Previous Issues Volume 4, Issue 2 - 2019
An In-Vivo Study on Pulsed Low-Dose-Rate Radiotherapy for Prostate Cancer
Bin Wang1,2, Jianhua Ren3, Peng Zhang4, Dusica Cvetkovic1, Xiaoming Chen1, Lili Chen1, and Chang-Ming Charlie Ma1
1Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, USA
2Department of Radiation Oncology, Temple University Hospital, Philadelphia, USA
3Department of Radiation Oncology, Taihe Hospital, Hubei University of Medicine, Shiyan, China
4Department of Radiation Oncology, Sichuan Cancer Hospital, Chengdu, China
Corresponding Author: Dr. C-M Charlie Ma, Ph.D., Department of Radiation Oncology, Fox Chase Cancer Center, 333 Cottman Ave, Philadlephia, PA 19111, E-mail: [email protected]
Received Date: Oct 15, 2019 Published Date: Nov 01, 2019
Citation: Ma CM. (2019). An In-Vivo Study on Pulsed Low-Dose-Rate Radiotherapy for Prostate Cancer. Mathews J Cancer Sci. 4(2): 21
ABSTRACT
Purpose: The objective of this study is to investigate the in-vivo tumor control efficacy of pulsed low-dose-rate (PLDR) radiotherapy for prostate cancer treatment.
Materials & Methods: We implemented three in vivo murine models of prostate cancer, namely an orthotopic LNCaP tumor model, a flank PC-3 tumor model, and an orthotopic PC-3 tumor model. The tumor-bearing mice were treated with a daily radiation dose of 2 Gy with either PLDR or at a conventional dose rate. The tumor growth was monitored with magnetic resonance (MR) imaging.
Results: For the orthotopic LNCaP tumor model and the flank PC-3 tumor model, we found that both PLDR and RT group tumors showed significant growth delay compared to the control group tumors. At two weeks after the first treatment, the difference between the mean tumor volume of the control group and the RT (PLDR) group was about 28% (25%) and 41% (43%) for the orthotopic LNCaP and flank PC-3 tumor models, respectively, with student t-test p values <0.05. However, there is no statistically significant difference between PLDR and RT groups. For the orthotopic PC-3 tumor model, we found that the PLDR treatment showed a better tumor control than conventional RT treatment. At two weeks after the first treatment, the difference between the mean tumor volume of the RT and the PLDR group tumors was about 31%, with student t-test p=0.02.
Conclusion: This study showed that PLDR could control prostate tumors at least as effectively as conventional RT. Considering that PLDR could also lead to much less normal tissue toxicity than conventional RT, we expect PLDR to be a viable modality for the management of recurrent prostate cancers.
Keywords: Pulsed low-Dose rate (PLDR); Radiation Therapy; Prostate Cancer; Invivo; Tumor Growth Delay.
INTRODUCTION
Prostate cancer tops the list of the most common cancers found in males in the United States. Currently, the standard curative treatment options for prostate cancer in the localized stages include radical prostatectomy, radiation therapy, and a combination of both. Although the local curative treatment with surgery or radiation is often associated with prolonged disease-free survival, unfortunately it has been estimated that about 20% ~ 30% of prostate cancer patients will experience disease recurrence after the 5-year mark [1]. For the recurrent prostate cancer patients, the current treatment options normally include chemotherapy with hormone management, immunotherapy, radiation therapy, and prostatectomy.
For the patients with recurrent cancers who have failed previous radiation treatments, however, there is no standard guideline for the re-irradiation with conventional radiotherapy techniques, because the normal tissues may have already received near-limit radiation toxicity [2-5] and it is very likely that the survived tumor cells are radiation-resistant [6]. Recently, a novel radiotherapy technique known as pulsed low dose rate (PLDR) or pulsed reduced dose rate (PRDR) external beam radiotherapy has been investigated for the re-irradiation of recurrent cancer patients [7-13]. The PLDR radiotherapy is often delivered as a series of 0.2 Gy radiation pulses with 3-minute intervals. The basic idea behind the technique is to take advantage of the low-dose hyper-radiosensitivity of the tumor cells and the increased repair of sublethal radiation damage to the normal tissues.
