Previous Issues Volume 1, Issue 1 - 2016
Can Ultrasound Elastography Substitute Tissue Biopsy in the Diagnosis of Malignancy?
Feril LB1,Hata T2,Tachibana K1
Department of Anatomy, Fukuoka University School of Medicine, Fukuoka, Japan
2Department of Perinatology and Gynecology, Kagawa University Graduate SchoolofMedicine, Kagawa, Japan
Corresponding Author: Loreto B. Feril, Department of Anatomy, Fukuoka University School of Medicine, Fukuoka, Japan. Tel: +81-76-434-7265; E-Mail: [email protected]
Received Date: 10 Feb 2016 Accepted Date: 16 Feb 2016 Published Date: 24 Feb 2016
Copyright © 2016 Feril LB
Citation: Feril LB. (2016). Can Ultrasound Elastography Substitute Tissue Biopsy in the Diagnosis of Malignancy? Mathews J Cancer Sci. 1(1): 004.
ABSTRACT
Ultrasonography, or imaging by ultrasound, is one of the most commonly utilized diagnostic procedures today. This is despite the introduction of many other alternative diagnostic methods. The reasons include ultrasound being non-ionizing (unlike X-rays and CT scans), non-invasive (unlike tissue biopsies), less expensive and more commonly available (unlike MRI and genetic tests). In addition, new ultrasound technologies have also made ultrasonography more reliable and agile, thus offering additional diagnostic capabilities. One of these new technologies is the so-called "ultrasound elastography".
INTRODUCTION
We casually judge a material as “hard” or “soft” by applying pressure while touching it. In medicine, clinicians palpate the patient's body to determine if certain tissue feels normal, unusually hard or unusually soft, to get possible signs of disease or disorder. However, palpation is highly subjective and therefore can be unreliable. For example, lesions that are very small and those that are located deep into the body may not be detectable by palpation alone. Also, the degree of hardness between different pathologies may not be distinct enough that can be appreciated by our sense of touch despite extensive training and experience. Although in some cases, abnormal growths can be easily judged as hard tumor or cystic tumor based on their hardness and on their echo pattern during conventional ultrasound imaging, to differentiate one type of solid tumor to the others based on degree of hardness can be difficult. Such distinction is particularly important in clinically differentiating deadly malignant tumors from the benign ones because early detection and intervention of malignant lesions can be life-saving. A newly introduced ultrasound technology provides a noninvasive way to accurately diagnose a malignant tumor based on its characteristic hardness. This technology is being utilized in a diagnostic procedure that grades tissue elasticity using ultrasound, more often called "ultrasound elastography".
Basic Principle of Ultrasonography
Use of ultrasound in diagnosis has been one of the oldest of the "modern technologies" available to medicine today. Imagingwith the use of ultrasound, also called ultrasonography or echography, is considered one of the safest and cost-effective real-time imaging that is widely used today not only for diagnosis but also as an instrument useful in interventional medicine. The imaging works when ultrasound waves, usually at frequencies between 2 and 10 MHz, is applied on the part of the body and the reflected sound waves (or echo), collected by the receiver and then analyzed by the computer, give a picture of tissue along its path. The varying tissue densities will results in varying impedances that will in turn give a varying echo signals and hence the formation of an image. Some tissue will have characteristic echo patterns that will help guide sonographers to identify landmark structures and detect possible anatomical anomalies and other abnormalities.
The Physics behind Elastography
Tissues that are very reflective of ultrasound tend to block ultrasound from getting an image of the tissue beyond that region while a tissue with very low impedance tends to dissipate ultrasound and prevent it from having enough echoes. These are true with hard tissues such as bones and gas filled structures such as the lungs. Some calcified lesions and tumors may also have some hard outer shells that could reflect ultrasound. These types of lesions would create artifacts that distort the echo-pattern. To address this imaging issue, elastography has been introduced. The term "elastography" is coined for this particular method that determines the level of tissue elasticity and display them as images based on the degree of elasticity. those indicator pathogens that recommended for quality evaluation of raw materials and finished products by different pharmacopoeia. These procedures include cultivation, morphological and biochemical characterization of isolates [1]. Microbial identification methods can be divided into several groups (Table 1).
