99% compared to the original plans. The target dose is less heterogenous for the MLC segment-adjusted plans in comparison to the original plans, while the dose conformity index (CI) is also improved after MLC leaf adjustments.
Table 2. Comparison of dose-volume parameters for the target and organs at risk for 15 patients previously treated for lung, liver and prostate cancers
|
Target/Organ |
Dose/Volume |
Original Plan |
|
New Plan |
|
Target |
Dmax (%Dp) |
112.5% (108.4%-119.1%) |
|
110.6% (109.4%-120.5%) |
|
Dmin (%Dp) |
98.5% (97.2%-99.0%) |
|
98.7% (97.9%-99.4%) |
|
|
CI |
1.07% (1.02%-1.13%) |
|
1.04% (1.01%-1.08%) |
|
|
Lung |
Dmean (cGy) |
480 (190-800) |
|
460 (170-780) |
|
V1350 (cc) |
440 (180-700) |
|
400 (150-660) |
|
|
Liver |
Dmean (cGy) |
1770 (1380-2190) |
|
1660 (1310-1980) |
|
Kidney |
Dmean (cGy) |
400 (0-800) |
|
350 (0-690) |
|
Bladder |
Dmean (cGy) |
2800 (1900-3620) |
|
2600 (1600-3550) |
|
V6500 (cc) |
14 (5-25) |
|
12 (3-23) |
|
|
V4000 (cc) |
33 (15-51) |
|
30 (11-50) |
|
|
Rectum |
Dmean cGy) |
3400 (2440-4420) |
|
2900 (2430-3450) |
|
V6500 (cc) |
15 (5-24) |
|
10 (6-16) |
|
|
V4000 (cc) |
43 (18-68) |
|
27 (20-34) |
This work investigated a new workflow that integrates ART into the routine IGRT workflow seamlessly. Using an independent ART system (e.g., the Prowess ART Workstation), this new workflow can be implemented on existing clinical accelerators equipped with advanced imaging systems (e.g., online CT, CBCT, MRI or in-room CT/MRI, etc.) that can provide high quality treatment geometry information for IGRT and ART applications. The new workflow employs the same treatment simulation and planning process as in routine IGRT. During a treatment session, the patient will be set up and imaged prior to treatment, and the patient’s anatomy will be compared with the planned dose distribution to decide whether ART is needed. If not, the patient will be treated as regular IGRT using the original treatment plan (i.e., the scheduled plan) with proper couch rotations/shifts. Otherwise, new target/OAR contours will be delineated, and an adaptive treatment plan will be generated and evaluated/approved. Independent dosimetry verification will be performed before and after the dose delivery for the adaptive plan. This is different from existing ART workflows (e.g., the Ethos CBCT-based ART), in which one must go through the entire ART workflow including re-contouring and re-planning even if the patient has minimal anatomy changes and can be treated satisfactorily using the original treatment plan (i.e., the scheduled plan). The new workflow allows efficient IGRT treatment and only initiates ART when necessary.
Two novel strategies were implemented in the new workflow to improve the ART effectiveness and efficiency. The first strategy employs an isodose-guided target localization technique to reduce the need for re-planning. As shown in the results section, this technique improved the target localization accuracy significantly and reduced the re-planning rate from 36.7% to 19.4% for 98 prostate fractions (Figure 4). The second strategy employs a two-tier treatment optimization process to improve planning efficiency and plan quality over the scheduled plan. Our results showed that many treatment fractions could be optimized using the simple DAO algorithm and minor MLC leaf adjustments to improve the heterogeneity index and conformity index for the target and most dose-volume parameters for organs at risk such as lung, liver, kidney, bladder and rectum (Table 2). Since the first-tier optimization uses a simple DAO algorithm to change the MLC segment shape and weight, it is more efficient (e.g., optimization in seconds) than the second-tier optimization, which calls for changes of the objective function and optimization parameters, and it is more frequently used in regular IGRT as most treatment fractions can be treated satisfactorily with the original plan with couch rotations/shifts or small modifications of the MLC shape/weight.