The low-dose hyper-radiosensitivity (HRS) is a well-known effect of rapidly proliferating cells exhibiting higher cell killing probability per unit dose of radiation when they receive radiation doses lower than certain transition doses (typically less than 0.4 Gy) [14]. A number of radiobiological studies have been conducted over the past decade to unveil the mechanism of HRS [15-18]. Current findings support the hypothesis that in the HRS regime the cells fail to undergo an early-G2-phase cell cycle arrest to recognize and repair small numbers of DNA double-strand break damage and in the subsequent cell cycles the cells die due to apoptosis in the G1 phase [18].
To investigate whether one could achieve any potential gain in the therapeutic ratio using PLDR technique for recurrent prostate cancer treatment, we implemented murine models of human prostate cancer cell lines, namely LNCaP and PC3, and evaluated the tumor control efficacy of PLDR treatment by monitoring the tumor growth using magnetic resonance imaging (MRI). In this study, we have found that the in vivo tumor control efficacy of PLDR treatment was at least not worse than that of the conventional radiation treatment (2 Gy radiation dose delivered continuously in one fraction). As indicated by our previous study and other published data, the normal tissue toxicity due to PLDR treatment could be much lower than that from the conventional radiation treatment [11,19]. Therefore, PLDR treatment could be a viable option for the treatment of recurrent prostate cancer.
METHODS AND MATERIALS
Prostate tumor models
For this study, we implemented three prostate tumor models using nude mice, namely, an orthotopic LNCaP tumor model, an orthotopic PC-3 tumor model, and a subcutaneous PC-3 tumor model. The human prostate cancer LNCaP and PC-3 cells were obtained from the American Type Culture Collection (ATCC, Manassas, VA) and cultured in RPMI-1640 medium, containing 10% fetal bovine serum (FBS), 1% L-glutamine, and 1% penicillin-streptomycin. Cells were maintained at 37ºC and in a humidified atmosphere of 5% CO2. Male athymic Balb/c nude mice (6 weeks old) were purchased from Harlan (Indianapolis, IN). Animal studies were carried out in compliance with a protocol approved by the Institutional Animal Care and Use Committee (IACUC) of Fox Chase Cancer Center (FCCC). Aseptic techniques were used for the injection of LNCaP and PC-3 prostate cancer cells in the mice. An anesthesia machine with flowing oxygen carrying 2% to 3% isoflurane (VEDCO Inc, Saint Joseph, MO) was used for inhalation anesthesia. For the orthotopic prostate tumor models, with the animals in supine position, a lower midline incision was made above the presumed location of the bladder. The seminal vesicles were brought out gently through the incision. The resulting exposed dorsal prostate lobes were injected with 106 cancer cells in 25 µl of media using a 1/2 mL U-100 insulin syringe with 28 G × 1/2 inch needle (Becton Dickinson, Franklin Lakes, NJ). The seminal vesicles were then restored to the abdominal cavity and the incision was sealed by suturing the muscle layer and using 2-3 wound clips for the skin layer. Buprenorphine 0.05 mg/kg to 0.1 mg/kg (Sigma Aldrich, St. Loius, MO) was given subcutaneously after the tumor implantation for pain relief. For the flank tumor model, the animals were placed in prone position. The skin on the back was lifted to separate it from the underlying muscle and 5 × 106 PC-3 cells in 150 µl of phosphate-buffered saline (PBS) were injected bilaterally subcutaneously.
Experiment design
Tumor-bearing mice were randomly assigned to one of three experimental groups: (1) PLDR group, which received 2 Gy/fraction radiation dose delivered in ten 0.2 Gy pulses with 3-minute intervals; (2) RT group, which received 2 Gy/fraction radiation dose delivered continuously; and (3) control group. The orthotopic LNCaP prostate tumors received one single fraction of treatment only, while the PC-3 orthotopic tumors were treated for 2 fractions separated by one week. The flank PC-3 tumors received 2 fractions of treatment on two consecutive days.
