Information Links
Related Conferences
Previous Issues Volume 10, Issue 3 - 2025
The Pathophysiology of Esophageal Achalasia, As Described by The Chicago Classification, Corresponds in Most Cases to GERD
Michael D Levin*
Dorot. Medical Center for Rehabilitation and Geriatrics, Netanya, Israel
*Corresponding Author: Michael D Levin, MD, Ph.D, Dorot. Medical Center for Rehabilitation and Geriatrics, Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus, Dorot. Medical Center for Rehabilitation and Geriatrics, Amnon veTamar, Netanya, Israel, Tel: 972-538281393, Email: [email protected]
Received Date: November 10, 2025
Published Date: November 25, 2025
Citation: Levin MD. (2025). The Pathophysiology of Esophageal Achalasia, As Described by The Chicago Classification, Corresponds in Most Cases to GERD. Mathews J Gastroenterol Hepatol. 10(3):36.
Copyrights: Levin MD. © (2025).
ABSTRACT
Background: Adoption of high-resolution manometry (HRM) and the Chicago Classification has led to a dramatic increase in the diagnosis of esophageal achalasia. To determine the cause of this phenomenon, we decided to examine pathophysiologic distinctions between gastroesophageal reflux disease (GERD) and esophageal achalasia (EA), diagnosed using HRM. Methods: We reviewed radiographic, manometric, endoscopic, and histologic markers of gastroesophageal junction (EGJ) disease. We contrasted HRM-based diagnoses with radiographic studies with maximum provocation, с histologic criteria and reviewed outcomes following myotomy/POEM. Results: HRM was introduced as a method for studying esophageal pressure by engineers and physicians ignorant of normal and pathological physiology. The selection of the control group was carried out in violation of scientific methodology, and diagnostic parameters were selected by a vote of individuals interested in the widespread use of recording equipment. Radiographic studies with maximal provocation allow one to measure with mathematical precision the width of the esophagus, the length of the lower esophageal sphincter (LES) and pathological esophageal sphincters. Histological studies may identify shortening of the intra-abdominal lower esophageal sphincter, peptic stenosis, or mucosal change (squamo-oxyntic gap) consistent with GERD. Comparison of EA diagnostic results by different methods revealed that HRM most often diagnoses EA, whereas based on radiographic examinations with maximum provocation typical cases of GERD were diagnosed. Significant rates of reflux/esophagitis after LES myotomy procedures, particularly POEM, were found. Transection of the LES permanently eliminates residual anti-reflux competence and predisposes patients to clinically significant GERD. Conclusions: HRM is not a scientifically validated method. It diagnoses EA in patients with GERD, which is an indication for treatment, as if the patient had true GERD. Dissection of a weak but functioning LES permanently destroys the antireflux function of the LES, which worsens the prognosis. Radiographic diagnostics using maximum provocation allows for the mathematically accurate diagnosis of GERD and true EA. Scientific discussion is needed to determine the best diagnostic and treatment options for patients with GERD.
Keywords: Gastroesophageal Reflux Disease, Esophageal Achalasia, X-Ray Diagnosis, High-Resolution Manometry, Pathophysiology of Esophageal Gastric Junction, Peroral Endoscopic Myotomy, Blown-Out Myotomy.
INTRODUCTION
Since high-resolution manometry (HRM) practitioners do not utilize knowledge of the anatomy and physiology of the esophagus and its sphincters, it is necessary to briefly review this scientific knowledge, without which it is impossible to evaluate the different research methods.
Anatomy and physiology of the esophagus
The esophagus transports food from the pharynx to the stomach. It is located between the upper esophageal sphincter (UES) and the lower esophageal sphincter (LES). The food bolus moves by peristalsis in a craniocaudal direction. In 1899, the famous English physiologists Bayliss and Starling published the law of the intestine, which explained the peristaltic movement of the esophagus. This law almost immediately became one of the foundation stones of physiology, about which there has never been any question or argument. In the first article, the following statement was formulated: “Excitation at any point in the gut excites contraction above, inhibition below. This is the law of the intestine” [1]. The UES and LES are muscular valves that allow bolus to move caudally and contract to prevent retrograde movement. They also obey the law of the intestine, opening when pressure rises cranially and contracting when pressure rises caudally in relation to the sphincters [2,3]. All participants in the bolus advancement have normal parameters (localization, tone, length and width). Some well-known parameters are listed below. The UES is defined as high-pressure zone, determined by manometry, maybe 2.5 to 4.5 cm in length [3]. The true length of the LES in adults, measured on radiographs of individuals without obvious pathology of the digestive system, turned out to be the same as in manometric studies [4]. The length of the LES in patients of different ages is presented in Table 1.
Table 1. Normal length LES in different age groups
|
Length of lower esophageal sphincter (cm) |
||||||
|
Age |
Up to 1 year |
1–3 years |
4–7 years |
8–10 years |
11–15 years |
21–65 years |
|
Limits |
0.7 – 1.0 |
1.2 – 1.5 |
1.5– 1.8 |
1.9 – 2.3 |
2.3 – 2.9 |
3.2 – 4.2 |
|
mean ± SEM |
0.86 ± 0.03 |
1.40 ± 0.02 |
1.72 ± 0.07 |
2.10 ± 0.05 |
2.45 ± 0.11 |
3.60 ± 0.08 |
In healthy children, the average esophageal diameter at the cranial measurement point was 6.75 mm at the lowest body weight (2.6 kg) and 14 mm at a body weight of 74 kg [5]. In adults, the width of the esophagus normally does not exceed 15 mm [4].
