Information Links
Related Conferences
Previous Issues Volume 4, Issue 1 - 2022
Utilizing Music Therapy during an Exercise Program to Reduce Blood Pressure and Depressive Symptoms in Adult Patients with Cardiovascular Diseases
Joan Katherine Maldonado-Resto
Marybelle and S. Paul Musco School of Nursing and Health Professions, Brandman University, Irvine, California
Corresponding author: Joan Katherine Maldonado-Resto, Marybelle and S. Paul Musco School of Nursing and Health Professions, Brandman University, Irvine, California. Tel: 949-341-9800; Email: [email protected]
ABSTRACT
Cardiovascular disease (CVD) is the leading source of morbidity and mortality in the United States (U.S.) and worldwide (American Heart Association [AHA], 2017). Emphasis should be placed on modifying risk factors that can potentiate the development and/or progression of CVD. Healthcare providers should consider addressing the physiological and psychological components of these individuals. Music interventions have been utilized in the past to reduce blood pressure and depression symptoms. This quasi-experimental project evaluated the effect of music therapy during an exercise program on blood pressure and depression scores utilizing the Patient Health Question-9 (PHQ-9) scale in adult hypertensive patients with CVD and moderate- severe depression. The sample consisted of 11 adult male and female patients between the ages of 18-65 in a private cardiology practice in rural Maryland. A paired sample t test was utilized to assess the significance of a decrease in average systolic and diastolic blood pressures and PHQ-9 depression scores before and four-weeks after the intervention. The t test revealed that the average systolic blood pressure decreased pre versus post-intervention from 120.4 (SD=12.4) to 116.4 (SD=9.5). Average diastolic blood pressure decreased by a smaller amount from 75.6 (SD=7.2) to 74.0 (SD=7.0). Depression decreased significantly following the intervention from an average PHQ-9 score at baseline of 13.8 (SD=3.3) to 5.7 (SD). Reducing blood pressure and depression scores utilizing music therapy during an exercise program in patients with CVD can potentially reduce myocardial infarctions (MIs) and cardiovascular events.
Keywords: music therapy, hypertension, depression, cardiovascular disease
CHAPTER 1
Cardiovascular disease (CVD) imposes an extensive amount of health issues, financial burdens and deaths in the United States (U.S.) and globally (Benjamin et al., 2019; Centers for Disease Control and Prevention [CDC], 2017; World Health Organization [WHO], 2017).
According to the CDC, CVD is the primary source of mortality in both men and women resulting in approximately 610,000 deaths yearly in the U.S. (CDC, 2017). Of these results, coronary heart disease (CHD) is the leading type of CVD causing 370,000 deaths annually (CDC, 2017).
Roughly, 735,000 Americans experience a heart attack yearly, of these results, 510,000 individuals have their first heart attack and 210,000 occur in individuals who have already had a heart attack (CDC, 2017). Globally, CVD is the number one cause of death producing 31% of deaths worldwide and 85% of these deaths are attributed to heart attacks and stroke (WHO, 2017). The complex sequela of CVD impacts individuals’ physical, psychological, and social well-being (Antonakoudis et al., 2006). Primary risk factors for CVD include hypertension, hyperlipidemia, diabetes, smoking, sedentary lifestyle, obesity, as well as, males, elderly, stress, and family history (De Hert et al., 2018). However, of all of these risk factors, hypertension (HTN) is considered a leading cause of worsening cardiovascular health resulting in roughly 47% of coronary artery disease and 54% of strokes worldwide (Wu et al., 2015). HTN has also been correlated with harmful effects to specific organs such as retinopathy, left ventricular hypertrophy (LVH), chronic kidney disease and vascular dementia which are identified as “target organ damage” (TOD) (Nadar, Tayebjee, Messerli, & Lip, 2006). Hypertension is defined as a systolic blood pressure of ≥130 mmHg or diastolic blood pressure ≥80 mmHg, or patient self- report use of anti-hypertensive medications, or advised by a physician/healthcare professional that one has high blood pressure at least twice (Benjamin et al., 2019). In considering this definition, the age modification prevalence of adults ≥ 20 years in age in the U.S. who have HTN was equal to approximately 116.4 million (Benjamin et al., 2019). Of these results, 35.3% of U.S. adults were not aware they had HTN (Benjamin et al., 2019).
Depression may also contribute to the global burden of CVD (De Hert et al., 2018). The association between CVD and depression appears to be bi-directional (Mensah & Collins, 2015). For instance, individuals with CVD have an increased risk for depression, and individuals with depression have a higher risk for various non-communicable diseases (NCDs) such as CVD (Mensah & Collins, 2015). Depression independently provides a detrimental prognosis for CVD morbidity and mortality (Mensah & Collins, 2015). In addition, depression can impair individuals with CVD quality of life which may affect the success of efficient “prevention, detection, evaluation, and treatment of CVD as well as rehabilitation after cardiovascular events” (Mensah & Collins, 2015, p. 221). The impact is that individuals with depressive disorders average life span are 8-20 years lower than individuals without these disorders with deaths frequently occurring from NCDs such as CVD (Mensah & Collins, 2015). Thus, addressing the risk determinants that contribute to the development of CVD and its progression is imperative in reducing further cardiovascular events.
Music therapy is an applicable collective approach in the physical and psychological field for decreasing risk factors that potentiate CVD and cardiac events (Metzger, 2004). Music therapy is defined by the American Music Therapy Association (2021) as “the clinical and evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship by a credentialed professional who has completed an approved music therapy program” (p, 2). Research on music therapy has been conducted in the past which has shown to alter cardiovascular measurements like blood pressure and heart rate, enhance mood and inclination to exercise (Bowles et al., 2019; Metzger, 2004). However, inconsistent findings in this research require further investigation to distinguish implications for use in clinical practice. This project aims to evaluate the effect of music therapy during an exercise program on blood pressure and depression scores utilizing the PHQ-9 scale in adult hypertensive patients with CVD and moderate-severe depression.
1.1 Background and Significance
The 2020 Impact Goals of the American Heart Association (AHA) aims to reduce mortality associated with cardiovascular disease (CVD) and stroke by 20% through the needed attention of the treatment of acute CVD events and secondary prevention (Benjamin et al., 2019). Secondary prevention after a CVD event is focused on both pharmacological interventions and modifying risk factors to prevent future occurrences (Benjamin et al., 2019). Several risk factors influence the advancement of CVD (Nystoriak & Bhatnagar, 2018). Hypertension is the most important risk factor for CVD and stroke (Benjamin et al., 2019; Wu et al., 2015). In a conducted study of over one million hypertensive adults, the life span risk of CVD at the age of 30 was 63.3% in comparison to 46.1% without HTN (Benjamin et al., 2019). Also, those adults with HTN advanced to CVD five years earlier than those without HTN (Benjamin et al., 2019). Between 2006 and 2016, the mortality rate attributed to HTN increased by 18% and the exact number of mortalities resulting from HTN rose 46.3% (Benjamin et al., 2019). The eradication of HTN could decrease CVD deaths by 38.0% among females and 30.4% among males (Benjamin et al., 2019).
Psychological factors, such as depression, can also affect the outcomes of individuals with CVD or post cardiovascular events (Meijer et al., 2013; Smolderen, 2017). Depression is associated with an increased risk of developing CVD and worsening outcomes in individuals with established CVD (Leung et al., 2015). Studies propose that individuals with worsening CVD are at a higher risk of developing depression symptoms (Meijer et al., 2013). This may be due to the psychological response to the disease and the sequela of the disease, and also, physiological components that affect CVD which may produce depressive symptoms (Meijer et al., 2013). Several meta-analysis studies have revealed that depression was linked to an increase in mortality rates after an acute myocardial infarction (AMI) (Thombs et al., 2005). In a study conducted by Thombs et al. (2005), major depression was determined in approximately 19.8% of AMI survivors utilizing systematic interviews. The same study also identified substantial depressive and anxiety symptoms in the studied participants (Thombs et al., 2005). Another study conducted by Stewart, Perkins, & Callahan (2014) discovered if synergistic care for patients that suffer from depression is delivered before clinical manifestations of CVD, it decreases the risk of hard CVD events. The specific fundamental mechanisms that correlate these associations are still under further investigation but more likely are multifactorial with physiological, social, and behavioral mechanisms (Smolderen, 2017). Physiological mechanisms of CVD that result in symptoms of depression and worsening prognostic outcomes include elevations in inflammatory cytokines, alterations to the hypothalamic-pituitary-adrenal (HPA) system leading to chronically elevated glucocorticoid secretion as well as cortisol levels that may suppress the immune system (McCance & Huether, 2015; Meijer et al., 2013). Also, depression may affect individuals’ motivation to adhere to medication and exercise regimes (Smolderen, 2017). It can increase poor social habits such as tobacco, alcohol and/or drug abuse (CDC, 2012).