MR Imaging
The prostate tumor growth was monitored using a 1.5T GE MR scanner (GE Healthcare, Waukesha, WI). For MR scanning, the nude mice were anesthetized with an intramuscular (i.m.) injection of a mixed solution of ketamine (60 mg/kg) ((VEDCO Inc, Saint Joseph, MO) and ace-promazine (2.5 mg/kg) (Boehringer Ingelheim, Ridgefield, CT) in 15 µl volume, which was sufficient to immobilize the animal during MR scanning (approximately 15 min ~ 20 minutes).
A ring-shaped surface coil (with a diameter of about 8 cm) was used for the MR signal detection. T2-weighted MR images were acquired using fast-recovery fast-spin-echo (FRFSE) sequence with the following parameters: TR/TE = 2200/85 ms, NEX=3, matrix = 288 ´ 288, FOV = 7 ´ 7 cm2 (resolution = 0.243 ´ 0.243 mm2), and slice thickness = 2 mm and 1.2 mm for coronal and axial images, respectively.
External beam radiotherapy
The radiation treatment for the prostate tumors in the PLDR and conventional RT groups were delivered using a Siemens Artiste linear accelerator (Siemens Medical System, Malvern, PA). A 6 MV photon beam and a dose rate of 100MU/min were used. The mice were anesthetized with ketamine and ace-promazine and placed on the treatment table with either head-in-first supine position for the treatment of orthotopic tumors or head-in-first prone position for the flank tumors. Since the prostate tumor was very shallow, as compared to the depth of maximum dose for 6 MV photons, a piece of bolus was added on the top of the mouse skin to provide radiation dose buildup. The boluses were 10 mm thick for the treatment of orthotopic tumors and 15 mm thick for the flank tumors. The treatment couch position was adjusted so that the source surface distance (SSD) to the upper surface of the bolus was 100 cm.
Post-treatment tumor growth measurement
Following the treatment, the mice were scanned weekly for tumor growth monitoring with MRI. A high-resolution T2-weighted MR scan protocol developed specifically for our animal study (the parameters were described in the MR imaging section) enabled us to measure the tumor volume precisely. Both coronal and axial scans were performed and a slice thickness of 1.2 mm was used for axial MR scanning, which provided a resolution of 0.243 ´ 0.243 ´ 1.2 mm3 per voxel for the axial images. Tumor volume measurement was performed on the axial MR images using Philips Dicom Viewer software. We contoured the tumor on each slice of the images and the area was automatically calculated by the software. The total tumor volume was then calculated by summing up the tumor area on each axial MR image and multiplying the slice thickness (1.2 mm). The relative tumor volumes were calculated by normalizing the tumor volumes of each individual mouse at various time points to its volume on the first treatment day.
Statistical analysis
Measured tumor volumes were analyzed statistically. The mean and standard deviation of the mean (SDM) were calculated and the results were expressed as mean ± SDM. To determine if there was a significant difference between different groups, Student’s t-test was used and a p-value ≤ 0.05 was considered to be statistically significant.
RESULTS
The mice bearing orthotopic prostate LNCaP tumors in the conventional RT and PLDR groups received a total radiation dose of 2 Gy in one single fraction of radiation treatment. The mean tumor volumes on the treatment day were 95 mm3 ± 8 mm3, 112 mm3 ± 9 mm3, and 115 mm3 ± 8 mm3 for the control (n=7), RT (n=7), and PLDR (n=9) groups, respectively. The prostate tumor growth after the radiation treatment was compared with that of the control group tumors. In Figure 1, we show the MR images (the coronal slices with maximum tumor size) of three typical orthotopic prostate LNCaP tumors at various time points. The growth curves of the orthotopic LNCaP tumors are shown in Figure 2, from which we can clearly see that the conventional RT and PLDR treatment both significantly delayed the tumor growth, as compared with the untreated control group tumors. Furthermore, the results also show that the tumor growth delays of the RT and PLDR groups are comparable to each other. The difference between the mean normalized tumor volumes of the RT and PLDR groups is statistically insignificant with student t-test p=0.50, 0.34, and 0.31 at one, two, and three weeks after treatment, respectively.
