Information Links
Related Conferences
Previous Issues Volume 7, Issue 4 - 2023
Vaccination Versus Risk Identification & Risk Management: The Role of Risk Communication in Disease Outbreaks
Jos Noordhuizen*
School of Agriculture and Veterinary Science, Charles Sturt University, Boorooma Street, North Wagga, Australia
*Corresponding author: Jos Noordhuizen, DVM, PhD, Former Diplomate at EC BHM and VPM, former professor at Universities of Utrecht and Wageningen (The Netherlands), and School of Agriculture and Veterinary Science, Charles Sturt University, Boorooma Street, North Wagga, Australia; E-mail: [email protected].
Received Date: September 04, 2023
Published Date: September 22, 2023
Citation: Noordhuizen J. (2023). Vaccination Versus Risk Identification & Risk Management: The Role of Risk Communication in Disease Outbreaks. Mathews J Vet Sci. 7(4):26.
Copyrights: Noordhuizen J. © (2023).
ABSTRACT
In this paper, major domains of veterinary preventive medicine are addressed: applying vaccines and implementing risk identification & risk management plans. Both should go together on animal production farms because they are mutually beneficial. Moreover, the potential risk of economic losses may be drastically lowered. Both domains are briefly highlighted. A dairy farm is used for illustration purposes. Moreover, the role of professional risk communication is addressed for cases of an epidemic disease outbreak. The reason is that risk communication is not at all comparable to the marketing kind of communication. The latter is unfortunately often used for communication with the people in case of such outbreaks. The example is COVID-19.
Keywords: COVID-19, Biosecurity Plans, Animal Production, Pig Farms, Vaccination, Bacteria.
INTRODUCTION
Animal production these days cannot function without vaccines, not in the least because of the high animal density in animal production farms, and the often lack of biosecurity plans on these farms [1]. The most important representatives of animal production farms are the intensive poultry and pig farms around the world and to a lesser extent cattle production. Vaccination plans are part of veterinary preventive medicine programs and cover a wide spectrum of micro-organisms, such as viruses, bacteria, and endo- or ectoparasites.
Preventive medicine, however, should also cover risk identification and risk management. This is a highly relevant domain given that most diseases and disorders in, for example, dairy cattle herds, have a multifactorial background. In this background, risk factors from the cows’ environment such as housing, barn climate, feed, and at the cow level such as the level of genetic disease resistance, metabolism, age, milk production level may play a substantial role in the occurrence of these diseases [2,3].
Veterinary preventive medicine in practice should address both domains: the animal health promotion through vaccination and through risk identification & management.
This chapter addresses both domains, with the example of dairy cattle for illustration purposes. Moreover, special attention is given to emergency risk communication [4], using the French example of the COVID-19 epidemic.
Veterinary preventive medicine --Vaccines
During a veterinary herd health program for dairy farms, the veterinarian addresses different domains of dairy farming, like reproductive performance, milk production & nutrition, and animal health and welfare. Part of the animal health program is the design of vaccination plans, tailor-made for each farm. These plans may cover a broad spectrum of micro-organisms, depending on local conditions [1].
For dairy cattle farms such plans may comprise, for example, starting at young calf level and related to the age of the calves, the different vaccines as named in Table 1.
Table 1. An example of a youngstock vaccination plan on a dairy farm (Noordhuizen, 2012). IBR= infectious bovine respiratory disease (Herpes virus); BVD= Bovine virus diarrhea; Brucellosis= Brucella abortus.
|
Age in days |
Type of vaccine or drug |
|
15 |
Pasteurellosis |
|
30 |
Clostridium enterotoxemia |
|
45 |
Pasteurellosis |
|
60 |
Clostridium enterotoxemia |
|
75 |
Anti-parasiticum |
|
90 |
Anti-parasiticum |
|
120 |
IBR, Parainfluenza 3, BVD |
|
150 |
IBR, Parainfluenza 3, BVD |
|
180 |
Brucellosis |
It is highly advisable that a veterinarian evaluates what the results of vaccination are, using parameters such as monthly and yearly disease incidence, milk production performance, the occurrence of other (non-vaccine related) disorders, total cost-benefit analysis results. Unfortunately, this is not a common rule everywhere, and -hence- there is room for improvement.
Veterinary preventive medicine--Risk Identification and Risk Management
As stated earlier, risk identification & risk management is the second domain of veterinary preventive medicine. In the author’s experience this domain is largely neglected in the veterinary and professional dairy world. In fact, this domain should be part of any dairy herd health program, irrespective of whether vaccines in a biosecurity plan are being applied or not [1,8].