Music therapy has been extensively utilized in clinical practice as a nonpharmacological complementary to medical therapy (Liu & Petrini, 2015). In a meta-analysis by Soares do Amaral et al. (2016), the use of music therapy in hypertensive patients resulted in a significant reduction of systolic blood pressure. A randomized-control trial using passive listening to raga Indian music and lifestyle modifications in participants with prehypertension and/or stage 1 hypertension demonstrated a considerable decrease in both systolic and diastolic blood pressures and stress levels (Kunikullaya et al., 2015). A systematic review of the Bonny Method of Guided Imagery and Music sessions by McKinney & Honig (2017), revealed that utilization of these sessions resulted in positive effects on physical variables such as blood pressure, chronic pain, and cortisol and beta-endorphin plasma levels. This study also presented evidence to advantageous outcomes for various mood variables including depression, anxiety, and total mood disturbance. (McKinney & Honig, 2017). In a multiple-case study design by Aalbers et al. (2020), reduction in depressive symptoms was demonstrated after utilizing emotion-regulating improvisational music therapy (EIMT) in young adult students after ten-week sessions and was sustained on a four-week follow-up. A randomized-controlled trial conducted by Biasutti & Mangiacotti (2021) used music training in elderly participants and proved an improvement in depression scores measured by the Geriatric Depression Scale. To enhance prognostic outcomes in individuals with CVD concentration should be focused on promoting efforts to reduce high blood pressure as well as managing psychological burdens.
1.2 Problem Statement
Cardiovascular disease (CVD) is an outstanding epidemic and the leading cause of mortalities and morbidities globally (CDC, 2012; Sumner, Harrison, & Doherty, 2017). Acute myocardial infarction (AMI) is the most frequent cause of death from CVD occurring every 40 seconds in the U.S. alone (CDC, 2017). The burden of CVD financially equates to roughly $200 billion yearly. The American Heart Association aims to decrease mortality rates derived from CVD and stroke by treating acute events and through secondary prevention measures (Benjamin et al., 2019).
Hypertension (HTN) is a serious public health issue with a great prevalence in the general population serving as an essential risk for CVD (Soares do Amaral, 2016). Some of the consequences of HTN include myocardial infarction, angina, and stroke (Benjamin et al., 2019). By 60 years of age, the lifetime risk for CVD in individuals with HTN was 60.2% in comparison to 44.6% for their counterparts who do not have HTN (Benjamin et al., 2019). Mortality rates are also resulting in 82,735 deaths in 2016 primarily attributed to HTN (Benjamin et al., 2019).
Similar to other chronic diseases, CVD affects individuals’ physiological health as well as psychological and social behaviors (Antonakoudis et al., 2006). As these individuals advance in age and their health status worsens, they may become more depressed (Antonakoudis et al., 2006). Also, individuals with CVD frequently experience hardship related to diagnosis, surgery and/or diagnostic procedures, hospitalization, the ambiguity of outcomes, fear of death, uncertainties about healing and recovery, loss of hope and autonomy (Bradt, Dileo, & Potvin, 2013). These factors place cardiac individuals at a higher risk for adverse effects and sudden cardiac death (Bradt, Dileo, & Potvin, 2013).
Music interventions have been utilized in the past to decrease anxiety and stress and enhance both psychological and physiological effects in individuals with CVD (Bradt, Dileo, & Potvin, 2013). In a study completed by Chang (2011), music had a favorable effect on physiological responses and reduction in anxiety in individuals undergoing cardiac catheterization. In another study, music therapy sustained elevated mood, increased desire to exercise and facilitated continued rehabilitation efforts in individuals undergoing cardiac rehabilitation (Bowles et al., 2019). Studies have also shown music therapy may have blood pressure lowering effects. In a meta-analysis study conducted by Loomba et al. (2012), it was discovered that music therapy led to a significant reduction of systolic and diastolic BP. In an experimental study by Gogate & Patil (2019), the use of musical therapy in conjunction with physiotherapy in women with pregnancy-induced HTN resulted in a significant drop in systolic and diastolic blood pressures. Research in the use of music therapy to optimize physical and psychological variables has been conducted but with inconsistencies that warrant further examination of the evidence to establish this as an intervention in clinical practice.
1.3 Historical and Societal Perspectives
Hypertension (HTN) was not always viewed as a chronic disease as it is known now (Saklayen & Deshpande, 2016). For instance, during the presidential term of President Franklin D. Roosevelt, a blood pressure of 220/120 mmHg was still deemed the president in healthy condition by his physician (Saklayen & Deshpande, 2016). He later suffered a hemorrhagic stroke and as a result, raised awareness that HTN may cause mortality (Saklayen & Deshpande, 2016). Several years after Roosevelt’s death, President Truman signed the National Heart Act which paved the way for studies of heart diseases which included the Framingham Heart Study (Saklayen & Deshpande, 2016). The Framingham studies were consistent in demonstrating that HTN was associated with CVD morbidity and mortality including myocardial infarctions, heart failure, and strokes (Saklayen & Deshpande, 2016). Since then, aggressive research has been conducted with recognition of HTN as essential and the development of effective pharmacological therapy for control (Saklayen & Deshpande, 2016). However, even with awareness of HTN reaching a favorable goal of 83%, the rate of control is still only 50% (Saklayen & Deshpande, 2016).
Depression is progressively developing into a dominant factor in mortality and morbidity, especially when combined with chronic disease (Davidson, 2012). It is highly coexistent with CVD equating to two to three times more prevalent amongst individuals with CVD than in the general population (Vaccarino et al., 2019). Societal perspectives, including numerous researchers and the general public, presume depression is an absolute disorder, and those individuals who have depressive symptoms have a disorder subjectively different from daily stress (Davidson, 2012). As a result, depressive symptoms are perceived as a psychological disease as defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (Davidson, 2012). However, there are additional developing factors for these symptoms (Davidson, 2012). Depressive symptoms may affect compliance with medications, follow-up visits, and necessary lifestyle modifications (Vaccarino et al., 2019). It may also cause a decrease in physical activity during the recovery process after a cardiac event (Gathright et al., 2018).
Despite these considerations, depression is commonly unidentified and left untreated in individuals with CVD (Vaccarino et al., 2019). Some barriers to the detection of depression include a lack of training and deficiency in knowledge of mental health in cardiology practices, as well as a lack of approach to the problem (Vaccarino et al., 2019). In addition, depressive symptoms may be mistaken with physiological diseases (Vaccarino et al., 2019). Research shows that psychological aspects should be addressed to facilitate recovery and prevent disease progression in individuals with CVD.
1.4 Incidence and Prevalence
Approximately 45% or 108 million adults in the United States (U.S.) have hypertension (HTN) and of these adults, only 24% have controlled HTN (CDC, 2020). Almost half of the adults in the U.S. with uncontrolled HTN have a blood pressure ≥ 140/90 mmHg (CDC, 2020). In 2018, HTN was a primary or contributing factor of mortalities for greater than 494,873 individuals in the U.S. (CDC, 2020). In 2015, 42,749,000 of 990,808,000 primary care office visits had a principal diagnosis of HTN and a sum of 1,182,000 of 136,943,000 emergency room visits were for essential HTN (Benjamin et al., 2018). In considering local areas of the U.S., Anne Arundel County, Maryland accounts for over 544,400 residents (Anne Arundel County [AAC], 2014). Of these results, HTN was responsible for 166.09 per 100,000 population of emergency room visits between 2009 and 2011 (Anne Arundel County Department of Health [AACDH], 2020). The top leading cause of death in Anne Arundel County for 2018 was cancer followed closely by CVD (AACDH, 2020). Among risk factors for the development of HTN, depression, stress and anger were associated with an increase in blood pressure progression in the Jackson Heart Study (Benjamin et al., 2019). A systolic blood pressure <120 mmHg resulted in fewer CVD events and mortality in the SPRINT trial (Benjamin et al., 2019).