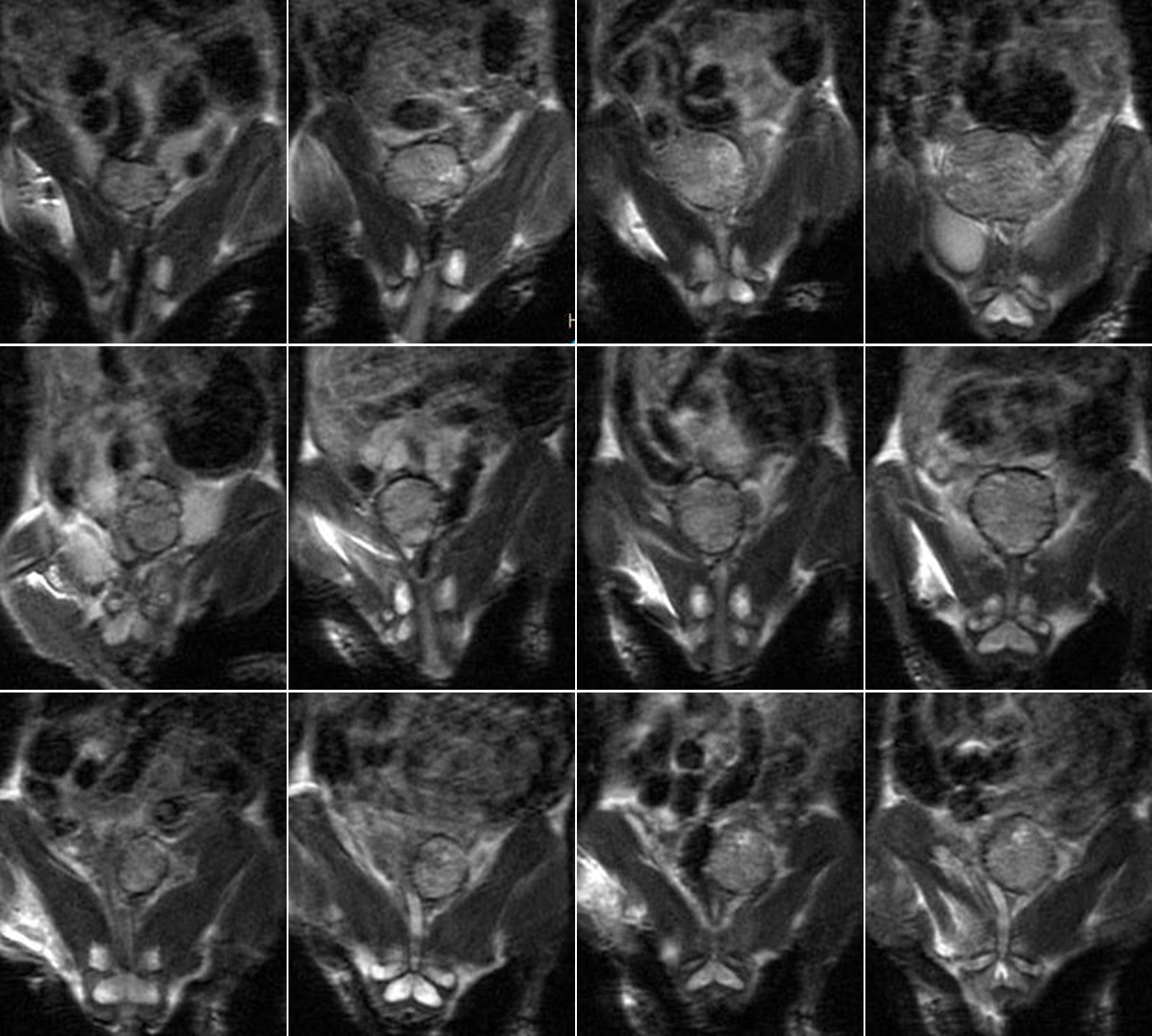
Figure 1: MR images for one control group LNCaP tumor (top row), one RT group LNCaP tumor (middle row), and one PLDR group tumor (bottom row) at various time points. From left to right: the 1st through the 4th columns correspond to the treatment day, one week, two weeks, and three weeks after treatment, respectively.