The reason is simple: by implementing risk management plans within a dairy herd health program [1], the operational level of the latter is complemented by the first, more tactical in nature. Given the multifactorial nature of animal disease, implicating many contributory risk factors, this approach is crucial (Table 2). In both dairy herd health programs and dairy farm audits [9] optimal professional communication between farmer and veterinarian is paramount.
Table 2. A short overview of risk factors associated with BVD in dairy cattle [3,10]
|
New cattle entering the farm |
Calving of a cow |
|
No quarantine facilities are present |
Sick animals group pen |
|
No BVD-testing is done prior to entry |
Waste milk is fed to calves |
|
Live contacts are possible (wildlife) |
Farm equipment and tools |
|
(Professional) People visiting the farm |
Cars, trucks |
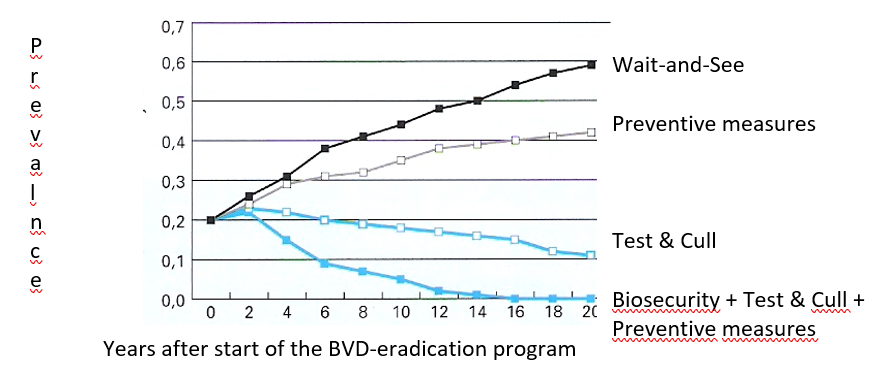
Figure 1. Example of results of different risk management strategies for combatting Bovine Virus Diarrhea at regional level [10]
From the graph in Figure 1 one can read that the infectious disease BVD can be eradicated on the long run by combining different appropriate strategies and even without vaccination. Here again, professional communication plays a key role [7,11].
Risk identification and risk management can be applied at the level of the individual farm, but also at regional level and even nation-wide. The latter often relates to trade barriers when a certain country does not wish to import dairy products or live cattle from a country with a BVD-prevalence. Several European countries have, for example, successfully implemented nation-wide BVD-control and monitoring programs for that reason. These programs are usually made compulsory for dairy farmers.
The role of emergency risk communication in epidemic disease outbreaks
- Major elements in developing Risk Identification & Risk Management Plans
Risk Identification has its origin in epidemiology: hazards (infectious diseases) are to be identified, as well as their associated risk factors or risk conditions. But it goes beyond that, because also non-infectious diseases, impaired welfare and public health issues may be addressed [3,12].
When developing a risk identification plan, there are seven major steps to follow. These steps are described in Table 3.
Table 3. Developing a risk identification plan for a dairy cattle farm: 7 major steps [3].
|
Major steps in developing a risk identification plan |
|
1—Conduct a critical inventory of infectious diseases representing a threat for the farm, considering the geography, soil type, water streams, housing system, animals, people, visitors to the farm, transports Identify risk factors and their priority and feasibility of control |
|
2—Identify the most important infectious diseases prevalent on the farm, together with the farmer. Identify the risk factors and their priority and feasibility |
|
3—Conduct a clinical inspection of the herd and its environment incl. management, as well as the farm data to determine the transmission risks of pathogens. |
|
4-- Formulate goals: for example, less than 10% of mastitis cases in the cows. Or, eliminating Salmonella spp prevalence from the herd in 3 years’ time |
|
5—Write down on paper, in a concise manner, the results of the preceding steps |
|
6—Design an Action Plan with priorities and secondary measures; implement it |
|
7—Evaluate each period (3 or 6 monthly) the effects of the action plan; adjust when deemed necessary. |
Moreover, an adequate professional communication is another keyword for success. The veterinarian should act as a coach to the farmer, to guide him along the path to success [5,6,11]. Discussions between both take place at the level of equality: each has his own knowledge, experience, and skills as input.
In all circumstances, the risk management plan must be practical, easy to understand for everybody, concise in format and flexible to changing conditions.
Table 4 presents a non-exhaustive overview of areas of concern, when developing a Risk identification plan [3].