Individuals with chronic diseases are susceptible to also developing depression (CDC, 2012). Other factors that may contribute to the development of psychological health disorders include family history, increase life stressors, traumatic experiences, drug abuse and lack of social support and/or childhood neglect or abuse (CDC, 2012). In the U.S., 4.7% of adults ≥ 18 years of age experience typical symptoms of depression and account for 48,344 suicide deaths (CDC, 2020a). Locally, there has been an increase of 70% in residents seeking mental health services and 26.3% of emergency room visits account for mood disorders such as depression (AAC, 2019). Depression is estimated to coexist in 17% of individuals who have CVD (CDC, 2012). In individuals who have suffered an MI, the prevalence of major depression or elevation in depression symptoms is relatively increased at roughly 20% in comparison to 5% contrarily in healthy individuals of comparable age (Meijer et al., 2013). Post-MI depression has been identified with poorer outcomes, and research into the validity of this identification has been established in several meta-analyses, which revealed that individuals with post-MI depression were 1.59-2.71 times higher to early death or had an additional cardiovascular event than individuals without depression (Meijer et al., 2013). Statistics as the ones mentioned above testify to the severity of HTN and depression on worsening prognostic outcomes and mortality in individuals with CVD.
1.5 Healthcare Cost
The impact of cardiovascular disease (CVD) on healthcare-related costs in the United States (U.S.) is substantial. Currently, CVD is the U.S.’s most costly chronic disease and it is projected to increase in the upcoming decades (AHA, 2017). Direct medical costs include health- related services provided by healthcare providers in the outpatient or inpatient setting, costs for follow-up care, home health care, or skilled nursing facilities and medications (AHA, 2017).
These costs will continue to rise for all racial backgrounds; however, there is racial and gender disparities with expected costs to triple over the next two decades for Hispanics, double amongst African Americans and greater costs will be allocated for female than males (AHA, 2017). There are also indirect medical costs related to lost time from work, unforeseen death related to CVD that may also have a spiraling effect on expenses (AHA, 2017).
Healthcare costs specific to hypertension (HTN) averaged $55.9 billion annually in direct and indirect costs (Benjamin et al., 2019). These healthcare costs are projected to rise by approximately $220.9 billion in total direct costs by 2035 (Benjamin et al., 2019). In 2014, prescription costs for anti-hypertensive medications equated to $28.81 billion (Benjamin et al., 2019). For adults ≥ 18 years of age with no co-morbidities diagnosed with HTN, the average yearly costs of HTN ranged from $3914 to $13920 for those with multiple co-morbidities (Benjamin et al., 2019).
Depression healthcare-related costs are also surging with $187.8 billion in expenditure in 2013 with an annual rate of 3.7% increase between 1996 and 2013 (Winerman, 2017).
Depressive disorders are the most expensive of mental and substance abuse disorders with a mean yearly cost of $71 billion. With such devastating health and economical burdens, healthcare providers must be proactive in delivering the most evidence-based care in their clinical practice.
1.6 Foundation of PICOt
Cardiovascular disease (CVD) imposes an overwhelming number of deaths in the United States (U.S.) and globally with projections of prevalence to increase in the upcoming decades (AHA, 2017). The effects of CVD on the health of individuals and economically are devastating (AHA, 2017). As such, healthcare providers and leaders must tackle the issues that increase risks of CVD development through primary prevention as well as reducing future events through aggressive secondary prevention. HTN is known as a primary causative factor in the development of CVD (Benjamin et al., 2019). Studies also show that it is equally important to direct attention to the psychological aspects of CVD (Bradt, Dileo, & Potvin, 2013). For health care providers to maximize care and reduce overall risk factors in the development of CVD events, they must administer a holistic approach to individuals with CVD. Various factors must be addressed to improve outcomes in individuals with CVD which include optimizing blood pressure control, adherence to physical activity, heart-healthy diet, smoking/alcohol cessation, weight reduction in the obese, as well as psychological factors such as depression and anxiety (CDC, 2012). Utilizing music therapy during an exercise program may have a beneficial effect on both physical and psychological outcomes for individuals with CVD. However, these interventions still require further investigation to employ for use in clinical practice. In allocating extensive research and resources to focus on music therapy during an exercise program, it is with great hope to identify this intervention as a standard of treatment to enhance the outcomes of individuals with CVD.
CHAPTER 2
2.1 Introduction of the PICOt Question
Experiences in the health care practice may influence health care providers to advocate for changes in health care policies, laws or regulations that have a direct impact on patient outcomes and the health care system. Oftentimes, a problem is identified within a clinical practice that may cause providers to investigate potential solutions. As such, health care providers must pursue the next step by identifying a research question to guide a systematic review of the literature to explore evidence-based interventions with inspiring results to utilize in their clinical practice. The PICOt format is a useful tool to outline research questions that examines the outcome of therapy and is as follows: P-Population, I-Intervention, C-Comparison of the intervention with alterations of the same intervention or other treatments, O-Outcomes that represent the effectiveness of the intervention, t-time indicating the duration of collecting data (Grove et al., 2015; Riva et al., 2012).
The problem identified in a private cardiology practice in rural Maryland was the lack of screening and treatment of depression in hypertensive patients with cardiovascular disease (CVD). This issue may result in worsening health outcomes in these individuals. Music therapy has been utilized in the past to lower blood pressure and depressive symptoms. Extensive research has been conducted on the advantageous effects of music therapy but requires further investigation to implicate it in clinical practice. This project will add to the body of knowledge on how music therapy contributes to favorable effects on blood pressure and depressive variables.
In adult male and female hypertensive patients 18-65 years with cardiovascular disease and concurrent moderate-severe depression, will utilization of music therapy during an exercise program compared to those who do not, improve blood pressure and depression symptoms in a four-week time frame?
A systematic review of current literature on the benefits of music therapy on blood pressure and depression was conducted using various databases including CINAHL, Medline, and PubMed. Key terms were identified and consisted of “music therapy or music intervention or musical therapy,” “hypertension or high blood pressure or elevated blood pressure or htn or hypertensive” and “depression or depressive disorder or depressive symptoms or major depressive disorder.” The CINAHL search yielded 213 articles while the Medline search yielded 318 articles. The MeSH system utilized in the PubMed database yielded 136 articles. The specific themes of this search were “effects of music therapy and/or music intervention on changes in blood pressure” and “music training/therapy/intervention improving depressive symptoms.” The search became refined when limitations were set including articles written only in English, academic journals and/or clinical core journals and published from 2015 to 2021. The literature search provided a comprehensive scope of the problem and outcomes of therapy. Eight articles were selected to support music therapy as a means of reducing blood pressure and depression to invoke change to current practice.
2.2 Synthesis of the Literature
The topics researched for the synthesis of this literature involved the use of music therapy and/or music intervention to reduce blood pressure and depressive symptoms. The criteria incorporated for the review of studies were: (1) pilot studies, randomized-controlled trials or meta-analysis design, (2) composed of patients with hypertension and/or depression, (3) included music therapy and/or music intervention to approach these underlying issues. Studies that were excluded from the review included editorials or periodicals. The literature search to support this clinical scholarly project yielded several themes.
Music Therapy Reduces Blood Pressure in Hypertensive Patients
Music therapy has demonstrated advantageous effects on lowering blood pressure in hypertensive individuals. In a randomized controlled trial conducted by Gogate & Patil (2019), 40 women in their third trimester of pregnancy with pregnancy-induced hypertension (HTN) were randomly selected to a music therapy group versus a music therapy group with physiotherapy. The music therapy group listened to OMKAR mantra in a low voice for 30 minutes daily until delivery (Gogate & Patil, 2019). In the alternative group, musical therapy was used in conjunction with physiotherapy (Gogate & Patil, 2019). Each group demonstrated a significant reduction in systolic and diastolic blood pressures. The group with music therapy and physiotherapy experienced a greater reduction in systolic and diastolic blood pressures than just music alone with p = <0.0001 (Gogate & Patil, 2019).
In a randomized controlled trial by Kunikullaya et al. (2015), a hundred individuals with prehypertension and stage one HTN were randomly divided into a music intervention with lifestyle modifications while the other group received lifestyle modifications alone. The music intervention group listened to raga bhimpalas played by a flute five days a week at 15-minute intervals for three months (Kunikullaya et al., 2015). A reduction in diastolic blood pressure was significantly lower in the music intervention group (p = 0.004) than lifestyle modifications alone (p = 0.015) (Kunikullaya et al., 2015).
Another study conducted by Liu & Petrini (2015) examined the effects of listening to music on pain, anxiety, and vital signs in patients post thoracic surgery. The design of the study was a randomized controlled trial with a convenience sample of 112 patients (Liu & Petrini, 2015). The experimental group received standard care in combination with a 30-minute music intervention for three days (Liu & Petrini, 2015). The control group received standard care alone (Liu & Petrini, 2015). The study revealed a significant difference in the experimental group after intervention concerning pain, anxiety and systolic blood pressure (Wald χ2 = 5.498, p = 0.019) compared to the control group (Liu & Petrini, 2015).