Physiology of the esophagus in radiographic examination
Radiographic examination is a demonstrative and physiological method, as it does not affect the gastrointestinal tract's function and clearly depicts the anatomy and physiology of the esophagus and sphincters. During a standard examination, the contrast agent normally moves very rapidly into the stomach. Therefore, neither the width of the esophagus nor the length of the LES can be determined. Given the physiology of the LES, whose tone increases in response to increased gastric pressure, we performed a radiograph of the esophagogastric junction (EGJ) during barium ingestion after ≈ 30 seconds of continuous abdominal compression. Abdominal compression causes contraction of the LES, which is defined as the gap between the contrast-enhanced esophagus and stomach (Figure 1a). A 30-second delayed radiograph can only determine the length of the LES, since the crural diaphragm (CD), being a striated muscle, quickly fatigues and relaxes after 15-18 seconds (mean 16.8 ±1.2) [6].
.png)
Figure 1. (a) Radiograph of the patient in an upright position taken during abdominal compression. The LES contracted in response to the increased pressure in the stomach. It is visible as a gap without contrast between the esophagus and stomach. Since the actual height of D-10 is ≈2 cm, the actual length of the LES is ≈3.4 cm. The LES parts: red - the abdominal segment, blue - inside the diaphragm, yellow - above the diaphragm. (b) Three-dimensional model of the EGJ [7]. The length of the LES is 3.4 cm (blue). Its abdominal part is ≈2 cm. About 1 cm is located at the level of the CD and 0.4 cm above the diaphragm.
Since the results of measuring the length of the LES in control adults are almost identical when measured by X-ray (3.60±0.08 cm), when using a three-dimensional model (3.4 cm) and a manometric study by pulling an open catheter (3.4-4.0 cm) is evidence of a close approximation to the actual norm. Secondly, radiographic studies have confirmed that increased gastric pressure does not cause relaxation, but a contraction of the LES to prevent reflux of an aggressive gastric chyme into the esophagus and belching too [8]. Furthermore, these studies are consistent with the law of the intestine.
Pathogenesis and pathophysiology of gastroesophageal reflux disease
There is no doubt that GERD results from damage to the LES and esophagus by aggressive gastric chyme, which contains hydrochloric acid and pepsin. Except for premature infants born with an immature LES, the disease begins gradually, beginning with chyme penetration only into the intra-abdominal portion of the LES. The disease process was traced by Chandrasoma and DeMeester [9]. Based on histological studies of the EGJ mucosa, they found that the normal state the esophageal squamous epithelium transitions to gastric oxyntic epithelium with no intervening cardiac epithelium. Because of gastric juice, cardiac metaplasia of the squamous epithelium of the esophagus occurs. Cardiac epithelium initially appears in the intraabdominal portion of the LES. However, as the process progresses, an increasing portion of the squamous epithelium converts to cardiac epithelium. At lengths >15 mm, reflux is severe, with increasingly uncontrollable symptoms. They also proved that the inflammatory process leads to expansion of the intraabdoninal part of the LES. The length of the squamo-oxyntic gap in the dilated distal esophagus, containing cardiac epithelium, is concordant with the shortening of the abdominal segment of the LES [9]. Although Chandrasoma and DeMeester's findings, published in numerous articles, have not been refuted, they are not cited. They are ignored because they challenge current concepts of GERD pathophysiology. First, the appearance of cardiac epithelium in the intra-abdominal portion of the LES does not mean: (1) that cardiac epithelium normally lines the proximal stomach; (2) that the stomach has risen cranially as a result of shortening of the esophagus; (3) that the GEJ is defined by the proximal limit of rugal folds, because the inflammatory response leads to edema and thickening of the LES wall, and folds appear in the LES, not the stomach. Secondly, since the disease begins with the penetration of gastric chyme only into the intra-abdominal part of the LES, i.e., the chyme does not enter the esophagus, therefore, during this period the acid cannot be determined by pH monitoring, (1) which excludes the possibility of functional reflux; (2) which indicates the low reliability of pH monitoring. Radiographic and manometric studies fully confirm the results of the histological studies by Chandrasoma and DeMeester. Manometric studies with catheter pull-through have demonstrated that in GERD, the length of the LES is shortened due to the length of the abdominal segment [10,11]. Figure 2 shows the shortening of the LES under different loads.
.png)
Figure 2. Radiographs of the EGJ in patients with GERD. (a). Before provocation. (b). During the water-siphon test, the LES between two red dots opened. Its length is 1.6 cm. The angle of His became obtuse. (c) Short LES without abdominal compression (2 cm vs 3.6 cm). (d) In the same patient with abdominal compression the LES length is 1 cm. (e) The opening of the LES in the form of a beak of the stomach is seen without provocation. The angle of His is obtuse.
These typical studies show that (1) Regardless of swallowing and pressure in the stomach, the distal point of the esophagus does not change its position, i.e., the length of the esophagus does not change; (2) Damage to the LES is manifested by its shortening mainly due to the opening of the intra-abdominal part of the LES. Those authors who call the "esophagus + LES" complex the esophagus come to false statements about shortening of the esophagus and displacement of the LES into the chest cavity [12]; (3). The degree of damage varies from slight shortening of the LES during maximum provocation to complete chalasia (gaping of the EGJ). During ontogenesis, the degree of damage to the LES increases. (4). In GERD, when the LES is unable to prevent reflux of gastric chyme, the pH of the chyme is not significant, since if it ensures the destruction of food proteins, it damages the wall of the esophagus. (5). An increase in the angle of His is not a cause of GERD, but evidence of LES shortening (Figure 3).
