Information Links
Related Conferences
Current Issue Volume 10, Issue 3 - 2025
The First Documented Case of Joubert Syndrome in Iraq: A Novel Variant
Aamir Jalal Al-Mosawi*
Advisor Doctor and Expert Trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq
*Corresponding Author: Aamir Jalal Al-Mosawi, Advisor doctor and expert trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq, Email: [email protected]
Received Date: November 10, 2025
Published Date: November 26, 2025
Citation: Al-Mosawi AJ. (2025). The First Documented Case of Joubert Syndrome in Iraq: A Novel Variant. Mathews J Pediatr. 10(3):47.
Copyrights: Al-Mosawi AJ. © (2025).
ABSTRACT
Background: Joubert Syndrome is a rare autosomal recessive neurological disorder marked by hypotonia, developmental delay, and a distinctive brain malformation called the "molar tooth sign", visible on MRI and caused by cerebellar vermis hypoplasia/agenesis. It was first described in 1969 by Marie Joubert and later elaborated on by other researchers. Patients and methods: A 3-year-old female with significant developmental delays, generalized hypotonia, and eye movement abnormalities was evaluated. Her parents were consanguineous, and no family history of similar conditions was reported. MRI showed the classic molar tooth sign, confirming a diagnosis within the Joubert Syndrome spectrum. Clinical Findings:
- Facial features: Synophrys, thick lips, epicanthal folds, frontal hair upsweep, strabismus, hypertelorism, and hypotonic facial expression.
- Neurological: Severe global developmental delay, hypotonia, and nystagmus.
- No abnormalities in limbs, digits, or major organs (kidney, liver).
- No polydactyly or oral anomalies, differentiating it from JS-OFD subtype.
Results: The findings suggested a diagnosis of Joubert Syndrome with oculofacial features (JS-OFG), but without organ or digital involvement, indicating a potentially novel or unclassified variant.
The patient was treated based on our extensive published experiences with treatment of neurological disorders and mental retardation:
- Cerebrolysin, piracetam, citicoline, and nandrolone decanoate.
- Showed improvements in muscle tone, ability to sit and crawl, and reduction in squint and nystagmus.
Conclusion: This case, the first documented case of the syndrome in Iraq illustrates the variability in Joubert syndrome presentation and highlights a potentially new subtype with prominent oculofacial dysmorphism but without systemic or digital anomalies.
Keywords: Joubert Syndrome, New Subtype, Treatment.
INTRODUCTION
Joubert syndrome is a very rare heterogeneous group of autosomal recessive mental retardation syndromes characterized by hypotonia and hypoplasia/agenesis of the cerebellar vermis which has characteristic tooth-like appearance on brain imaging, which is called the “Molar tooth sign”.
The syndrome was first described by Marie Joubert, a pediatric neurologist and her colleagues in 1969. They described a family of four siblings in a French Canadian family, with distantly related parents.
1977, Boltshauser and Isler highlighted the unique mental retardation syndrome associated with agenesis of the cerebellar vermis described by Joubert et al. (1969). They described three other children including two brothers, and called the condition “Joubert syndrome” [1,2].
Friede and Boltshauser from Switzerland reported that postmortem examination of a case of Joubert syndrome revealed an almost total aplasia of the cerebellar vermis [3].
In 1980, Paolo Curatolo from Italy and his colleagues reviewed nine reported cases and described a new case of Joubert syndrome. The diagnosis agenesis of the cerebellar vermis was confirmed by computerized tomography [4].
During the same year, Aparicio Meix and Pascual Castroviejo reported a male patient with Joubert. Computerized tomography showed an occipital encephalocele and partial defects of the cerebellar vermis. They emphasized that the episodic hyperpnea, facial hemispasms, and abnormal eye movements which are seen during infancy disappear at the age of three years, and mental retardation is the main presentation [5].
The 12th case of Joubert syndrome was reported by Lindhout and colleagues in 1980. Computerized axial tomography of the brain showed aplasia of the cerebellar vermis. This case was associated with bilateral colobomata of retina and choroid [6].