A meta-analysis performed by Soares do Amaral et al. (2016) investigated the effects of music in patients with HTN. Various databases were utilized in this meta-analysis including Scopus, Pubmed, LILACS, MEDLINE, IBECS and SciELO through a Virtual Health Library (Bireme) (Soares do Amaral et al., 2016). Randomized controlled trials evaluating the effects of music on systolic and diastolic blood pressure in patients with HTN were reviewed (Soares do Amaral et al., 2016). Three studies were selected which met the criteria and demonstrated an improvement in systolic blood pressure in the music group with weighted mean differences (− 6.58 95% CI: − 9.38 to – 3.79) in comparison to the control group (Soares do Amaral et al., 2016).
Music Therapy Improves Depressive Symptoms
In the realm of psychological disorders, music therapy has shown breakthroughs in enhancing mood in individuals with depressive disorders. In a multiple-case study design by Aalbers et al. (2020), Emotion-Regulating Improvisation Music Therapy (EIMT) was utilized in 11 young adult students with depressive symptoms for 10 weekly 60-minute sessions (Aalbers et al., 2020). Depressive symptoms were assessed using the Inventory of Depressive Symptomatology Self-Report assessment at baseline, at 10 weeks and four weeks following the intervention (Aalbers et al., 2020). The study revealed a significant reduction of depressive symptoms after EIMT in all 11 students (χ2 (2) = 15.42, p < .01) (Aalbers et al., 2020). These results also remained at a four-week follow-up (Aalbers et al., 2020).
Another study conducted by Biasutti & Mangiacotti (2021) utilized a music training program in 45 healthy elderly individuals with cognitive impairment between the ages of 62-95. The participants were randomly assigned to an experimental or control group (Biasutti & Mangiacotti, 2021). The experimental group attended an intense music-training program composed of 70-minute sessions twice a week for a total of 12 weeks (Biasutti & Mangiacotti, 2021). Depression severity was measured by the Geriatric Depression Scale pre-and post- intervention (Biasutti & Mangiacotti, 2021). The study revealed a significant improvement in depression scores in the experimental group (t =1.450; p < .005; d = 0.453) while the control group did not show improvement (t = 0.080; p > .1; d = 0.025) (Biasutti & Mangiacotti, 2021).
A pilot study conducted by Bowles et al. (2019) utilized a music intervention in 17 patients undergoing cardiac rehabilitation to assess mood, motivation and exercise. A Brief Mood Introspection Scale (BMIS) and a 5-point visual analog scale (VAS) were measured at baseline and at eight weeks (Bowles et al., 2019). The results of the study showed that music appeared to improve mood and motivated patients to exercise (Bowles et al., 2019). A descriptive analysis of the BMIS subscale revealed an elevation on the happiness scale scores and low scores were given for unhappiness (Bowles et al., 2019).
A systematic review by McKinney & Honig (2017) studied the health outcomes of the Bonny Method of Guided Imagery and Music (GIM). The review included repeated measures designs, randomized and non-randomized controlled trials that noted physiological and psychological outcomes after a minimum of six Bonny Method of GIM sessions (McKinney & Honig, 2017). Nine studies met the criteria and eight studies had a medium to low risk of bias (McKinney & Honig, 2017). Collectively, these studies included 275 participants between the ages of 18-78 years (McKinney & Honig, 2017). Some of the variables measured were depression, anxiety, systolic and diastolic blood pressures (McKinney & Honig, 2017). The results yielded favorable outcomes for improvement in depressive symptoms as well as systolic and diastolic blood pressures after a series of Bonny Method of GIM (McKinney & Honig, 2017).
There is a wealth of literature that demonstrates music therapy as a useful tool to lower blood pressure and depressive symptoms. However, inconsistencies in how music therapy is utilized and delivered in these studies present a gap in research for implementation in clinical practice. Commonly, each study referenced throughout this paper-demonstrated music as a non- invasive, cost-effective, non-pharmacological tool that may be used to improve blood pressure in hypertensive individuals and enhance depressive mood. It would be feasible to implement this intervention in a multitude of settings including inpatient as well as outpatient clinical practices. Overall, music therapy is a relatively safe intervention that may be administered and has rewarding effects on cardiovascular and mental health.
2.3 Theoretical Framework
The theoretical foundation and conceptual framework underlying the proposed clinical scholarly project (CSP) is the Neuman’s Systems Model. The Neuman’s System Model centralizes on an individual’s reactions to internal and external stimuli and the application of primary, secondary and tertiary prevention as a clinical intervention for conservation and adaptation for the overall wellness of an individual (Nursing Theory, 2016). Primary prevention is reducing risk factors that can potentiate a disease (Nursing Theory, 2016). Secondary prevention pertains to symptom relief and implementing effective interventions that can decrease the advancement of a disease (Nursing Theory, 2016). Whereas tertiary prevention correlates with altering mechanisms that are in process to facilitate the reconstitution of the individual (Nursing Theory, 2016). The Neuman’s System Model focuses on variables that offer individuals protection facing any type of threat include physical, psychological, sociocultural, spiritual, and developmental variables (Basogul & Buldukoglu, 2020). These variables are constantly interacting with each other (Basogul & Buldukoglu, 2020). In this regard, we can say that the Neuman’s Systems Model focuses on the holistic care of individuals. The physical variable relates to the body’s physiological structure and function (Basogul & Buldukoglu, 2020; Nursing Theory, 2016). The physical variable of this CSP was represented by the patient’s physical responses to music therapy, which involved measurements of the patient’s blood pressure. The psychological variable involves mental processes in connection to one’s environment (Basogul & Buldukoglu, 2020). The psychological variable for this CSP was represented by music therapy in interaction with the patient’s depressive health states. The sociocultural variable denotes the impact of an individual’s social and cultural surroundings (Basogul & Buldukoglu, 2020). The sociocultural variable of this CSP was represented by the social support patients received from each other during each session. The spiritual variable is attributed to an individual’s spiritual beliefs and influences and was represented in this project by utilizing calming music as background and motivational words during cool down after patients engaged in the exercise portion of the program (Basogul & Buldukoglu, 2020). The developmental variable concerns the individual’s “age-related processes and activities” (Basogul & Buldukoglu, 2020, p. 149). The developmental variables for this CSP were represented by personal data collected from each patient regarding their sex, age, race, education, and employment status. The conceptual framework of this CSP was designed to correspond to Neuman’s System Model by heightening some variables that protect individuals against any threats to offer protection to the central core. The central core is represented by blood pressure and depression. If music therapy during an exercise program is effective, then the central core is augmented with a reduction in blood pressure and depressive symptoms. Thus, this CSP mainly offers secondary prevention but also falls within the scope of primary prevention by promoting healthier lifestyle habits.
CHAPTER 3
3.1 Study Design
The purpose of this clinical scholarly project (CSP) is to build on earlier studies of music therapy and identify its potential use to decrease blood pressure and depressive symptoms and enhance the outcomes of individuals with cardiovascular disease (CVD). The design of the project is a quasi-experimental quantitative design. This project evaluated the effects of music therapy during an exercise program on blood pressure and depression scores utilizing the Patient Health Question-9 (PHQ-9) scale in hypertensive patients with CVD and moderate-severe depression. Participants were recruited from a private cardiology practice in rural Maryland.
Patients were administered a PHQ-9 assessment upon initial intake by the investigator (Appendix A). The investigator evaluated the patient’s PHQ-9 score and completed a thorough health assessment and physical to determine if the patient met the criteria to participate in the project. If the patient met the criteria, the project was explained to the patient and a packet was provided.
The packet contained essential forms for the project including the Brandman Bill of Rights, a consent form, demographic assessment, and a voluntary informal survey regarding their genre preference in music (Appendices B, C, D, E). The packet was collected including consent by the investigator prior to the patient leaving and the patient then scheduled his/her time to participate. The project was conducted every Friday consecutively for four weeks. Once the project commenced, the participants arrived at the private cardiology facility in hourly increments according to their scheduled time. Blood pressure monitoring was performed prior to the session according to the recommendations by the American Heart Association. COVID-19 precautions including social distancing, facial mask requirement, hand sanitization, and equipment sanitization were enforced per Centers for Disease Control Prevention (CDC) guidelines. Music therapy sessions began with a warm-up and stretching led by the investigator and were followed by the participants selecting their choice of exercise equipment. Studies have revealed that offering participants a choice of music reduced anxiety, improved relaxation, and led to efficacious results (Chan et al., 2009). Therefore, music was played during the entirety of each session and was selected by a random draw by the investigator according to the participants’ selected genre of music based on the informal survey results. Based on these results the following genres were selected: 60’s, 70’s, 80’s radio, Christian, Country, and Pop music. The participants alternated on each exercise equipment every 15 minutes for an hour with a cool- down directed by the investigator. These proceedings continued for a total of four weeks and a post-PHQ-9 questionnaire was collected by the investigator.