.png)
Figure 3. (a-b) Radiographs of the EGJ during barium ingestion in a horizontal position in patient with GERD. Since the true height of D10 (red line) is ≈ 2 cm, the length of the contracted part of the LES is 1 cm. The intra-abdominal portion of the LES between the contracted part of the LES and the blue line is opened. (b) For the last peristaltic wave to expel the barium into the stomach, the proximal sphincter (PS) closes the ampulla proximally. Therefore, the contracting ampulla was able to create a pressure higher than the gastric pressure, open the LES, and inject the bolus into the stomach. (c-d) Schem of the EGJ in normal (c) and in GER (d). Damage to the LES by the refluxate resulted in esophageal dilation with ampulla formation, shortening of the LES, an increase in the angle of His, and a decrease in the gastric gas bubble. (e-f) Radiographs of the gastric gas bubble in a healthy individual (e). In a patient with GER, the gas bladder is very small due to the escape of swallowed air with belching (f).
Clinical forms of GERD
To understand how different clinical forms of GERD arise, it is necessary to dwell on the etiology of this disease. The overproduction of acid and the associated illnesses linked to hypersecretion have a lifetime prevalence of 25-35% in the United States [13]. Acid-related diseases include inflammatory and ulcerative processes in the stomach and duodenum, which have become less common since the introduction of acid-suppressing drugs. GERD can be compared to the tip of an iceberg, which, despite conservative treatment, manifests with symptoms that reduce quality of life. This is because, unlike the stomach and duodenum, the esophagus lacks protection from acid and pepsin. Patients with acid-related diseases differ from other parts of the population in that they produce an excess amount of hydrochloric acid, which is not blocked by protective mechanisms. Previous studies have shown that lactose provokes hypersecretion of hydrochloric acid in most patients with GERD [14-16]. This is not surprising given that 36% of the population in the United States is genetically determined to have lactose intolerance (LI). In the United States, approximately three fourths of African Americans have the potential for symptoms of lactose intolerance [17]. In infants with lactose intolerance, GERD develops with early weaning from breastfeeding and manifests as infantile colic. The pain subsides at 4-6 months of age, but by this time, LES function is impaired, and this can manifest with clinical symptoms at any time throughout life. As shown previously, GERD can develop for many years without significant symptoms. Most young people don't associate the onset symptoms with dairy consumption, as heartburn doesn't appear immediately after consuming them. Only with a gaping EGJ, when acid enters the esophagus almost immediately after it forms in the stomach, does heartburn appear 15-30 minutes after drinking milk. The older the patient, the lower the amount of lactose triggers GERD symptoms [4,16,18].
The clinical presentation of GERD depends on many factors: age, duration of the disease, the extent of damage to the LES, the use of food triggers, the treatment, and the body's reactivity to tissue damage (allergies, histamine intolerance, etc.). Constant overdistension of the stomach in overweight individuals can also lead to failure of the LES and manifest itself in a typical GERD clinical picture. Below are observations explaining the pathogenesis of various clinical manifestations of GERD.
A 72-year-old female with GERD appeared intermittent heartburn in adolescence. At a young age, she began experiencing bronchospasm attacks, which were diagnosed as asthma, and the patient received bronchodilator therapy. At this time, GERD was diagnosed through X-ray. The bronchospasm attacks gradually passed. Due to abdominal pain and heartburn, she underwent repeated gastroscopies, which revealed a large hiatal hernia. Milk intolerance was discovered around age 60. Currently, severe heartburn occurs 15-30 minutes after drinking coffee with milk. When bending over, food with traces of food eaten the day before enters her mouth. Avoiding lactose-containing products, going to bed with an empty stomach, and taking 20 mg of Esomeprazole daily help her live a pain-free life. High-resolution manometry (HRM) has not led to changes in treatment (Figure 4).
.png)
Figure 4. (a) The X-ray was taken during barium swallow at maximum possible pressure in the stomach (raising straight legs). A sharp dilation of the esophagus is determined (2.6 cm instead of 1.7 cm), a sharp dilation of the esophageal ampulla (5 cm), which is unreasonably called a hernia. The LES, located caudal to the ampulla, did not close, despite the high pressure. (b) Five minutes later, in a resting state, reflux into the esophagus is determined. The LES has several folds, indicating a wide hiatus. Since the true height of D 10 (red line) is ≈ 2 cm, the length of the LES in the center of the folds is ≈ 1 cm. The ampulla is proximally closed by a contracted functional proximal sphincter (PS). The esophageal contraction at the level of the aortic arch is caused by contraction of the functional aorto-esophageal sphincter (AES), formed under the influence of hydrochloric acid at the site of anatomical narrowing of the esophagus. (c) HRM revealed a normal LES of 2.5 cm in length and did not detect a hiatal hernia.