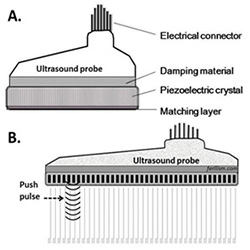
Figure 1:Phased-array transducers. A. A typical ultrasound transducer for imaging. B. Ultrasound transducer fitted with a pulsing mechanism for elastography.
In this new technology, a couple of methods to elicit elastographic images from a sonographic device are being used. One is by manually applying pressure using the ultrasound probe while another is by using an specially designed ultrasound probe capable of sending strong pulses that would compress the tissue while ultrasound imaging device monitors the tissue response to that compression (See Figure 1). The elasticity of the tissue is then gauged based on the movement of every particle in the ultrasound field in
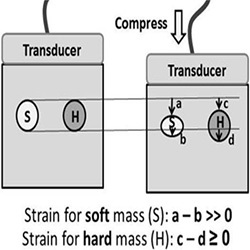
Figure 2:Calculating strain. The effect of manual compression on soft (S) or hard lesions (H) within the soft tissue and how strain or elasticity is being calculated.
response to the pulses (See Figure 2). Elastographic image will then be displayed either as gray-scaled or color-coded images based on the level of compressibility, thus allowing a more accurate image depicting hardness of the lesion relative to the surrounding normal tissue. Several clinical studies have shown the value of this method in differentiating suspected lesions.
Elastography in the Diagnosis of Malignancies and Other Lesions
Currently, several ultrasound devices from different companies have elastography functions. The main application of elastography is in the diagnosis of certain cancers; particularly cancers in the liver, breast, thyroid, and prostate (See Table 1) [1]. This ultrasound function is capable of identifying a tumor lesion to be either malignant or not, with a reliability comparable to tissue biopsy [2]. The latter being the current gold standard. Elastography has also the ability to delineate the actual size of the lesion (See Figure 3), more accurately than ordinary sonography. Studies have shown that with elastography, ultrasound imaging can diagnose the extent of breast tumors and are able to detect its state of malignancy.
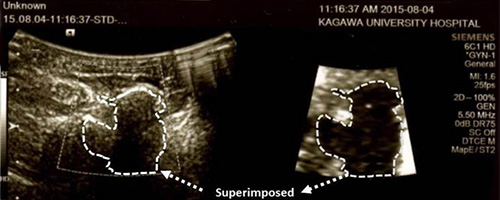
Figure 3:Ultrasound images of a breast lesion. Image of the lesion shown using B-mode with basic ultrasound imaging (left) and elastographic imaging of the same lesion (right). Broken white line delineates the “hard lesion” shown by elastography and then superimposed on the basic ultrasound image on the left for comparison
Considering the nature of ultrasonography, which is noninvasive and devoid of pain compared to tissue biopsy, with elastography it can also be a better alternative in identifying the grade of liver lesions. This is particularly useful in lesions such as liver fibrosis and cirrhosis which are currently diagnosed by tissue biopsy [3,4]. With tissue biopsy, a small part of the liver lesion is either surgically excised or taken using a large bore needle for microscopic analysis. Complications such as bleeding and infection, in addition to pain, are possible. These complications associated with tissue biopsy are absent with elastography, thus making elastography a safer and advantageous alternative. In most cases though, elastography may not be enough to make a diagnosis of a lesion's malignancy, but this will likely compliment diagnostic results from other methods to come up with a more accurate diagnosis. In addition, initial information provided by elastography may also help reduce the number of unnecessary biopsies.
| Organ/Tissue | Malignancy/Lesion |
|---|---|
| Liver | Hepatocellular carcinoma (HCC) [5], Cirrhosis [6], Liver fibrosis[7], Liver-related events [8], Liver tumors [9] |
| Thyroid | Thyroid nodules [10-14], Thyroid cancer [15,16], Hashimoto's thyroiditis [17] |
| Breast | Breast cancer [18-20], Breast lesions [3,21,22] |
| Prostate | Prostate cancer [23,24] |
| Superficial soft tissue | Superficial soft tissue lesions [25] |
| Testicles | Testicular tumor [26] |
| Rectum | Rectal cancer [27] |
| Pancreas | Pancreatic masses [28,29] |
| Lymph node | Lymph nodes [30] |
| Brain | Brain tumor [31] |
Table 1:Clinical studies related to the use of ultrasound elastography in the diagnosis of cancers and other lesions.