3.2 Population and Sample
The population of this project included adult hypertensive patients between the ages of 18-65 years with various cardiovascular diseases (CVDs) and moderate-severe depression at a private cardiology practice centralized in rural Maryland. A convenience sample of 11 participants was utilized in this project. The average age of participants was 42.6 years (SD = 8.0) and the majority were female (63.6%), Hispanic (63.6%), and married or in a domestic partnership (54.5%) (Table 1). Approximately 72.7% were employed and 63.6% had some college or higher-level education while 36.4% had received their high school diploma or equivalent. Participants included in the study had HTN and some other form of CVD and were diagnosed with moderate-severe depression with the PHQ-9 assessment tool by the investigator. Specifically, five participants had coronary artery disease (CAD) status post percutaneous intervention with stent placement, two participants had CAD status post coronary artery bypass graft (CABG), one participant had peripheral arterial disease (PAD) and three participants had atrial fibrillation. Participants were also included if they were on anti-hypertensive and anti- depressant medications and were not new patients to the clinical practice. Participants with substance abuse, schizophrenia, or any other psychiatric disorders were excluded from this study.
Table 1: Characteristics of Study Population
|
N (%) |
M (SD) |
|
|
Age in years: |
42.6 (8.0) |
|
|
Gender: |
||
|
Male |
4 (36.4%) |
|
|
Female |
7 (63.6%) |
|
|
Race: |
||
|
Hispanic or Latino |
7 (63.6%) |
|
|
White |
3 (27.3%) |
|
|
Other or multi-racial |
1 (9.1%) |
|
|
Educational Background: |
||
|
High school diploma or equivalent |
4 (36.4%) |
|
|
Some college, no degree |
1 (9.1%) |
|
|
Trade/technical/vocational training |
2 (18.2%) |
|
|
Bachelor’s degree |
1 (9.1%) |
|
|
Master’s degree |
3 (27.3%) |
|
|
Marital Status: |
||
|
Single, never married, or domestic partnership |
5 (45.5%) |
|
|
Married or domestic partnership |
6 (54.5%) |
|
|
Employment: |
||
|
Unemployed |
2 (18.2%) |
|
|
Employed |
8 (72.7%) |
|
|
Retired |
1 (9.1%) |
Note: N = 11.
3.3 Instrumentation
Music therapy may have an impact on the patient’s psychological well-being. To determine whether music therapy was effective in reducing depression symptoms, the PHQ-9 was utilized. The PHQ-9 was administered to assess participants’ levels of depression at baseline and four-weeks post-intervention. The PHQ-9 is a 9-item self-assessment instrument to detect and monitor the severity of depression (Sun et al., 2020). This questionnaire is copyright by Pfizer, Inc. and does not require fees or permissions to use or copy. To determine validity and reliability a study conducted by Sun et al. (2020) was reviewed. This study examined the reliability and validity of the PHQ-9 tool by comparing it to the Hamilton Depression Scale (HAMD-17) on 109 inpatients and outpatients diagnosed with Major depressive disorder (MDD) (Sun et al., 2020). The results revealed that the PHQ-9 had a positive correlation to the HAMD- 17 total score (r = 0.610, p < 0.001) (Sun et al., 2020). The PHQ-9 in the Sun et al. (2020) study demonstrated good construct validity and proven reliability to distinguish between depressed and non-depressed patients as well as the severity of depressive symptoms (a= 0.89.2 and retest reliability r = 0.737).
3.4 Data Collection
Data collection for the clinical scholarly project (CSP) commenced from October 2020 to December 2020. The project was approved by the Institutional Review Board (IRB) at Brandman University (Appendix F). Recruitment of patients involved a complete health and physical assessment by the investigator to ensure they were eligible to participate. A total of 11 patients from a private cardiology practice in rural Maryland were recruited and consented. Demographic variables from each participant were collected by the investigator. Before initiation of the project, participants were asked to fill out a voluntary informal survey regarding their music preferences. Music was selected based on the participants’ music selection gathered from the surveys and was played during a one-hour exercise session conducted each Friday for a total of four weeks. Physiological changes were measured by systolic and diastolic blood pressure readings. Pre-exercise blood pressure using a manual blood pressure cuff was recorded by the investigator weekly for four weeks. Psychological measures included a self-report PHQ-9 for depression collected from participants at baseline and post-intervention at four weeks.
3.5 Data Analysis
Data analyses were performed using SPSS version 26.0. The sample consisted of two groups, pre-intervention and post-intervention utilizing the pre-exercise systolic and diastolic blood pressures and the PHQ-9 scores, with N = 11 in each group. A paired sample t test was used to test the differences in participants’ systolic and diastolic blood pressures and PHQ-9 scores before intervention compared to after the intervention was applied.
3.6 Summary
This was a quasi-experimental project designed to gain an understanding of how music may affect an individual’s blood pressure and depressive state. Participants were recruited from a private cardiology practice in rural Maryland with diagnoses of hypertension and moderate- severe depression based on the PHQ-9 criteria. Data were collected on pre-exercise systolic and diastolic blood pressure for four consecutive weeks. A pre-and post-intervention PHQ-9 score was assessed from each participant. Data were analyzed utilizing the SPSS version 26.0 and were reviewed to evaluate the efficacy of music therapy on blood pressure and depression scores.
CHAPTER 4
4.1 Findings
The participants for this project were described by number and percentage in each category for gender, education, marital status and employment with additional description of average age (SD). Paired t-tests assessed significance of decrease pre- versus post-intervention in average systolic and diastolic blood pressure and PHQ-9 depression score. All analyses were conducted using SPSS version 26.0. Average age of participants was 42.6 years (SD = 8.0), the majority were female (63.6%), Hispanic (63.6%), and married or in a domestic partnership (54.5%) (Table 1). Approximately 72.7% were employed and 63.6% had some college or higher- level education while 36.4% had received their high school diploma or equivalent. Average systolic blood pressure decreased pre- versus post-intervention from 120.4 (SD = 12.4) to 116.4 (SD = 9.5). This resulted in a mean decrease of -4.0 points (95% CI [-9.1, 1.4]), t(10) = -1.638, p = .132 (Table 2). Average diastolic blood pressure decreased by a smaller amount from 75.6 (SD = 7.2) to 74.0 (SD = 7.0). The mean decrease was -1.6 points (95% CI [-4.0, 0.8]), t(10) = -1.526, p = .158. Depression decreased significantly following the intervention from an average PHQ-9 score at baseline of 13.8 (SD = 3.3) to 5.7 (SD = 3.5) with a mean decrease of -8.1 (95% CI [- 11.2, -5.0]), t(10) = -5.843, p < .001 (Figure 1).
Table 2: Results of t-test for pre-and post- Blood Pressure by Music Intervention
|
Before Intervention |
After Intervention |
t(10) |
p |
Cohen’s d |
|||
|
Outcome |
M |
SD |
M |
SD |
|||
|
Systolic Blood Pressure |
120.4 |
12.4 |
116.4 |
9.5 |
-1.638 |
.132 |
0.362 |
|
Diastolic Blood Pressure |
75.6 |
7.2 |
74.0 |
7.0 |
-1.526 |
.158 |
0.225 |
Note: N = 11.
Figure 1: Patient Questionaire -9 (PHQ-9) pre - versus Music Intervention Scores
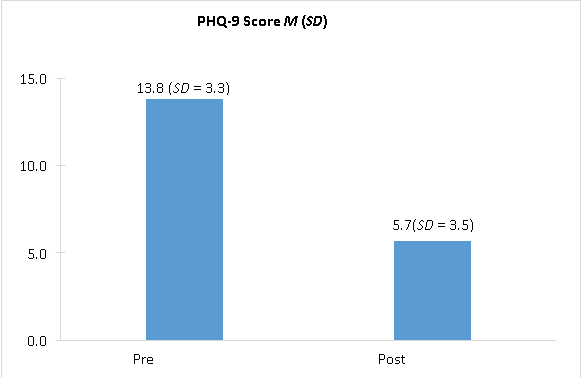
Note: Decrease in average depression pre- versus post-intervention (M = -8.1 (95% CI [-11.2, - 5.0]), t(10) = -5.843, p < .001.