The appearance of AES under the influence of hydrochloric acid leads to non-esophageal (pulmonary) symptoms of GERD [19], which explains the onset of bronchospasm in the patient at a young age. PS occurs only in GERD. Its contraction allows the contracting ampulla to create high pressure above the LES, causing the LES to open. This pressure must be higher than the pressure in the stomach to prevent reflux into the esophagus. Normally, this function is performed by the last peristaltic wave. However, in GERD, the force of peristalsis is reduced. Therefore, when the LES cannot withstand the tension during ampulla contraction and opens, the pressure in the ampulla drops, leading to reflux of gastric contents into the esophagus. This causes transient lower esophageal sphincter relaxations, which are characteristic only of GERD. The assertion that transient lower esophageal sphincter relaxations can occur in healthy individuals is because patients with GERD symptoms whose acid exposure time (AET) is < 4.0% are considered healthy [20]. This definition means that if a patient has AET < 4.0%, i.e., acid with a pH < 4 is in the esophagus for less than 1 hours during a 24-hour study, then this is a functional “esophageal disorder of gut–brain interaction” that requires specific treatment, not GERD [20].
It is obvious that in the dilated esophagus, against the background of inflammation, thickening of the walls occurs both in the esophagus itself and in the LES. The strength of the peristaltic wave decreases, which inevitably leads to a change in pressure compared to the norm. This observation allows us to compare two examination methods: radiography and HRM. (1) The radiographic method clearly proves the complete failure of the LES, which is confirmed by the appearance of eaten food in the mouth when bending after a meal. Its length (≈ 1 cm) and the large width of the hiatal opening, as well as free reflux in the horizontal position at rest, raise no doubt that this is a case of cardial chalasia. The HRM conclusion about the normal function of the LES based on the determination of its length as 2.5 cm contradicts the clinical symptoms and radiographic evidence. (2). Multiple gastroscopic examinations revealed a large hiatal hernia, the width of which on the radiograph with tight filling was equal to 5 cm. HRM did not detect the hernia. This observation indicates that HRM cannot serve as a diagnostic method, much less for scientific research.
GERD, based on visualization of the esophageal mucosa and histological examination, is divided into erosive reflux disease (E-GERD), if damage to the mucosa is visible during gastroscopy, and non-erosive reflux disease (NERD), if changes are not visible during gastroscopy, but histological examination reveals expansion of the intercellular space [21]. Dilated intercellular spaces correlated with loss or rearrangement of intercellular glycoconjugates of the overlying layers and with granulocyte (eosinophil and/or neutrophil) infiltration [21,22]. In E-GERD, focal destruction of the mucosa occurs under the influence of chemical elements of the gastric chyme (hydrochloric acid and pepsin). This occurs at sites of bolus retention—above the LES, above the PS, and above the AES—leading to prolonged local exposure to a chemically aggressive bolus. Healing of erosion, and especially a deep ulcer, can lead to fibrous tissue and esophageal stenosis. At the same time, irritation of the esophageal wall causes not limited, but an extended inflammatory reaction in the deeper layers of the esophagus (Figure 5).
.png)
Figure 5. (а-c) Stages of LES stenosis development in GERD. (a) Barium (acid) retention in the contracted ampulla above the LES. Inflammation in the LES mucosa is indicated by two thin parallel folds. (b) Rough deformed folds between the esophagus and stomach indicate more severe inflammation. (c) Sclerotic changes in the LES with slowed passage through it, as evidenced by the barium level in the esophagus. (d-f) Radiographs of the patients diagnosed with esophageal achalasia based on HRM. (d) In the projection of the LES, there is a narrowing with an uneven lumen 1.7 cm long, which prevents normal emptying of the esophagus, as evidenced by its significant dilation (3.8 cm). (e) Typical radiographic picture of peptic stenosis of the distal esophagus together with the proximal part of the LES. (f) Moderate esophageal dilation with a sharp shortening of the LES during its contraction (≈ 1 cm). A significant amount of contrast medium in the stomach and duodenum indicates good evacuation into the stomach.
Differential diagnosis between true esophageal chalasia (EA) and GERD with impaired evacuation from the esophagus (EA syndrome)
How did it happen that the diagnosis of the rare disease "esophageal achalasia," characterized by a normal-length LES that does not relax in response to high esophageal pressure, causing impaired esophageal emptying and symptom of dysphagia, manifested by a typical radiographic picture, turned into a common syndrome with obvious peptic narrowing? A disease with a common etiology, pathogenesis, anatomy, and physiology with a clinical picture of dysphagia due to spasm of the LES began to be equated with dysphagia syndrome due to mechanical narrowing of the LES based on HRM.
Esophageal achalasia (EA) was a very rare disorder characterized by the loss of nerve cells in the esophagus and LES, causing to LES contraction but not opening in response to increase of the esophageal pressure. However, over the past 50 years, the annual incidence of AE has increased more than 1000-fold. For example, in one district of Chicago, the incidence of EA increased from 0.03 to 32.58 per 100,000 populations [23] (Figure 6).
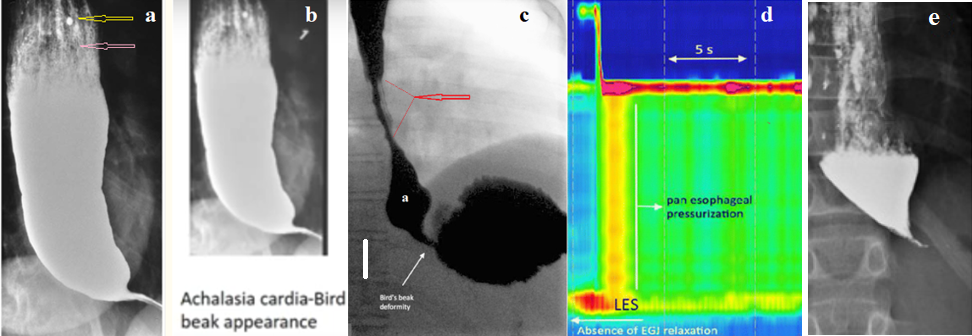
Figire 6. (a). Radiograph of a patient with EA from the article by Vaezi et al. [24]. (b). Radiograph from a textbook. Arrows indicate markers indicating that these are the same radiographs. (c-d). Study from the article by van der Pol et al. with the caption: - "A 14-year-old girl with dysphagia and vomiting. Based on radiological symptoms (dilated esophageal body, stasis of the contrast in it, a bird’s beak deformity in the EGJ) as well as on typical findings on HRM (absence EGJ relaxation), EA was diagnosed"[25]. The true height of D10 is ≈ 2 cm. (e) X-ray from article by Mashkov et al. [26].