Table 4. An overview of areas of concern when developing a Risk Identification plan, together with details and management actions to counteract or eliminate the respective risks [3,8].
|
Areas of concern and Management actions to be taken |
||
|
Area of concern |
Details |
Actions |
|
New additions to the herd |
Cattle, semen, embryos |
Check all animals. Test for relevant diseases. Sample milk for bacteriology. Vaccinate 2x before transport. Quarantine the cattle for 3 wks before mixing with the herd. Buy semen or cattle from health-certified farms. |
|
Forages & Concentrates, Drinking water |
Salmonella spp may be found in feed and in pasture grass and in water. E. coli and Cryptosporidium may be found in water. |
Test water on bacteriological, chemical, and nutritive contamination. Feed traders should show their health or quality certificates. Prevent contamination of feed and water by feces or urine. |
|
Animal contacts |
Presence of fences. No participation in cattle shows. Separate sick cattle. Specific calving pens
|
Minimize contacts between cattle age groups. Cattle returning from shows are to be considered as new additions to the herd. Avoid on-resident cattle. |
|
Wildlife and other vectors |
Rats, mice, squlrrels, foxes (Salmonella spp,Brucella sp, E. coli, Leptospira spp) Insects (Anaplasmosis, Blue Tongue) Dogs, cats, birds |
Prevent all contact with wildlife Apply insecticides and traps close to the feed. Avoid birds, dogs and cats to enter in barns. |
|
Animal health management |
Apply Good Medicine Application Code of Practice |
|
|
Noxae |
Vehicles & persons |
Both professional and non-professional people are a risk |
- Risk Communication elements
A final issue concerns, for example, human medicine and the COVID-19 pandemic. In several countries, such as in Europe, one has started too late with vaccination or confinement, while at the same time there was too little attention for risk identification & risk management. Risk= Hazard (virus transfer) x Exposure (to virus); the outcome is a probability.
Moreover, the domain of (emergency) risk communication was largely forgotten or even falsely implemented [13].
Risk communication must deal with people’s perceptions, fear, uncertainty, confinement stress and credibility of information and its providers. Hence, professionals are needed for this job. Covello (2003) [4] presented Best Practices with guidelines for developing and applying Emergency Risk Communication. In Annex 1, seven cardinal guidelines for ‘’best practices’’ in emergency risk communication are presented [4].
Too often government members and other authorities spoke about a ‘’war’’ or from a purely marketing communication point of view, while the latter has no association whatsoever with emergency risk communication in situations of disasters like pandemics or environmental disasters. It should be a must and target to educate officials in appropriate risk communication. The reasons for this need are presented in Table 5 [13].
Table 5. Examples of using ‘’marketing type of communication’’ in the COVID-19 epidemic in France instead of using emergency risk communication [13]
|
Which actions? |
Communication (citations) |
Comments (authors) |
|
Announcement of the pandemic by the President (Day 1) |
(We are at war!) |
Creates fear, hence counterproductive. People are not soldiers with weapons in hands! |
|
Announcement by the Minister of Public Health (Day 2) |
(Mouth masks are useless) |
But what is? |
|
,, (Day 3) |
(Mouth masks are not available at all) |
Now, are they useless or useful? |
|
,, (Day 5) |
(Mouth masks are useful) |
Time lost for proper reliable information. Loss of credibility |
|
Creation of a Scientific Committee by the President |
(I have chosen committee members of high scientific quality standards) |
Members have no competence in Corona virus or mass disease outbreaks. There is no member with applied epidemiological mathematical modelling competence on board |
|
Several Ministers talk on TV, even when Public Health is not their domain |
Communication varies and sometimes need to be corrected by the President the next day |
There is not one spokesperson. Who can people trust? |
|
Several TV stations invite self-named ‘’specialists’’ |
Media are looking for scoops and debates |
This leads to even more confusion among people |
|
The written Press issues different stories on COVID situation |
There is no operational plan for informing all media equally |
Confusion further increases and anti-Covid vaccination actions start. |
|
A lot of figures on infected and dead people are presented each day on TV. Action Plans are not addressed or explained |
|
Number of infected persons + rate of death are not very informative for people. They want useful information, not creation of fear. |
|
Public Health Service has 7 layers of decision-making |
The President decides. All other layers should follow but have no experience |
Decision layers are accusing each-other of failures made. Decision-tree is too fragmented. |
|
There is no updated scenario-book |
Finally, it is admitted that existing scenarios have never been updated |
There was a good scenario for SARS but was not updated in 12 years |
|
Appointing test-facilities |
There are not enough test facilities available |
Outstanding veterinary labs are not allowed to do PCR-testing |
|
Vaccination is not made compulsory |
But it is written in the Constitution |
The reasons why are unclear |
|
ETCETERA ETCETERA |
|
|
The issues addressed in Table 5 unfortunately reflect the amateurism of certain authorities and officials when dealing with an epidemic in their country. This is a very dangerous situation.