CHAPTER 5
5.1 Implications
A paired sample t-test demonstrated the differences in participants’ systolic and diastolic blood pressure readings and Patient Health Questionnaire-9 (PHQ-9) depression scores before intervention compared to after the intervention was applied. There was a mean decrease of -4.0 points in systolic blood pressure and a decrease of -1.6 points in diastolic blood pressure post intervention. Even though these results yielded a reduction in blood pressures, the t-test revealed that there was no statistical significance in systolic blood pressure t(10) = -1.638, p = .132 and diastolic blood pressure t(10) = -1.526, p = .158 between pre- and post-intervention. There was a statistically significant reduction in PHQ-9 depression scores t(10) = -5.843, p < .001. In terms of the PHQ-9 scale score, this translated to a decrease in average depression from moderate to mild severity. The results of this project support that music therapy during an exercise program may have beneficial effects on blood pressure and depression severity in patients with CVD. These findings are considered clinically significant as uncontrolled blood pressure and depression are associated with an increased risk of developing CVD and may affect the outcomes of patients with CVD or post cardiovascular events (Leung et al., 2015; Meijer et al., 2013; Smolderen, 2017; Wu et al., 2015). Implementing music therapy may serve as an alternative intervention to enhance blood pressure and depression symptoms that is non-invasive, cost-effective and without adverse effects. Moreover, the project results provide a foundation to call for change in clinical practice by establishing a holistic approach in the management of patients with chronic diseases and mental disorders. CVD and mental health disorders are a growing concern on a national and global level. A collaborative approach to the management of individuals with these conditions should be considered in clinical practice to ensure improvement in healthcare outcomes.
5.2 Supporting Evidence for Advanced Practice Registered Nursing
The implication of advanced practice registered nurses (APRNs) arose from an increasing need in healthcare practice (Walker & Polancich, 2015). Recent attention from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) and the Institute of Medicine (IOM) cited the urgency for rigid concentration on safe practice to diminish the risk of patient sentinel events that established the demand of APRNs in the healthcare field (Walker & Polancich, 2015). As a result, one essential proposal was to apply evidence-based practice (EBP) (Stevens, 2013). EBP is focused on the application of up-to-date research into routine patient care to optimize patient outcomes (Stevens, 2013). It signifies a fundamental conclusion that research generates the greatest trustworthy information that the probability that a given intervention will modify a patient’s current health condition into a desirable outcome (Stevens, 2013).
APRNs are highly prepared to provide changes in their clinical practices and transform the healthcare field. As such, APRNs have to be diligent in advocating for patients when a gap in practice has been identified. With the knowledge and skills APRNs have developed through continuing education and practice, APRNs can provide advancements in clinical practice initiatives, provide excellence in nursing care and translate evidence-based medicine that is essential with the emanate progression in healthcare (Walker & Polancich, 2015).
Recognizing the need of reducing risk factors that may lead to worsening CVD or secondary cardiac events led to a devotion to addressing these areas for this CSP. This CSP focused on utilizing music therapy during an exercise program to reduce blood pressure and depressive symptoms in adult hypertensive patients with cardiovascular disease. On a national level, quality management initiatives for CVD and mental health disorders aim to reduce the burden of these diseases as well as morbidities and mortalities through modification of risk factors for prevention, detection and treatment (De Hert, 2018; HealthyPeople, 2020; Mensah & Collins, 2015). Some of the national objectives for HealthyPeople (2020) include the expansion of comprehensive cardiovascular healthcare, decreasing coronary heart disease (CHD) related deaths and increasing the number of referrals to cardiac rehabilitation for myocardial infarction (MI) survivors at discharge. As such, this CSP aligned with HealthyPeople (2020) objectives HDS-1, “(Development) Increase overall cardiovascular health in the U.S. population” (p.1), HDS-2, “Reduce coronary heart disease deaths,” (p.1) MHMD-4, “Reduce the proportion of persons who experience major depressive episodes (MDEs),” (p.2) and MHMD-9, “Increase the proportion of adults with mental health disorders who receive treatment” (p.4).
5.3 Limitations
There were certain limitations to this clinical scholarly project (CSP). One limitation was that there was only one investigator in this project who assumed responsibility in implementing the intervention and collecting the data, which potentially may bias the results. For that reason, it is recommended to distribute responsibilities amongst various researchers. Also, participants in the project were on anti-hypertensive and anti-depressant medications and adjustments to their medications during the four weeks were not noted which may also have a bias in the results.
Thus, it is recommended that researchers consider changes to participants’ medication regimes for future analysis. Another limitation was the time frame the study was conducted was limited to four weeks. As such, the sustainability of the results was not assessed. Therefore, it is recommended future studies also include a post-intervention follow-up. Due to the COVID-19 pandemic, recruitment was difficult resulting in a small sample. Thus, the results of this project could not be generalized, which may affect external validity.
5.4 Sustainability
The sustainability of a clinical research project into healthcare practice should be planned at the beginning stage of any project (Feldstein & Glasgow, 2008). It is also important to identify key stakeholders that will care about the outcomes of the project to have full and ongoing support early in the planning process (Kleinpell, 2017). Individuals desiring to implement a change project should allocate sources of support that are dedicated to the cause as they are (Kleinpell, 2017). The goals of the project and the roles and responsibilities of each stakeholder should be communicated across all department levels (Feldstein & Glasgow, 2008). Other essential components to sustain project implementation in practice include initiating a framework for encouraging dissemination, allocating exceptional practices, monitoring project outcomes, modifying processes appropriately, and providing adaptability of protocols (Feldstein & Glasgow, 2008).
This clinical scholarly project (CSP) will maintain sustainability at the private cardiology practice it was implemented in through various channels. First, a policy to implement routine depression screening to identify at-risk populations will be discussed with the stakeholders in addition to a music therapy protocol. The private cardiology practice is currently changing to reintroduce cardiac rehabilitation (CR) for their eligible patients. With approval from the stakeholders, the music therapy protocol will be implemented in the CR program. Staffing will be trained to define objectives and distribute team member roles and responsibilities.
Communication is vital in sustaining change and this may be accomplished through quarterly face-to-face meetings and weekly updates via email (Kleinpell, 2017). Communication provides opportunities for ongoing assessment, feedback, assists in addressing issues that may arise, and allows for policy adjustments (Feldstein & Glasgow, 2008; Kleinpell, 2017). Once the project is adopted into practice, a maintenance infrastructure should be established (Feldstein & Glasgow, 2008). To do so, it will be proposed that the clinical practice initiate yearly competencies for staff. Also, bi-annual performance reviews will allow for modifications to the protocols and/or procedures (Feldstein & Glasgow, 2008). As noted, meticulous project planning is essential in sustaining change in practice.
A cost-benefit analysis (CBA) should also be considered for sustainability into practice which includes staffing, total project hours, equipment, and training in addition to the outcome benefits (Table 3). Per the clinical practice’s policy, CR will consist of one hour of monitored physical activity by trained professionals for a total of 36 sessions. The trained professionals administering CR to the patients will be an exercise physiologist and a registered nurse (RN). To incorporate music therapy in CR, a hired music therapist was included in the CBA. The salaries for all staff as well as the music therapist were determined by average salaries across the nation for these positions to avoid intrusion of staff’s personal information. Included in the costs for the exercise physiologist and RN was their hourly salary rate multiplied by a total of 36 CR sessions. The music therapist costs were configured by a total of 10 visits with the breakdown as follows:
1) an initial group training session for all involved parties, 2) one-hour visits three days a week for the first week, 3) one-hour visit one day a week for the following four weeks, 4) one-hour visit monthly for the remaining two months. Essential equipment required for music therapy as well as CR is readily available in clinical practice, thus no costs were inquired with these items. Printing costs were determined by the average costs of one box of copying and/or printing paper. Also included were costs for refreshments for meetings with a total of four quarterly meetings per year. Lastly, the benefits section in Table 3 includes the average amount of health insurance reimbursement per CR session. Also, included was the number of patients receiving CR in one session multiplied by the 36 sessions according to the current clinical practice’s policy. The total cost for implementing music therapy in CR amounted to $2,578.16 and the total benefit is $19,800. This CBA identified the cost-effectiveness of implementing music therapy in CR as well as the potential financial gains of doing so.