Figure 6a is typical for EA. It is repeated three times in Vaezi's articles. The markers suggest that this particular figure is cited as an example in various review articles and textbooks. This supports the assertion that true EA is a very rare disease. Of the 29 cases of EA in children published in the public domain with radiographs, only one case (Figure 6e) had a radiographic appearance similar to true EA [26], which was supported by the authors' statement about the easy passage of the endoscope into the stomach [27].
All articles devoted to EA ignore the pathological physiology of the disease. Instead of describing the condition of the LES, authors refer to the mythical "bird beak," which is a LES and it when examined without provocation is observed only in GERD and EA. However, in EA, its length is always equal to the age-appropriate norm, while in GERD, its length is significantly shorter. In EA, there are no signs of inflammation, and the folds of the LES mucosa are thin and smooth. The LES opening in EA is mechanical and only occurs with a very dilated esophagus. In radiograph 6c, the narrow area between the ampulla (a) and the stomach, described as the "bird beak," is an open LES 1.7 cm long (with a minimum normal length of 3.2 cm) with an uneven lumen. The non-dilated esophagus and a significant amount of contrast medium in the stomach indicate the absence of obstruction in the EGJ. The radiograph clearly contradicts the HRM conclusion regarding "absence EGJ relaxation". The authors ignored the presence of a 3-cm peptic stenosis above the ampulla (red arrow), which was actually the cause of the pressure change in the esophagus. Thus, in a 14-year-old patient due to the use of HRM instead of GERD with peptic esophageal stenosis the EA was misdiagnosed. After repeated pneumodilations, the EGJ dysphagia completely resolved. As we have previously shown, dilation of the esophagus and sphincters of the esophagus, stomach, and duodenum by swallowing a dense tablet with a diameter of 1.9 to 2.3 cm improves sphincter function and has a beneficial effect on symptoms, but this does not eliminate the need for comprehensive treatment of GERD [18]. Comparison of X-ray examination with HRM shows the obvious diagnostic advantage of X-ray examination, its resolution is higher in all respects than the HRM.
In contrast to the rare condition known as esophageal achalasia, a syndrome of the same name has emerged. It differs from true achalasia in its etiology, pathogenesis, clinical symptoms, radiographic manifestations, and endoscopic findings. Its diagnosedmany times times more common than that of true achalasia. Patients previously diagnosed with GERD, based on complaints of dysphagia and unresponsive to therapy with proton pump inhibitors (PPIs), have been diagnosed with achalasia and treated as if they had true achalasia, i.e., by stretching or transecting the LES along with the esophageal sections above it and the proximal portion of the stomach below the LES. Was this change scientifically justified?
INFERENCES
1. Authors describing the current state of the problem do not utilize known scientific achievements in physiology. It seems as if manometric indicators were developed by engineers who searched for manometric patterns based on the analysis of patients with clinician diagnoses. For example, instead of the physiological explanation of the function of the EGJ described above, their analysis "is based on Poiseuille's Law of Flow, which states that the flow rate of a liquid through a tube is directly proportional to the fourth power of the radius of the tube and inversely related to the length and viscosity of the tube" [28]. Pressure characteristics (Diagnostic Thresholds and Definitions) do not have physiological meaning, such as: integrated relaxation pressure (IRP), distal contractile integral (DCI), contractile deceleration point (CDP), distal latency (DL) [29].
2. All these parameters have no diagnostic value, since the normal ranges were not determined on healthy people. “Healthy, asymptomatic adult volunteers were enrolled. Subjects were paid for their participation” [30]. Such selection of control individuals to determine normal ranges was and is still used for all instrumental research methods, including pH monitoring and HRM. However, science should not rely on subjective assessments in general, and especially not on patients’ opinions. In addition, the reliability of new methods should be verified using other methods. Lee et al., as a result of an endoscopic examination of 6,683 health examinees, detected esophageal diseases in 17.26% of cases. Gastroesophageal reflux diseases (GERD) were the most common diseases (15%) [31]. Since gastroscopy reveals only complications of the disease (erosions, narrowing, Barrett’s esophagitis, and tumors), the true incidence of GERD is significantly higher than 15%. Because hydrochloric acid destroys nerve elements, pain sensitivity is lost. For example, Shieh et al. showed that of patients with achalasia of the esophagus after POEM surgery, 26 (41.9%) had erosive esophagitis, but only 12 had GERD symptoms [32]. Receiving payment for participating in an experiment provides an incentive to answer questions in bad faith. This conflict of interest is another methodological fallacy.