Online target alignment using rigid body registration with anatomy matching has received widespread clinical acceptance for IGRT [1-10,32-34], where couch shifts/rotations are initiated if the CTV on pretreatment images is outside the pre-specified safety margins (i.e., the PTV on simulation images). Our new target localization technique is conceptually different from the traditional anatomy-based target alignment because the prescription isodose surface does not always coincide with the surface of the PTV, and therefore target coverage is not guaranteed even if the pre-treatment CTV is enclosed by the original PTV contours. As discussed in detail previously [23], if the target dose distribution of a prostate treatment plan is normalized to give the prescription dose to 95% of the PTV, the prescription isodose surface may deviate by several millimeters from the surface of the PTV (i.e., 5% of the PTV receives doses less than the prescription dose). Therefore, it is more accurate to use the prescription isodose surface to localize the target directly than using the PTV, thus resulting in better target coverage. On the other hand, the CI of IMRT/SBRT plans are usually greater than 1, which means that the prescription isodose volume is larger than the PTV, thus it is more likely to enclose the CTV with the prescription isodose volume, reducing the need for adaptive replanning.
The difference of the patient anatomy as shown in images between the simulation CT and CBCT on the treatment day indicates a change in the optimization solution space even if one uses the same objective function/optimization parameters. It is expected that the adaptive plan is different from the scheduled plan, and hopefully it is also better than the scheduled plan in terms of the plan quality since it is optimized based on the patient anatomy on the treatment day. Due to the use of fast optimization algorithms in the ART systems (e.g., the widely used gradient descent algorithm, which is prone to getting stuck in local minima, especially in complex, non-convex problems [35]), however, it is sometimes observed that the quality of an adaptive plan is worse than that of the scheduled plan. Such an optimization outcome is understandable but not satisfactory (and in fact a disappointment) in the adaptive therapy process. Modifications are needed to improve both the re-planning efficiency and quality of current ART systems. For example, one can choose to start the search at a point closer to the global minimum (e.g., starting from the scheduled plan), or use hyperparameter tuning [36] to avoid getting stuck in local minima, or use stochastic gradient descent [37] to escape local minima. Simulated annealing has been used successfully with the DAO algorithm [24-29] for IMRT and VMAT plan optimization, which is flexible with the implementation of the two-tier optimization process for ART. For the first-tier optimization, only small changes in the MLC segment shape and weight are required and the random search will start from the scheduled plan in the nearby solution space. This ensures that the resulting adaptive plan quality is always better, or at least equal to the scheduled plan quality depending on the clinical acceptance criteria. The second-tier optimization is only needed for significant changes in the treatment geometry, which makes it difficult, if not impossible, for an adaptive plan to meet clinical acceptance criteria with the same objective function/optimization parameters. The opportunity to modify the objective function/optimization parameters opens the door to a new optimization solution space and the possibility to search for a solution closer to the global minimum, thus obtaining a more favorable adaptive plan. Such features have not been available in current ART systems.
CONCLUSIONS
This work investigates a new workflow that integrates adaptive radiotherapy into routine image-guided radiotherapy on existing clinical CBCT linacs, based on the Prowess ART system. The new workflow can improve the effectiveness and efficiency of radiotherapy treatment with the use of two new strategies, dose-guided target localization and two-tier treatment planning optimization. The former strategy can improve the target localization accuracy by better matching the target geometry with the isodose distribution, thus reducing the need for re-planning. The latter strategy can improve the optimization outcome to ensure the adaptive plan quality is better than or at least equal to the scheduled plan and achieving clinical goals for treatment scenarios with severe anatomical deviations from the original planning conditions.
ACKNOWLEDGMENTS
Technical support from Prowess Inc. is greatly appreciated for adaptive treatment planning and direct aperture optimization using the RT Pro TPS.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interests.
REFERENCES
- Paskalev K, Feigenberg S, Jacob R, McNeeley S, Horwitz E, Price R, et al. (2005). Target localization for post-prostatectomy patients using CT and ultrasound image guidance. J Appl Clin Med Phys. 6(4):40-49.
- Ma CM, Paskalev K. (2006). In-room CT techniques for image-guided radiation therapy. Med Dosim. 31(1):30-39.