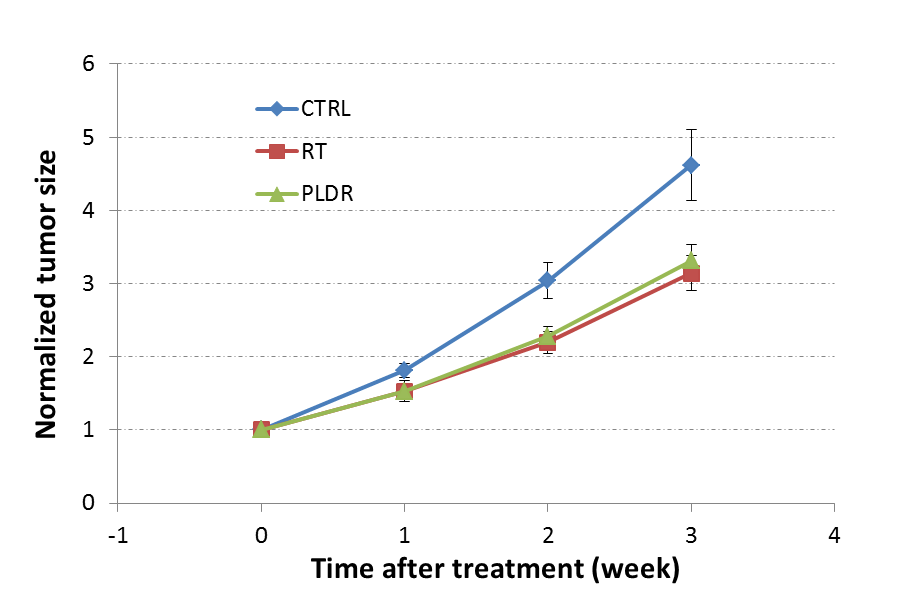
Figure 2: Normalized LNCaP tumor volumes of the control (n=7), RT (n=7), and PLDR (n=9) groups at various time points after treatment. The volume of each tumor was normalized to its initial tumor size on the treatment day.
The subcutaneous flank PC-3 tumors in the conventional RT and PLDR groups received 4 Gy of total radiation dose in two fractions of corresponding treatments on two consecutive days. The mean volumes on the first treatment day were 100 mm3 ± 9 mm3, 117 mm3 ± 13 mm3, and 100 mm3 ± 7 mm3 for the control (n=10), RT (n=6), and PLDR (n=7) group tumors, respectively. Figure 3 shows the growth curves of the flank PC-3 tumors. Both RT and PLDR treatments significantly inhibit the growth of the flank PC-3 tumors as compared with the control group tumors, similar to the above results of LNCaP tumors. Also, we did not find a statistically significant difference between the RT and PLDR groups with the subcutaneous PC-3 tumor model. The p values from the student t-test analysis of the RT and PLDR group data were p=0.47, 0.43, and 0.40 at one, two, and three weeks after the first treatment, respectively.
The RT and PLDR group mice bearing orthotopic PC-3 tumors were treated with 4 Gy total radiation dose in two fractions which are separated by one week. The mean volumes of the orthotopic PC-3 tumors on the first treatment day were 93 mm3 ± 11 mm3 and 84 mm3 ± 10 mm3 for the RT (n=7) and PLDR (n=7) groups, respectively. A comparison of the tumor growth between the RT and PLDR groups is presented in Figure 4. The difference between the two treatment groups is more significant than what we have seen in Figure 2 (orthotopic LNCaP tumor model) and 3 (flank PC-3 tumor model). The p values from the student’s t-test analysis for the RT and PLDR group tumor volume data were p=0.04, 0.02, and 0.08 at one, two, and three weeks after the first treatment, respectively. Moreover, we want to point out that for the last data points corresponding to three weeks after the first treatment in Figure 4, we had 4 and 6 mice in the RT and PLDR groups respectively, which is at least partly responsible for the dramatic increase in the statistical error for those data points. Furthermore, the difference in the survival between the two groups also indicates that the tumor control from the PLDR treatment was better than that from the RT treatment for the orthotopic PC-3 tumors.