Due to a violation of scientific methodology, approximately 50% of the control subjects were found to have GERD. Therefore, a reasonable question arises: why did the authors neglect scientific methodology? It also seems strange that, while promoting pH monitoring as a reliable method for diagnosing GERD, the authors did not use it to exclude GERD patients from the control subjects to determine normal values for HRM. This analysis demonstrates the low scientific qualifications of the authors promoting HRM and confirms the low diagnostic accuracy of this method.
3. Currently, HRM is used in patients with dysphagia who do not respond to therapy with proton pump inhibitors (PPIs). However, this category of patients also includes those with GERD. In review by Lanzoni et al shows that pediatric dysphagia was caused by a heterogeneous group of disorders, among which in addition to EA are the most relevant EoE and GERD [33]. The failure to respond to the therapy with PPIs occurs in a significant number of patients with GERD, which leads them to surgical treatment [24].
4. Numerous articles on HRM emphasize that "high-resolution manometry (HRM) is the primary method to evaluate esophageal motility and sphincter function" [34]. “Currently high-resolution manometry in combination with the Chicago Classification v3.0 is the “Gold Standard” for the "clinical" assessment of esophageal motility disorders” [28]. On the one hand, proponents of HRM claim that HRM determines only the manometric profile of the esophagus. Однако, the division of ЕА into 3 subtypes, от чего зависит лечение больных turns the HRM into a diagnosis method.
5. It is known that a chronic inflammatory process in the esophagus caused by damage to the wall by hydrochloric acid leads to the formation of an inflammatory infiltrate, which can be complicated by motility disturbances, fibrogenesis, and carcinogenesis [35]. The inflammatory process, complicated by erosion, ulceration, and scar tissue formation, causes narrowing of the esophagus and/or LES, which impairs bolus evacuation into the stomach and is accompanied by esophageal dilation and pressure changes. HRM is not only unable to differentiate true EA from peptic esophageal stenosis in GERD, but, as shown above (all figures, including figures 4 and 6 with HRM), it incorrectly localizes the evacuation disorder. As shown in a study by Kwiatek et al in patients with achalasia frequently had a LES relaxation as well as in patients without achalasia [36]. This means that the authors are not describing true achalasia, which is characterized by a lack of relaxation.
6. A reasonable question arises: why did patients with typical GERD symptoms, в том числе у тех где a diagnosis confirmed by pH monitoring and erosive esophagitis, develop stenosis? Obviously, the patients either did not receive treatment or the treatment was ineffective. Analysis of the literature indicates that treatment for GERD includes only suppression of gastric acidity and only in those patients with AES > 6% [18]. Even this treatment is not received by patients who based on pH monitoring, instead of GERD, are erroneously diagnosed with "functional heartburn", "functional dyspepsia", "esophageal hypersensitivity", "irritable bowel syndrome", etc. They instead of treating GERD receive antidepressants [37]. Only comprehensive treatment for GERD can lead to cure if diagnosed early, and if diagnosed late to control symptoms.Complex treatment includes: suppression of hydrochloric acid production (PPI), exclusion from food of provocateurs that increase the secretion of hydrochloric acid (lactose, etc.), use of acid-neutralizing medications, gastrointestinal mucosal protectors (bismuth salts, Esoxx), reflux prevention through diet and behavior (such as lying down only on an empty stomach), and dilation of the esophagus and sphincters by swallowing dense tablets 1.9-2.3 cm in diameter [18]. The Chicago Classification, blurring the boundaries of GERD and classical EA, created a fictitious disease “EA syndrome”, which supposedly had all the signs of classical EA, but was not related to GERD. The goal of the per-oral endoscopic myotomy (POEM) or Heller myotomy operation is the vertical intersection of the circular muscle layer of the LES. However, the LES has no visible anatomical boundaries, therefore, in adults in whom the length of the LES is ≈ 4 cm, dissection is usually performed to the total length 8.3 ± 1.8 (6–15). In children median age 14 years, range 9 to 18 years the median length of total myotomy was 12 cm (range, 6–16 cm) [26]. This means that in addition to cutting the circular muscle fibers of the LES, surgeons cut the muscle fibers of the esophagus and stomach above and below the LES. Although LES function is weakened in GERD, its dissection during POEM completely and permanently eliminates its antireflux function.
7. Complications after dissection of the LES. Dissection of the ring of the muscular wall of the LES inevitably and irrevocably stops its antireflux function. The percentage of GERD after EA surgery in different articles ranges from 41% to 69.8%. It can be assumed that this figure is underestimated, since severe complications can occur without pronounced symptoms [26]. Ota et al detected esophageal cancer in 6 patients. All 6 patients undergone surgery for achalasia and the outcome had been rated as excellent or good [38]. Questionnaire results by Meyer et al., suggested a significant long term deleterious impact of Heller myotomy on the quality of life of children and their families [39]. Thus, long-term results after dissection of the LES in patients with GERD with EA syndrome fully confirm the theoretical conclusion about the development of more severe GERD in most patients.
Complications after dissection of the esophageal wall
According to Triggs et al., blown-out myotomy (BOM) is a postoperative complication for achalasia in 17.8% of patients after POEM [40]. The diverticular-like changes occur because of dissections of the muscular layer of the esophagus above the LES. The severity of the complication is because refluxant with low pH and pepsin may reside within these pockets, causing inflammation and ulceration. This figure (18%) does not reflect the true incidence of this complication. Firstly, because they included patients who had a post-treatment esophagram within 1 year of their follow-up manometry. Meanwhile, mucosal protrusion into the muscular window may increase over time. Secondly, the authors arbitrarily classified only those cases where the width-mouthed outpouching was >50% increase in esophageal diameter in the myotomy as BOM.