Not one European country synchronized with another. Experiences and knowledge were not shared among EU countries. There was no true coordination center for COVID-19 in Europe.
There is ample room for improvement in this area. So far, no signs are visible that the EU or a member state is taking action to avoid this chaos the next time.
There are training centers for educating people in this discipline (e.g. in the USA). The example is the US Center for Risk Communications (www.centerforriskcommunications.org ). They provide international courses for professionals and officials [14].
CONCLUDING REMARKS
The potential role and power of risk identification & risk management in disease control is largely underestimated in dairy veterinary practice. One reason is maybe that it is so easy to apply a vaccine just by injection. One nearly does not need to think, while in risk management one needs to think.
The domains of vaccination and risk management are complementary and therefore should need more attention and implementation. Currently, the (veterinary) literature shows ample publications about risk identification and risk management. One should benefit from these.
The passed COVID-19 situation points to the absolute need of combining the two forenamed domains. This is even more so, when vaccines are not (sufficiently) available and strong emphasis must be put on (emergency) risk management. Public health authorities should be much better prepared for this. There are places where such a type of communication is addressed a specific international training course for professionals and authorities. An example is the US Center for Risk Communications (www.centerforriskcommunications.org).
REFERENCES
- Brand A, Noordhuizen, JPTM, Schukken YH. (2002). Herd Health and Production Management in Dairy Practice. Wageningen Academic Publ., The Netherlands. 543 pp.
- Noordhuizen J, Wentink H. (2001). Epidemiology: Developments in veterinary herd health programmes on dairy farms–a review. Vet Q. 23(4):162-169.
- Noordhuizen J. (2012). Dairy herd health and management. Context Products, UK.
- Covello VT. (2003). The cardinal rules of risk communication. The Heartland Center for Public Health crises. St. Louis, MO, USA.
- Kleen JL, Rehage J. (2008). Communication skills in veterinary medicine. Tierarztliche Praxis. 36:5.
- Kleen JL, Atkinson O, Noordhuizen, JPTM. (2011). Communication in production animal medicine–modelling a complex interaction with the example of dairy herd health medicine. Irish Vet J. 64(1):8.
- Noordhuizen J & Edmondson P. (2019). Arranging a conflict on a dairy farm, a case report: The veterinarian as a process coach. Anim Husb Dairy Vet Sci. 3:1-4.
- Towery D. (2001). Areas of concern in biosecurity. AFIA—BAMN publications, Wilson Boulevard, Arlington, Virginia, USA.
- Noordhuizen J. (2018). Report on a Dairy Farm Audit for improving heat stress management. (Unpublished data).
- Viet AF, Fourichon C, Seegers H. (2007). Review and critical discussion of assumptions and modelling options to study the spread of BVD-virus within a cattle herd. Epidemiol Infect. 135(5):706-721.
- Pun JKH. (2020). An integrated review of the role of communication in veterinary clinical practice. BMC Vet Res. 16(1):394.
- Noordhuizen J. (2022). Emergency crisis management: the example of dairy cattle farming. AAPS. 1(5):555574.
- Noordhuizen JPTM, van Dijke J. (2020). Risk communication in the case of major disasters: the COVID-19 example. Research Gate.
- www.centerforriskcommunications.org Consulted on February 6, 2020.
ANNEX 1. Seven Cardinal Guidelines for Emergency Risk Communication
(Adapted from Covello 2003 by the author)
BEST PRACTICE 1: Accept and involve stakeholders
- Show respect for people affected by risk management decisions by involving them early: that is, before crucial decisions are made.
- Involve all parties which have an interest or stake in a particular hazard or risk.
- Include in the decision-making process the broad range of factors involved in determining public perception of risk concern and outrage.
- Use a wide range of communication channels to engage and involve stakeholders.
- Adhere to the highest ethical standards and recognize that people hold you professionally and ethically responsible.
- Strive for mutually beneficial outcomes.
BEST PRACTICE 2: Listen to the people
- Before acting, find out what people know, think, or want done about risks. Use techniques such as interviews, facilitated discussion groups, information exchanges, availability sessions, advisory groups, toll-free numbers, surveys.