The Future of Ultrasound Elastography
With the rapid advances in this technology, ultrasound elastography will likely become a common feature in all ultrasonographic devices. Further studies in this field will certainly find more applications for such technology, not only in the diagnosis of cancer and liver lesions, but in many other fields in medicine and related sciences.
REFERENCES
- Ueno E, Tohno E, Morishima I, Umemoto T, et al. (2001). J Med Ultrason. 42(4), 521-531.
- Fausto A, Rubello D, Carboni A, Mastellari P, et al. (2015). Clinical value of relative quantification ultrasound elastography in characterizing breast tumors. Biomedicine & pharmacotherapy. 75, 88-92.
- Barr RG, Ferraioli G, Palmeri ML, Goodman ZD, et al. (2015). Elastography Assessment of Liver Fibrosis: Society of Radiologists in Ultrasound Consensus Conference Statement. Radiology. 276(3), 845-861.
- Guibal A, Renosi G, Rode A, Scoazec JY, et al. (2016). Shear wave elastography: An accurate technique to stage liver fibrosis in chronic liver diseases. Diagnostic and interventional imaging. 97(1), 91-99 .
- Kim MN, Kim SU, Kim BK, Park JY, et al. (2015). Increased risk of hepatocellular carcinoma in chronic hepatitis B patients with transient elastography-defined subclinical cirrhosis. Hepatology. 61(6), 1851-1859.
- Wang JH, Chuah SK, Lu SN, Hung CH, et al. (2014).Baseline and serial liver stiffness measurement in prediction of portal hypertension progression for patients with compensated cirrhosis. Liver International. 34(9), 1340-1348.
- Bohte AE, van Dussen L, Akkerman EM, Nederveen AJ, et al. (2013). Liver Fibrosis in Type I Gaucher Disease: Magnetic Resonance Imaging, Transient Elastography and Parameters of Iron Storage. PloSONE. 8(3), e57507.
- Park MS, Kim SU, Kim BK, Park JY, et al. (2015). Prognostic value of the combined use of transient elastography and fibrotest in patients with chronic hepatitis B. Liver International. 35(2), 455-462.
- Kato K, Sugimoto H, Kanazumi N, Nomoto S, et al. (2008). Intra-operative application of real-time tissue elastography for the diagnosis of liver tumours. Liver International. 28(9), 1264-1271.
- Korkusuz H, Happel C, Klebe J, Ackermann H, et al. (2015). Diagnostic accuracy of elastography and scintigraphic imaging after thermal microwave ablation of thyroid nodules. Europe PMC. 187(5), 353-359.
- Calvete AC, Mestre JD, Gonzalez JM, Martinez ES, et al. (2014). Acoustic Radiation Force Impulse Imaging for Evaluation of the Thyroid Gland. Journal of ultrasound in medicine. 33(6), 1031-1040.
- Liu BX, Xie XY, Liang JY, Zheng YL, et al. (2014). Shear wave elastography versus real-time elastography on evaluation thyroid nodules: A preliminary study. European journal of radiology. 83(7), 1135-1143.
- Cakir B, Ersoy R, Cuhaci FN, Aydin C, et al. (2014). Elastosonographic strain index in thyroid nodules with atypia of undetermined significance. Journal of endocrinological investigation. 37(2), 127-133.
- Chong Y, Shin JH, KoES and Han BK.(2013). Ultrasonographic elastography of thyroid nodules: is adding strain ratio to colour mapping better? Clinical radiology. 68(12), 1241-1246.