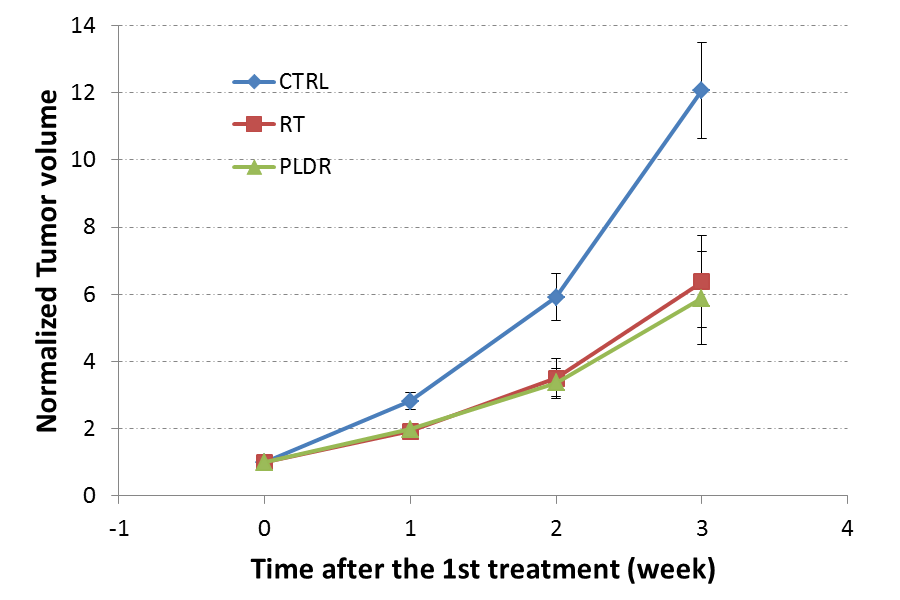
Figure 3: Normalized volumes of the control (n=10), RT (n=6), and PLDR (n=7) groups subcutaneously implanted PC-3 tumors at various time points after treatment.
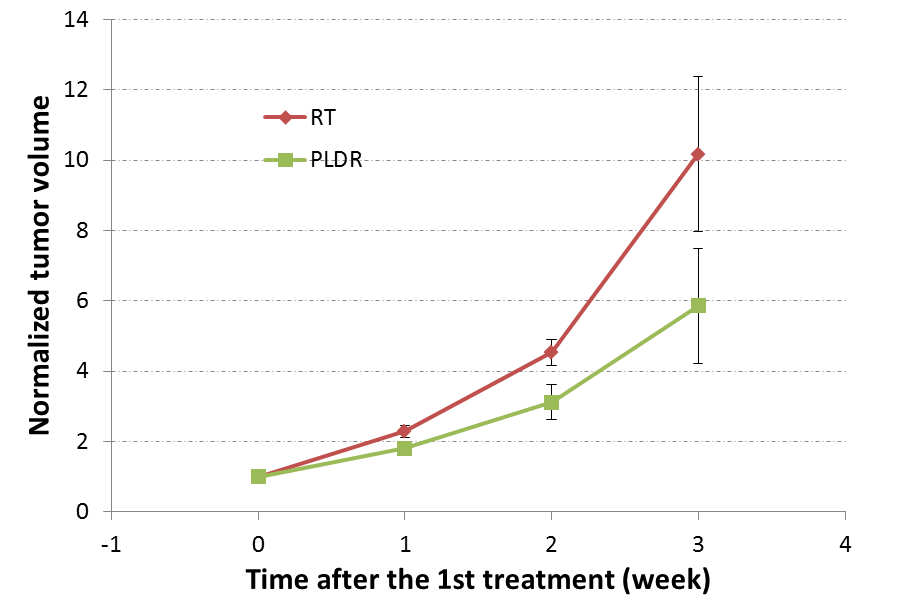
Figure 4: Normalized volumes of the RT and PLDR groups orthotopically implanted PC-3 tumors at various time points after treatment. From the 1st treatment day to two weeks after 1st treatment (the first three data points), both RT and PLDR groups had 7 tumors. However, for the last data points corresponding to three weeks after first treatment, we had n=4 and 6 for the RT and PLDR groups, respectively.