Table 3: Cost-Benefit Analysis of Music Therapy in Cardiac Rehabilitation
|
Cost-Benefit Analysis for Music Therapy in Cardiac Rehabilitation |
||||
|
Costs |
||||
|
Category |
Item |
Qty |
Price |
Total |
|
Staffing |
CR Exercise Physiologist |
36 |
$21.28/hour |
$766.08 |
|
CR Registered Nurse |
36 |
$39.06/hour |
$1406.16 |
|
|
Music Therapist |
10 |
$23.12/hour |
$231.12 |
|
|
Equipment |
Treadmill |
2 |
n/a |
$0 |
|
Stationary Bicycle |
2 |
n/a |
$0 |
|
|
Upper Body Cycle |
2 |
n/a |
$0 |
|
|
Audio System |
1 |
n/a |
$0 |
|
|
Printing |
Stationary/printing |
1 |
$35 |
$35 |
|
Focus Group |
Refreshments |
4 meetings |
$35 |
$140 |
|
Training |
Group Training |
10 sessions with Music Therapist |
$23.12/hour |
Calculated Above |
|
Total Cost: |
$2578.16 |
|||
|
Benefits |
||||
|
Average insurance reimbursement per cardiac rehabilitation session |
$110 |
|||
|
Average patients receiving cardiac rehabilitation per session |
5 |
|||
|
Number of cardiac rehabilitation sessions |
36 |
|||
|
Total Benefit: |
$19,800 |
|||
5.5 Dissemination
Health care change initiatives begin with identifying a problem and researching evidence- based interventions to assess potential solutions. Acquiring new knowledge is merely the beginning as one must translate the discovered research into clinical practice (American Association of Colleges of Nursing [AACN], 2006). The dissemination and assimilation of this new research are paramount in enhancing patient safety, satisfaction, and clinical outcomes (AACN, 2006). This clinical scholarly project (CSP) will be disseminated in several formats.
First, the finished manuscript will be made available to the Brandman University Library for open access to interested parties. In addition, the results of the CSP will be shared with pertinent stakeholders of the clinical practice in which the project was conducted. An abstract of the CSP will also be submitted to the American Psychiatric Nurses Association (APNA) annual conference. If the abstract is accepted by the APNA, the results of the project will be presented as a poster at the conference and disseminated on a national platform.
5.6 Application of the Essentials
The Doctor of Nursing Practice (DNP) Essentials provides the foundation of academic components and competencies that are required in programs bestowing the DNP degree (AACN, 2006). These essentials address the fundamental core competencies that apply to all advanced nursing practice functions (AACN, 2006). In considering this, several DNP Essentials were met while engaging in the clinical scholarly project (CSP)..
Scientific underpinnings illustrate DNP Essential I and demonstrates the intricacy of nursing practice at the highest level of education enriched in a tradition that is the conceptual framework of nursing (AACN, 2006). This Essential recognizes the need to incorporate natural and social sciences to expand nursing knowledge and guide practice (AACN, 2006). As such, DNP graduates will be able to assimilate nursing science with an array of expertise and utilize scientific theories and concepts to differentiate the magnitude of health and health care delivery systems (AACN, 2006). In addition, DNP graduates can identify interventions to improve and evaluate health outcomes and health care delivery (AACN, 2006). As such, this DNP Essential was applied to the CSP through vigorous and meticulous literature review to ensure that the evidence in the sciences supported the intervention. Also, collaborating with health care disciplines with extensive experience and knowledge in planning the design of the project and coordinating activities met the criteria for this DNP Essential. Other activities that outlined this Essential included the evaluation of the outcomes of the project and determining areas that may need modifications for the future development of clinical protocol and policy.
Organizational and systems leadership defines DNP Essential II and provides the foundation for DNP graduates to make changes in the health care system to improve both patient and health outcomes (AACN, 2006). DNP graduates will be able to comprehend the concepts of practice management and provide theoretical and practical approaches to balance work output with efficacious care (AACN, 2006). This DNP essential ultimately focuses on practice, continuous improvement of patient outcomes and safety (AACN, 2006). In essence, DNP essential II provided the foundation of fine-tuning leadership skills in implementing project activities. Some project activities that enhanced leadership skills were a collaboration with the chair of the project and the clinical practice owner in the design and processes of the CSP. Other project activities that improved leadership skills were mentorship for essential team members, providing background and education on the intervention, training of staff members, and distributing roles and responsibilities among key team members to attain a common goal.
The DNP Essential VI prepares graduates to engage in direct and collective communication and skills to form and apply peer review, practice models and guidelines, policy changes, and standards of care (AACN, 2006). DNP graduates will be able to expand their roles as leaders guiding multidisciplinary teams in the examination of complexities in clinical practice as well as problems in organizations (AACN, 2006). As a result, DNP graduates will be able to establish modifications in the care of patients and health care systems (AACN, 2006). Applying DNP Essential VI was imperative throughout the planning and coordinating phases of the CSP. Some project activities that incorporated this Essential were providing leadership to relevant staff that participated in the CSP by providing education, training and direction to facilitate project goals. Other project activities included collaborating with the chair and stakeholders to implement the CSP, discussing the progression of the project, and developing and preparation for defense for the CSP intervention. In addition, a meeting with the clinical practice owner was scheduled to discuss the outcomes of the project and possibilities for establishing a protocol for music intervention and policy changes within the clinical practice.
REFERENCES
-
Aalbers S, Spreen M, Pattiselanno K, Verboon P, Vink A, et al. (2020). Efficacy of emotion-regulating improvisational music therapy to reduce depressive symptoms in young adult students: A multiple-case study design. The Arts in Psychotherapy. 71:101720. doi: 10.1016/j.aip.2020.101720.
-
American Association of Colleges of Nursing. [AACN]. (2006). DNP essentials. https://www.aacnnursing.org/DNP/DNP-Essentials
-
American Heart Association. (2017). Cardiovascular disease: A costly burden for America projections through 2035. https://www.heart.org/en/get-involved/advocate/federal-priorities/cardiovascular-disease-burden-report
-
American Music Therapy Association. (2021). Frequently asked questions. https://www.musictherapy.org/faq/#267
-
Anne Arundel County [AAC]. (2014). Anne arundel county health data by councilmanic districts and zip codes. https://aahealth.org/wp-content/uploads/2017/08/healthdata-by-district- 2014.pdf
-
AAC. (2019). Community health needs assessment (CHNA) 2019. https://www.aahealth.org/wp-content/uploads/2019/02/CHNA2019.pdf
-
Anne Arundel County Department of Health [AACDH]. (2020). Anne arundel county department of health report card 2020. https://aahealth.org/pdf/aahealthreportcard2020.pdf
-
Antonakoudis H, Kifnidis K, Andreadis A, Fluda E, Konti Z, et al. (2006). Cardiac rehabilitation effects on quality of life in patients after acute myocardial infarction. Hippokratia. 10(4):176-181.
-
Basogul C and Buldukoglu K. (2020). Neuman systems model with depressed patients: A randomized controlled trial. Nursing Science Quarterly. 33(2):148-158. doi: 10.1177/0894318419898172.
-
Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, et al. (2019). Heart disease and stroke statistics-2019 Update. American Heart Association Circulation. 139:e56-e528. doi: 10.1161/CIR.0000000000000659
-
Biasutti M and Mangiacotti A. (2021). Music training improves depressed mood symptoms in elderly people: A randomized controlled trial. International Journal of Aging & Human Development. 92(1):115–133. doi: 10.1177/0091415019893988.
-
Bowles L, Curtis J, Davies C, Lengerich A, and Bugajski A. (2019). The effect of music on mood, motivation, and exercise among patients in a cardiac rehabilitation program: A pilot study. Nursing Forum. 54:340-344. doi: 10.1111/nuf.12334.
-
Bradt J, Dileo C, and Potvin N. (2013). Music for stress and anxiety reduction in coronary heart disease patients. Cochrane Database of Systematic Reviews, 12:1-104. doi: 10.1002/14651858.CD006577.pub3.
-
Centers for Disease Control and Prevention [CDC]. (2017). Heart disease fact sheet. https://www.cdc.gov/heartdisease/facts.htm
-
CDC. (2020, September 8). Facts about hypertension. https://www.cdc.gov/bloodpressure/facts.htm
-
CDC. (2020a, November 18). Mental health. https://www.cdc.gov/nchs/fastats/mental-health.htm
-
CDC. (2012). Mental health and chronic diseases. https://www.cdc.gov/workplacehealthpromotion/tools-resources/pdfs/issue-brief-no-2-mental-health-and-chronic-disease.pdf
-
Chan MF, Chan EA, Mok E, and Kwan Tse FY. (2009). Effect of music on depression levels and physiological responses in community-based older adults. Int J Ment Health Nurs. 18:285-294. doi: 10.1111/j.1447-0349.2009.00614.x.