- Chen L, Paskalev K, Xu X, Zhu J, Wang L, Price RA, et al. (2010). Rectal dose variation during the course of image-guided radiation therapy of prostate cancer. Radiother Oncol. 95(2):198-202.
- Foster RD, Solberg TD, Li HS, Kerkhoff A, Enke CA, Willoughby TR, et al. (2010). Comparison of transabdominal ultrasound and electromagnetic transponders for prostate localization. J Appl Clin Med Phys. 11(1):2924.
- Barney BM, Lee RJ, Handrahan D, Welsh KT, Cook JT, Sause WT. (2011). Image-guided radiotherapy (IGRT) for prostate cancer comparing kV imaging of fiducial markers with cone beam computed tomography (CBCT). Int J Radiat Oncol Biol Phys. 80(1):301-305.
- De Los Santos J, Popple R, Agazaryan N, Bayouth JE, Bissonnette JP, Bucci MK, et al. (2013). Image guided radiation therapy (IGRT) technologies for radiation therapy localization and delivery. Int J Radiat Oncol Biol Phys. 87(1):33-45.
- Dang A, Kupelian PA, Cao M, Agazaryan N, Kishan AU. (2018). Image-guided radiotherapy for prostate cancer. Transl Androl Urol. 7(3):308-320.
- Hall WA, Paulson ES, van der Heide UA, Fuller CD, Raaymakers BW, Lagendijk JJW, et al. (2019). The transformation of radiation oncology using real-time magnetic resonance guidance: A review. Eur J Cancer. 122:42-52.
- Hehakaya C, Van der Voort van Zyp JR, Lagendijk JJW, Grobbee DE, Verkooijen HM, Moors EHM. (2020). Problems and Promises of Introducing the Magnetic Resonance Imaging Linear Accelerator Into Routine Care: The Case of Prostate Cancer. Front Oncol. 10:1741.
- Grégoire V, Guckenberger M, Haustermans K, Lagendijk JJW, Ménard C, Pötter R, et al. (2020). Image guidance in radiation therapy for better cure of cancer. Mol Oncol. 14(7):1470-1491.
- Tong X, Chen X, Li J, Xu Q, Lin MH, Chen L, et al. (2015). Intrafractional prostate motion during external beam radiotherapy monitored by a real-time target localization system. J Appl Clin Med Phys. 16(2):5013.
- Park SS, Yan Di, McGrath S, Dilworth JT, Liang J, Ye H, et al. (2012). Adaptive image guided radiotherapy (IGRT) eliminates the risk of biochemical failure caused by the bias of rectal distension in prostate cancer treatment planning: clinical evidence. Int J Radiat Oncol Biol Phys. 83(3):947-952.
- Ma CM. (2011). Adaptive radiation therapy for prostate cancer, in Adaptive Radiation Therapy. In: Allen Li X, ed. CRC Press, New York, USA. pp. 331-350.
- Moazzezi M, Rose B, Kisling K, Moore KL, Ray X. (2021). Prospects for daily online adaptive radiotherapy via Ethos for prostate cancer patients without nodal involvement using unedited CBCT auto-segmentation. J Appl Clin Med Phys. 22(10):82-93.
- Ma CM, Lomax T. (2012). Proton and carbon ion therapy. New York, USA: Taylor & Francis.
- Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Kavanagh B, et al. (2010). Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 37(8):4078-4101.
- Ma CM. (2022). Physics and Dosimetric Principles of SRS and SBRT. Mathews J Cancer Sci. 4(2):22.
- Lagendijk JJW, Raaymakers BW, Van den Berg CAT, Moerland MA, Philippens ME, van Vulpen M. (2014). MR guidance in radiotherapy. Phys Med Biol. 59(21):R349-R369.
- Lamb J, Cao M, Kishan A, Agazaryan N, Thomas DH, Shaverdian N, et al. (2017). Online adaptive radiation therapy: implementation of a new process of care. Cureus. 9(8):e1618.
- Panetta JV, Eldib A, Meyer JE, Galloway TJ, Horwitz EM, Ma CMC. (2025). Experience and uncertainty analysis of CT-based adaptive radiotherapy for abdominal treatments. Phys Med. 131:104946.