- Vidal-Casariego A, Lopez-Gonzalez L, Jimenez-Perez A, Ballesteros-Pomar MD, et al. (2012). Accuracy of ultrasound elastography in the diagnosis of thyroid cancer in a low-risk population. German Society of Endocrinology. 120(10), 635- 638.
- Trimboli P, Guglielmi R, Monti S, Misischi I, et al. (2012). Ultrasound Sensitivity for Thyroid Malignancy Is Increased by Real-Time Elastography: A Prospective Multicenter Study. The Journal of Clinical Endocrinology and Metabolism. 97(12), 4524-4530.
- Yildirim D, Gurses B, Gurpinar B, Ekci B, et al. (2011).Nodule or Pseudonodule? Differentiation in Hashimoto's Thyroiditis with Sonoelastography. The Journal of international medical research. 39(6), 2360-2369.
- Lee SH, Moon WK, Cho N, Chang JM, et al. (2014). Shearwave elastographic features of breast cancers: comparison with mechanical elasticity and histopathologic characteristics. InvestRadiol. 49(3), 147-155.
- Tamaki K, Tamaki N, Kamada Y, Uehara K, et al. (2013). A Non-invasive Modality: The US Virtual Touch Tissue Quantification (VTTQ) for Evaluation of Breast Cancer. Japanese Journal of Clinical Oncology. 43(9), 889-895.
- Chang JM, Moon WK, Cho N, Yi A, et al. (2011). Clinical application of shear wave elastography (SWE) in the diagnosis of benign and malignant breast diseases. Breast Cancer Res Treat. 129(1), 89-97.
- Cebi OD, Korkmazer B, Kilic F, Dikici AS, et al. (2014).Use of shear wave elastography to differentiate benign and malignant breast lesions. DiagnIntervRadiol. 20(3), 239-244.
- Moon WK, Chang SC, Huang CS and Chang RF. (2011). Breast Tumor Classification Using Fuzzy Clustering for Breast Elastography. Ultrasound in Medicine &Biology. 37(5), 700- 708.
- Xu G, Feng L, Yao M, Wu J, et al. (2014). A new 5-grading score in the diagnosis of prostate cancer with real-time elastography.IntJ ClinExpPathol. 7(7), 4128-4135.
- R. Ganzer, A. Brandtner, Wieland WF and Fritsche HM. (2012). Prospective blinded comparison of real-time sonoelastography targeted versus randomised biopsy of the prostate in the primary and re-biopsy setting. World journal of urology. 30(2), 219-223.
- Magarelli N, Carducci C, Bucalo C, Filograna L, et al. (2014). Sonoelastography for qualitative and quantitative evaluation of superficial soft tissue lesions a feasibility study. European radiology. 24(3), 566-573.
- Jedrzejewski G, Ben-Skowronek I, Wozniak MM, Brodzisz A, et al. (2013). Testicular adrenal rest tumors in boys with congenital adrenal hyperplasia: 3D US and elastography-- do we get more information for diagnosis and monitoring?J Pediatr Urol. 9(6 Pt B), 1032-1037.
- Rafaelsen SR, Vagn-Hansen C, Sorensen T, Lindebjerg J, et al. (2013). European journal of radiology. 82(6), 913-917.
- Dawwas MF, Taha H, Leeds JS, Nayar MK, Oppong KW, et al. (2012). Diagnostic accuracy of quantitative EUS elastography for discriminating malignant from benign solid pancreatic masses: a prospective, single-center study. Gastrointestinal Endosc. 76(5), 953-961.
- Saftoiu A, Vilmann P, Gorunescu F, Janssen J, et al. (2011). Accuracy of endoscopic ultrasound elastography used for differential diagnosis of focal pancreatic masses: a multicenter study. Endoscopy. 43(7), 596-603.
- Larsen MH, FristrupCW and Mortensen MB. (2011). Intraand interobserver agreement of endoscopic sonoelastography in the evaluation of lymph nodes.Ultraschall Med 32 Suppl 2, E45-50.
- Scholz M, Noack V, Pechlivanis I, Engelhardt M, et al. (2005). Vibrography during Tumor Neurosurgery. Journal of Ultrasound in Medicine. 24(7), 985-992