-
Chang H-K, Peng T-C, Wang J-H, and Lai H-L. (2011). Psychophysiological responses to sedative music in patients awaiting cardiac catheterization examination: A randomized controlled trial. J Cardiovasc Nurs. 26(5):E11–E18. doi: 10.1097/JCN.0b013e3181fb711b.
-
Davidson K. (2012). Depression and Coronary Heart Disease. ISRN Cardiology. 1-18. doi: 10.5402/2012/743813.
-
De Hert M, Detraux J, Vancampfort D. (2018). The intriguing relationship between coronary heart disease and mental disorders. Dialogues Clin Neurosci. 20(1):31-39.
-
Feldstein AC and Glasgow RE. (2008). A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. The Joint Commission Journal on Quality and Patient Safety. 34(4):228-243.
-
Gathright EC, Goldstein CM, Loucks EB, Busch AM, Stabile L, et al. (2019). Examination of clinical and psychosocial determinants of exercise capacity change in cardiac rehabilitation. Heart & Lung. 13:13-17.
-
Gogate MD and Patil NR. (2019). Effects of musical therapy and physiotherapy in pregnancy induced hypertension. Indian Journal of Public Health Research & Development. 10(8):339–343.
-
Grove SK, Gray JR, and Burns N. (2015). Understanding nursing research: Building an evidence-based practice. (6th ed.). Elsevier.
-
HealthyPeople. (2020, April 17). Heart disease and stroke. https://www.healthypeople.gov/2020/topics-objectives/topic/heart-disease-and-stroke
-
HealthyPeople. (2020, August 20). Topics and objectives. https://www.healthypeople.gov/2020/topics-objectives
-
Kleinpell R-M. (2017). Outcome assessment in advanced practice nursing. Springer Publishing Company.
-
Kunikullaya KU, Goturu J, Muradi V, Hukkeri PA, Kunnavil R, et al. (2015). Music versus lifestyle on the autonomic nervous system of prehypertensives and hypertensives—a randomized control trial. Complementary Therapies in Medicine. 23(5):733–740. doi: 10.1016/j.ctim.2015.08.003.
-
Leung YW, Flora DB, Graverly S, Irvine J, Carney RM, et al. (2015). The impact of pre- morbid and post-morbid depression onset on mortality and cardiac morbidity among coronary heart disease patients: A meta-analysis. Psychosom Med. 74(8):786-801. doi: 10.1097/PSY.0b013e31826ddbed.
-
Liu Y and Petrini MA. (2015). Effects of music therapy on pain, anxiety, and vital signs in patients after thoracic surgery. Complementary Therapies in Medicine. 23(5):714–718. doi: 10.1016/j.ctim.2015.08.002
-
Loomba RS, Shah PH, Chandrasekar S, Arora R, Molnar J. (2012). Effects of music on systolic blood pressure, diastolic blood pressure, and heart rate: a meta-analysis. Indian Heart J. 309-313. doi: 10.1016/S0019-4832(12)60094-7.
-
McCance KL and Huether SE. (2015). Pathophysiology: the biologic basis for disease in adults and children. St. Louis: Mosby.
-
McKinney CH and Honig TJ. (2017). Health outcomes of a series of bonny method of guided imagery and music sessions: A systematic review. Journal of Music Therapy. 1:1.
-
Meijer A, Conradi HJ, Bos EH, Anselmino M, Carney RM, et al. (2013). Adjusted prognostic association of depression following myocardial infarction with mortality and cardiovascular events: Individual patient data meta-analysis. The Br J Psychiatry. 203:90-102. doi: 10.1192/bjp.bp.112.111195.
-
Mensah GA and Collins PY. (2015). Understanding mental health for the prevention and control of cardiovascular disease. Global Heart. 10(3):221-224. doi: 10.1016/j.gheart.2015.08.003.
-
Metzger LK. (2004). Assessment of use of music by patients participating in cardiac rehabilitation. Journal of Music Therapy. 41(1):55-69.
-
Muntner P, Shimbo D, Carey RM, Charleston JB, Gaillard T, et al. (2019). Measurement of blood pressure in humans: A scientific statement from the American heart association. American Heart Association Circulation. 73:e35- e66. doi: 10.1161/HYP.0000000000000087.
-
Nadar S-K, Tayebjee M-H, Messerli F, and Lip G. (2006). Target organ damage in hypertension: Pathophysiology and implications for drug therapy. Curr Pharmaceutical Design. 12(13):1581-1592. doi:10.2174/138161206776843368.
-
Nursing Theory. (2016). Neuman’s system model. https://www.nursing-theory.org/theories-and- models/neuman-systems-model.php
-
Nystoriak MA and Bhatnagar A. (2018). Cardiovascular effects and benefits of exercise. Frontiers in Cardiovascular Medicine. 5(135):1-11. doi: 10.3389/fcvm.2018.00135.
-
Riva JJ, Malik KM, Burnie SJ, Endicott AR, and Busse JW. (2012). What is your research question? An introduction to the PICOT format for clinicians. The Journal of the Canadian Chiropractic Association. 56(3):167–171.
-
Saklayen MG and Deshpande NV. (2016). Timeline of history of hypertension treatment. Frontiers in cardiovascular medicine. 3:3. doi: 10.3389/fcvm.2016.00003.
-
Smolderen KG. (2017). Coping after an acute myocardial infarction: The role of depression and anxiety. American College of Cardiology. 1-10.
-
Soares do Amaral MAS, Neto MG, de Queiroz JG, Martins-Filho PRS, Saquetto MB, et al. (2016). Effect of music therapy on blood pressure of individuals with hypertension: A systematic review and Meta-analysis. International Journal of Cardiology. 214:461–464. doi: 10.1016/j.ijcard.2016.03.197.
-
Stevens CJ and Dascombe BJ. (2015). The reliability and validity of protocols for the assessment of endurance sports performance: An updated review. Measurement in Physical Education & Exercise Science. 19(4):177–185.
-
Stevens KR. (2013). The impact of evidence-based practice in nursing and the next big ideas. The Online Journal of Issues in Nursing. 18(2):1-12. doi: 10.3912/OJIN.Vol18No02Man04.
-
Stewart JC, Perkins AJ, and Callahan CM. (2014). Effect of collaborative care for depression on risk of cardiovascular events: Data from the IMPACT randomized controlled trial. Psychosom Med. 76(1):29-37. doi: 10.1097/PSY.0000000000000022.
-
Sumner J, Harrison A, and Doherty P. (2017). The effectiveness of modern cardiac rehabilitation: A systematic review of recent observational studies in non-attenders versus attenders. Plos One. 12(5):1-14. doi: 10.1371/journal.pone.0177658.
-
Sun Y, Fu Z, Bo Q, Mao Z, Ma X, and Wang C. (2020). The reliability and validity of PHQ-9 in patients with major depressive disorder in psychiatric hospital. BMC psychiatry. 20(1):474. doi: 10.1186/s12888-020-02885-6.
-
Thombs BD, Bass EB, Ford DE, Stewart KJ, Tsilidis KK, et al. (2005). Prevalence of depression in survivors of acute myocardial infarction. J Gen Int Med. 21:30-38. doi: 10.111/j.1525- 1497.2005.00269x.
-
Vaccarino V, Badimon L, Bremner JD, Cenko E, Cubedo J, et al. (2020). Depression and coronary heart disease: 2018 ESC position paper of the working group of coronary pathophysiology and microcirculation. Eur Heart J. 41(17):1687-1696. doi: 10.1093/eurheartj/ehy913.
-
Walker D-K and Polancich S. (2015). Doctor of nursing practice: The role of the advanced practice nurse. Seminars in Oncology Nursing. 31(4):263-272. doi: 10.1016/j.soncn.2015.08.002
-
Winerman L. (2017). By the numbers: The cost of treatment. Monitor on Psychology. 48(3):80. https://www.apa.org/monitor/2017/03/numbers
-
World Health Organization [WHO]. (2017). Cardiovascular diseases (CVDs). https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
-
WHO. (2020). Global hearts initiative, working together to promote cardiovascular health. https://www.who.int/cardiovascular_diseases/global-hearts/en/
-
Wu CY, Hu HY, Chou YJ, Huang N, Chou YC, et al. (2015). High blood pressure and all-cause and cardiovascular disease mortalities in community-dwelling older adults. Medicine. 94(47):e2160. doi: 10.1097/MD.0000000000002160.