- Lavrova E, Garrett MD, Wang YF, Chin C, Elliston C, Savacool M, et al. (2023). Adaptive Radiation Therapy: A Review of CT-based Techniques. Radiol Imaging Cancer. 5(4):e230011.
- Lee PL, Chen X, ElDib A, Galloway TJ, Hallman MA, Ma CC, et al. (2024). CT-Guided Adaptive Radiotherapy for the Treatment of Technically Challenging Oligometastatic Disease: A Case Report. Cureus. 16(10):e70765.
- Ma CMC, Shan G, Hu W, Price RA, Chen L. (2023). A new target localization method for image-guided radiation therapy of prostate cancer. Phys Med. 107:102550.
- Shepard DM, Earl MA, Li XA, Naqvi S, Yu C. (2002). Direct aperture optimization: a turnkey solution for step-and-shoot IMRT. Med Phys. 29(6):1007-1018.
- Ahunbay EE, Chen GP, Thatcher S, Jursinic PA, White J, Albano K, et al. (2007). Direct aperture optimization-based intensity-modulated radiotherapy for whole breast irradiation. Int J Radiat Oncol Biol Phys. 67(4):1248-1258.
- Broderick M, Leech M, Coffey M. (2009). Direct aperture optimization as a means of reducing the complexity of Intensity Modulated Radiation Therapy plans. Radiat Oncol. 4:8.
- Qi P, Xia P. (2013). Relationship of segment area and monitor unit efficiency in aperture-based IMRT optimization. J Appl Clin Med Phys. 14(3):4056.
- Cho PS, Marks RJ 2nd. (2000). Hardware-sensitive optimization for intensity modulated radiotherapy. Phys Med Biol. 45(2):429-440.
- Wu D, Eldib A, Chen L, Ma CM. (2025). MLC Leaf Adjustment for Direct-Aperture Optimization Treatment Planning. Mathews J Cancer Sci. 10(1):50.
- Oanh LT, Tai DT, Loan TTH, Minh TH, Minh TV, Chow JCL. (2019). Dosimetric evaluation of lung treatment plans produced by the Prowess Panther system using Monte Carlo simulation. Biomedical Physics & Engineering Express. 5(5):055005.
- Ma CM, Eldib A, Aslmarand SM, Chen L. (2024). Fraction-Modulated Dose Optimization for Advanced Radiation Therapy. Mathews J Cancer Sci. 9(1):47.
- Kontaxis C, de Muinck Keizer DM, Kerkmeijer LGW, Willigenburg T, den Hartogh MD, van der Voort van Zyp JRN, et al. (2020). Delivered dose quantification in prostate radiotherapy using online 3D cine imaging and treatment log files on a combined 1.5T magnetic resonance imaging and linear accelerator system. Phys Imaging Radiat Oncol. 15:23-29.
- Wang L, Feigenberg S, Fan J, Jin L, Turaka A, Chen L, et al. (2012). Target relocalization accuracy and PTV margin verification using three-dimensional cone-beam computed tomography (CBCT) in stereotactic body radiotherapy (SBRT) of lung cancers. J Appl Clin Med Phys. 13(2):41-54.
- Bohoudi O, Bruynzeel AME, Meijerink MR, Senan S, Slotman BJ, Palacios MA, et al. (2019). Identification of patients with locally advanced pancreatic cancer benefitting from plan adaptation in MR-guided radiation therapy. Radiother Oncol. 132:16-22.
- Chong EKP, Żak SH. (2013). "Gradient Methods". An Introduction to Optimization (Fourth ed.). Hoboken: Wiley. pp. 131-160.
- Bergstra J, Bengio Y. (2012). Random Search for Hyper-Parameter Optimization. Journal of Machine Learning Research. 13:281-305.
- Spall JC. (2003). Introduction to Stochastic Search and Optimization: Estimation, Simulation, and Control. Hoboken. NJ, USA: Wiley. pp. Sections 4.4, 6.6, and 7.5. ISBN: 0-471-33052-3.