Thus, BOM is a serious complication of myotomy, which has begun to be identified recently. This is another circumstance that should make the surgeon think about the need for myotomy in EA syndrome.
CONCLUSION
Over the years, at four physician meetings (Chicago Classification), specially invited physicians agreed manometric diagnosis of diseases through Delphi voting. Their proposals are widely published, despite declarations of conflicts of interest. They claim to receive grants, to be full-time lecturers, consultants for numerous companies, etc. [29]. These statements cannot but raise suspicions about the integrity of decisions during voting. All new methods are tested by methods that were previously considered the gold standard. But HRM has not been tested by other methods. Radiographic examination using maximum provocation, unlike HRM, allows for the accurate diagnosis of GERD. Using this method, it was demonstrated that the increase in frequency of EA is due to misdiagnosis, because of which patients with GERD were diagnosed with EA and treated as if they had true EA. This led to serious complications that were not observed before the introduction of HRM. From these considerations, it follows that HRM cannot serve as a diagnostic method at all, much less to be used for scientific research [41].
REFERENCES
- Alvarez WC. (1924). Bayliss and Starling’s Law of to be be bee Intestine or the Myenteric Reflex. American Journal of Physiology–Legacy Content. 69(2).
- Levin MD. (2024). Gastrointestinal motility and law of the intestine. Gastroenterology & Hepatology: Open access. 15(5):163-172.
- Lang IM, Shaker R. (1997). Anatomy and physiology of the upper esophageal sphincter. Am J Med. 103(5A):50S-55S.
- Levin MD. (2025). X-Ray Imaging of the Esophagus and Lower Esophageal Sphincter and Its Role in the Diagnosis of Gastroesophageal Reflux Disease. Mathews J Gastroenterol Hepatol. 10(2):31.
- Bott TS, von Kalle T, Schilling A, Diez OH, Besch S, Mehlig U, et al. (2019). Esophageal Diameters in Children Correlated to Body Weight. Eur J Pediatr Surg. 29(6):528-532.
- Shafik A, El-Sibai O, Shafik AA, Mostafa R, Shafik I. (2004). Effect of straining on the lower esophageal sphincter: identification of the "straining-esophageal reflex" and its role in gastroesophageal competence mechanism. J Invest Surg. 17(4):191-196.
- Yassi R, Cheng LK, Rajagopal V, Nash MP, Windsor JA, Pullan AJ. (2009). Modeling of the Mechanical Function of the Human Gastroesophageal Junction Using an Anatomically-Realistic Three-Dimensional Model. J Biomech. 42(11):1604-1609.
- Shafik A, Shafik AA, El Sibai O, Shafik IA. (2007). The effect of gastric overfilling on the pharyngo-esophageal and lower esophageal sphincter: a possible factor in restricting food intake. Med Sci Monit. 13(10):BR220-BR224.
- Chandrasoma P, DeMeester T. (2016). A New Pathologic Assessment of Gastroesophageal Reflux Disease: The Squamo-Oxyntic Gap. Adv Exp Med Biol. 908:41-78.
- Valdovinos Díaz MA, Flores C, Facha MT, Koller Lucio J. (1999). Esophageal manometry in gastroesophageal reflux disease. Lower esophageal sphincter incompetence or esophageal dismotility? Rev Gastroenterol Mex. 64(1):16-18.
- Ritter MP, Peters JH, DeMeester TR, Crookes PF, Mason RJ, Green L, et al. (1998). Outcome after laparoscopic fundoplication is not dependent on a structurally defective lower esophageal sphincter. J Gastrointest Surg. 2(6):567-572.
- Kwiatek MA, Nicodème F, Pandolfino JE, Kahrilas PJ. (2012). Pressure morphology of the relaxed lower esophageal sphincter: the formation and collapse of the phrenic ampulla. Am J Physiol Gastrointest Liver Physiol. 302(3):G389-G396.
- Kirchhoff P, Socrates T, Sidani S, Duffy A, Breidthardt T, Grob C, et al. (2011). Zinc salts provide a novel, prolonged and rapid inhibition of gastric acid secretion. Am J Gastroenterol. 106(1):62-70.
- Levin MD. (2023). Gastrointestinal Motility and Law of the Intestine. (Preprint). DOI:10.20944/preprints202312.2003.v1.
- Levin MD. (2025). Hydrochloric acid hypersecretion is the cause of pathology of the upper digestive tract. Literature analysis. DOI: 10.32388/4QXH2Q.
- Levin MD. (2025). Pathogenesis of Infantile Colic. Hypothesis. Mathews JGastroenterol Hepatol. 10(1):29.
- Byers KG, Savaiano DA. (2005). The myth of increased lactose intolerance in African-Americans. J Am Coll Nutr. 24(6 Suppl):569S-573S.
- Levin MD. (2025). Prevention and Treatment of Esophageal Reflux Disease: Literature Analysis. Mathews J Gastroenterol Hepatol. 10(2):33.
- Levin MD. (2025). Aorto-Esophageal Sphincter and its role in the pathogenesis of the gastroesophageal reflux: cases report and analysis. Gastroenterol Hepatol Open Access. 16(1):1-8.
- Gyawali CP, Yadlapati R, Fass R, Katzka D, Pandolfino J, Savarino E, et al. (2024). Updates to the modern diagnosis of GERD: Lyon consensus 2.0. Gut. 73(2):361-371.