DISCUSSION
The PLDR treatment was designed to exploit the low dose HRS of the tumor cells. According to the in vitro data from the literature, low dose HRS has been found for both LNCaP and PC-3 cell lines [20]. However, the low dose HRS in vitro does not necessarily translate into better tumor control of PLDR in vivo, as suggested by our data (Figure 2). The low dose HRS might be suppressed for PLDR in vivo as the DNA damage repair mechanism could be activated due to accumulated pulsed doses or finite break time between the pulses. Our in vivo data in this study (Figures 2-4) also suggest that the tumors with a higher proliferation rate (i.e. PC-3 tumors in our case) might respond to PLDR treatment better than those with a lower proliferation rate (i.e. LNCaP tumors in this case). This finding is consistent with the current understanding about the low dose HRS cell killing mechanism, which has been associated with the avoidance of the G2 checkpoint of actively proliferating cells with a small amount of DNA damage. The difference between the data for orthotopic and flank PC-3 tumors suggests that the tumor microenvironment may play an important role in the HRS effect in PLDR. Nevertheless, our results demonstrate that the PLDR treatment with 10 0.2 Gy-pulses and 3 minutes inter-pulse interval shows at least comparable tumor control as compared with conventional RT for different tumor models.
It has been shown in previous studies that the PLDR treatment could better spare normal tissue [11,19]. For example, in a study using an orthotopic murine model of human glioblastoma multiforme, the pulsed regimen was found to lead to less neuronal death than the standard fractionation regimen [11]. We have also recently conducted a study to perform total body irradiation (TBI) for mice with PLDR or conventional RT [19]. A significant difference in mice survival time and toxicities to spleen and bone marrow was found between the PLDR and conventional RT groups in the TBI study. Since our current study demonstrates that the in vivo tumor control efficacy of the PLDR treatment is at least comparable to that of the conventional RT treatment for prostate cancer, we anticipate to gain in the therapeutic ratio for treating recurrent prostate cancer with PLDR, considering the additional benefit of less normal tissue toxicity from PLDR.
Treatment planning strategies for PLDR treatments of recurrent cancers utilizing advanced delivery techniques including intensity-modulated radiation therapy (IMRT) and volumetric-modulated radiation therapy (VMAT) have been developed recently by our group [21-24]. The IMRT and VMAT treatment plans for our PLDR patients exhibited significantly improved target dose conformity and organ at risk dose sparing. Currently, clinical trials for PLDR using IMRT or VMAT techniques are ongoing for the management of recurrent cancers at Fox Chase Cancer Center.
CONCLUSION
In this study, we performed in vivo experiments to study the efficacy of PLDR treatment for the management of prostate cancer. Three murine models of human prostate cancer, namely an orthotopic LNCaP tumor model, a flank PC-3 tumor model, and an orthotopic PC-3 tumor model, were implemented for this study. For the orthotopic LNCaP tumor model and the flank PC-3 tumor model, we found that both PLDR and RT group tumors showed significant growth delay as compared to the control group tumors. However, for these two tumor models, there is no statistically significant difference in the tumor growth delay between PLDR and RT group tumors. For the orthotopic PC-3 tumor model, we found that the PLDR treatment showed a better tumor control than conventional RT treatment. In summary, the PLDR treatment could control prostate tumors at least as effectively as conventional RT as shown by our in vivo experiments. Considering that PLDR could also lead to much less normal tissue toxicity than conventional RT, we expect PLDR to be a viable modality for the management of recurrent prostate cancers.
Acknowledgements
The authors would like to thank Doctors Joshua Meyer, Wei He, Wenguang Luo, and Pindong Li for valuable discussions. We would also like to thank Ms. Lorraine Medoro for her assistance in editing and proofreading the manuscript.
REFERENCES