- Let all parties with an interest or a stake in the issue of concern be heard.
- Let people know that what they said has been understood and tell them what actions will follow.
- Acknowledge the validity of people’s emotions.
- Emphasize communication channels that encourage listening, feed-back, participation and dialogue.
- Recognize that competing agendas, symbolic meanings and broader social, cultural, economic, or political considerations may complicate risk communication.
BEST PRACTICE 3: Be truthful, honest, frank, and open
- Disclose risk information as soon as possible. Fill information vacuums.
- If information is evolving or incomplete, emphasize appropriate reservations about its reliability.
- If in doubt, lean toward sharing more information, not less. Or else people may think that something significant is being hidden or withheld.
- If you don’t know or are unsure about an answer, express willingness to get back to the questioner with a response by an agreed-upon deadline. Do not speculate.
- Discuss data and information uncertainties, strengths, weaknesses (including those identified by other credible sources)
- Identify worst-case estimates as such and cite ranges of risk estimates when appropriate.
- Do not minimize or exaggerate the level of risk; do not over-reassure neither.
- If errors are made, correct them rapidly.
BEST PRACTICE 4: Coordinate, collaborate and partner with other credible sources
- Coordinate all inter- and intra-institutional communications.
- Devote efforts and resources to the slow, hard work of building partnerships and alliances with other organizations.
- Use credible and authoritative intermediaries between you and your target audience(s).
- Consult with others to decide who is best able to take the lead in responding to questions or concerns about risks. Document and date these decisions.
- Cite credible sources that believe what you believe. Issue communication with or through other trustworthy sources.
- Do not attack individuals or organizations with a higher perceived credibility.
BEST PRACTICE 5: Meet the needs of the medias
- Be accessible to reporters; respect their deadlines.
- Prepare a limited number of key messages before media-interactions. Take control of the interview and repeat your key messages several times.
- Keep interviews short. Agree with the reporter in advance about the specific topics to address and stick to that topic during the whole interview.
- Say only what you want the media to repeat. Everything you say is on the record.
- Tell the truth, do not speculate.
- Provide background materials about complex risk issues.
- Provide information which is tailored to the needs of each type of media.
- If you don’t know the answer to a question, focus on what you do know and tell the reporter what action you will take to get an answer.
- Be aware of and respond effectively to media pitfalls and trap-questions.
- Avoid saying ‘’no comment’’.
- Follow up on stories with praise or criticism, as warranted.
- Work to establish long-term relationships with editors and reporters.
BEST PRACTICE 6: Communicate clearly and with compassion
- Use clear, non-technical language, adapted to the target audience.
- Use graphics and other pictorial material to clarify your messages.
- Personalize risk data. Use stories, narratives, examples, and anecdotes to make technical data come alive.
- Avoid embarrassing people.
- Respect the unique communication needs of special and diverse audiences.
- Express genuine empathy. Acknowledge and say that any illness, injury, or death is a tragedy to be avoided.
- Avoid using distant, abstract, unfeeling language when discussing harm, deaths, injuries, and illness.
- Acknowledge and respond in words, gestures, and actions, to emotions that people express (anxiety, fear, anger, outrage, uncertainty, helplessness)
- Acknowledge and respond to the distinction that the public considers as important in evaluating risks.
- Use risk comparisons to help put risks in a perspective; make sure those comparisons consider the distinctions the public considers important.
- Identify specific actions that people can take to protect themselves and maintain control of the actual situation.
- Always try to include discussion of actions that are underway or can be taken.
- Be sensitive to local norms such as speech and dress.
- Only promise what you can deliver, then follow through.
- Understand that truth is earned. Do not ask or expect to be trusted by the public.
BEST PRACTICE 7: Plan thoroughly and carefully
- Start with clear, explicit objectives (providing information, or establishing trust, or encouraging appropriate actions, or stimulating emergency responses, or involving stakeholders in dialogue, or partnership, or joint problem solving).
- Identify important stakeholders and subgroups within the audience; respect diversity and design communication for specific stakeholders.
- Recruit spokespersons with effective presentation and personal interaction skills.
- Train staff, including technical staff, in basic, intermediate, and advanced crisis communication skills. Recognize and reward outstanding performances.
- Anticipate questions and subjects of concern.
- Prepare and pre-test messages.
- Carefully evaluate risk communication efforts and learn from mistakes.
- Share what you have learned with others.
Center for Risk Communications, New York, NY USA
EBSCO Publishing, 2003
Journal of Health Communication 8: 1-5
(Covello, 2003)