- Solcia E, Villani L, Luinetti O, Trespi E, Strada E, Tinelli C, et al. (2000). Altered intercellular glycoconjugates and dilated intercellular spaces of esophageal epithelium in reflux disease. Virchows Arch. 436(3):207-216.
- Brzacki V, Nagorni A, Mihailović D, Raicević-Sibinović S, Mladenović B. (2010). Analysis of the grade of esophagitis, chromendoscopical and histological findings of esophagus in patients with gastroesophageal reflux disease before and after the therapy. Vojnosanit Pregl. 67(12):991-997.
- Samo S, Carlson DA, Gregory DL, Gawel SH, Pandolfino JE, Kahrilas PJ. (2017). Incidence and Prevalence of Achalasia in Central Chicago, 2004-2014, Since the Widespread Use of High-Resolution Manometry. Clin Gastroenterol Hepatol. 15(3):366-373.
- Vaezi MF, Pandolfino JE, Yadlapati RH, Greer KB, Kavitt RT. (2020). ACG Clinical Guidelines: Diagnosis and Management of Achalasia. Am J Gastroenterol. 115(9):1393-1411.
- van der Pol RJ, Benninga MA, Magré J, Van Maldergem L, Rotteveel J, van der Knaap MS, et al. (2015). Berardinelli-Seip syndrome and achalasia: a shared pathomechanism? Eur J Pediatr. 174(7):975-980.
- Levin MD. (2024). Esophageal achalasia or gastroesophageal reflux? Pediatric cases analysis. Gastroenterol Hepatol Open Access. 15(6):174-184.
- Mashkov AE, Pykchteev DA, Sigachev AV, Bobylev AV, Mayr JM. (2018). Obstructive bronchitis and recurrent pneumonia in esophageal achalasia in a child: A CARE compliant case report. Medicine (Baltimore). 97(23):e11016.
- Donnan EN, Pandolfino JE. (2020). EndoFLIP in the Esophagus: Assessing Sphincter Function, Wall Stiffness, and Motility to Guide Treatment. Gastroenterol Clin North Am. 49(3):427-435.
- Yadlapati R, Kahrilas PJ, Fox MR, Bredenoord AJ, Prakash Gyawali C, Roman S, et al. (2021). Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0©. Neurogastroenterol Motil. 33(1):e14058.
- Carlson DA, Kou W, Lin Z, Hinchcliff M, Thakrar A, Falmagne S, et al. (2019). Normal Values of Esophageal Distensibility and Distension-Induced Contractility Measured by Functional Luminal Imaging Probe Panometry. Clin Gastroenterol Hepatol. 17(4):674-681.e1.
- Lee JH, Kim N, Chung IK, Jo YJ, Seo GS, Kim SW, et al. (2008). Clinical significance of minimal change lesions of the esophagus in a healthy Korean population: a nationwide multi-center prospective study. J Gastroenterol Hepatol. 23(7 Pt 1):1153-1157.
- Shieh TY, Chen CC, Chou CK, Hu TY, Wu JF, Chen MJ, et al. (2022). Clinical efficacy and safety of peroral endoscopic myotomy for esophageal achalasia: A multicenter study in Taiwan. J Formos Med Assoc. 121(6):1123-1132.
- Lanzoni G, Sembenini C, Gastaldo S, Leonardi L, Bentivoglio VP, Faggian G, et al. (2022). Esophageal Dysphagia in Children: State of the Art and Proposal for a Symptom-Based Diagnostic Approach. Front Pediatr. 10:885308.
- Singendonk MJ, Lin Z, Scheerens C, Tack J, Carlson DA, Omari TI, et al. (2019). High-resolution impedance manometry parameters in the evaluation of esophageal function of non-obstructive dysphagia patients. Neurogastroenterol Motil. 31(2):e13505.
- Rieder F, Biancani P, Harnett K, Yerian L, Falk GW. (2010). Inflammatory mediators in gastroesophageal reflux disease: impact on esophageal motility, fibrosis, and carcinogenesis. Am J Physiol Gastrointest Liver Physiol. 298(5):G571-G581.
- Kwiatek MA, Post J, Pandolfino JE, Kahrilas PJ. (2009). Transient lower oesophageal sphincter relaxation in achalasia: everything but LOS relaxation. Neurogastroenterol Motil. 21(12):1294-e123.
- Weijenborg PW, de Schepper HS, Smout AJ, Bredenoord AJ. (2015). Effects of antidepressants in patients with functional esophageal disorders or gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 13(2):251-259.e1.
- Ota M, Narumiya K, Kudo K, Yagawa Y, Maeda S, Osugi H, et al. (2016). Incidence of Esophageal Carcinomas After Surgery for Achalasia: Usefulness of Long-Term and Periodic Follow-up. Am J Case Rep. 17:845-849.
- Meyer A, Catto-Smith A, Crameri J, Simpson D, Alex G, Hardikar W, et al. (2017). Achalasia: Outcome in children. J Gastroenterol Hepatol. 32(2):395-400.
- Triggs JR, Krause AJ, Carlson DA, Donnan EN, Campagna RAJ, Jain AS, et al. (2021). Blown-out myotomy: an adverse event of laparoscopic Heller myotomy and peroral endoscopic myotomy for achalasia. Gastrointest Endosc. 93(4):861-868.e1.
- Woodland P, Sifrim D. (2013). Management of gastro-oesophageal reflux disease symptoms that do not respond to proton pump inhibitors. Curr Opin Gastroenterol. 29(4):431-436.