This paper presents the first documented case of Joubert syndrome in Iraq which was associated with notable oculofacial dysmorphism.
PATIENTS AND METHODS
At about the age of three years, a female child was evaluated for significant developmental delay, muscle hypotonia and nystagmus. The parents are related and family history was negative for similar condition. On examination, she was not sating any word and had poor spontaneous movements, and unable to sit alone. She had no limb abnormalities or polydactyly. Notable craniofacial dysmorphisms included (Figure 1):
- Thick eyebrows with synophrys (midline unibrow)
- Long eyelashes
- Broad/high forehead
- Coarse, curly hair with a frontal upsweep
- Low-set ears
- Full cheeks
- Thick, especially upper, lips
- Everted lower lip
- Short philtrum
- Downturned mouth corners
- Open mouth posture
- Facial hypotonia and reduced facial expression
- Epicanthal folds and apparent hypertelorism
- Strabismus (squint)
Neurologic examination confirmed generalized hypotonia and severe global developmental delay. There were no abnormalities of the digits, limbs, or skeletal system.
MRI of the brain revealed MRI revealed “elongated cerebellar peduncles and abnormal 4th ventricle with a tooth-like appearance “Molar tooth sign”, suggesting vermian agenesis/hypoplasia.
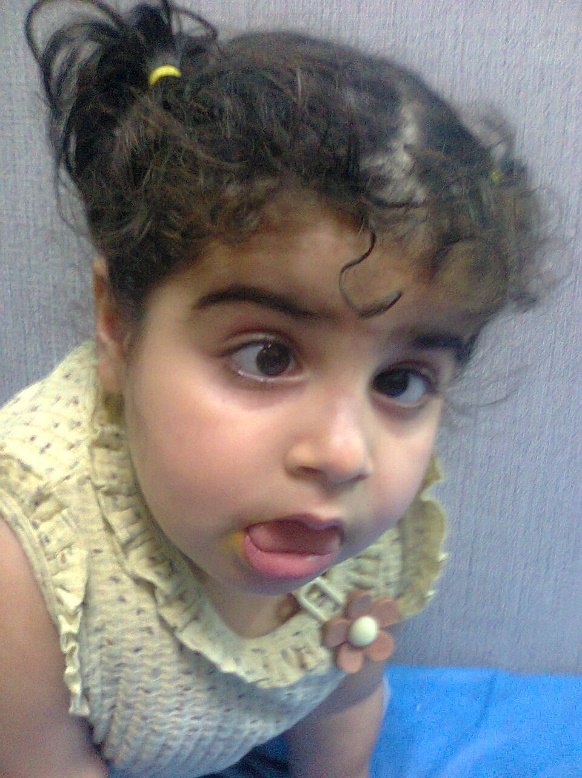
Figure 1. The first documented case of Joubert syndrome in Iraq was a girl who exhibited notable craniofacial dysmorphisms.
- Molar tooth sign on MRI confirms a diagnosis within the Joubert syndrome spectrum disorders.
- Facial dysmorphism with features like synophrys, epicanthal folds, thick lips, and frontal upsweep suggests a recognizable facial gestalt.
- Ocular findings: Squint and apparent hypertelorism.
- No polydactyly or digital anomalies, which are typical of some JS subtypes like JS-OFD or JS with Jeune asphyxiating thoracic dystrophy.
- Cognitive delay and hypotonia support central nervous system involvement.
The patient was treated based on our extensive published experiences with the treatment of neurologic disorders and mental retardation [7-17].
First week treatment included:
Daily intramuscular cerebrolysin
Single intramuscular injection of nandrolone decanoate 12.5 mg.
Oral piracetam 400 mg daily in the morning.
Thereafter, she was treated for one month with:
Intramuscular piracetam (400mg) every third day (10 doses) over one month.
Oral citicoline 200 mg daily in the morning.
Treatment was associate with obvious improvement in muscle tone and she was able to sit and crawl. Treatment was also associated with reduction in squint and nystagmus.
DISCUSSION
Joubert syndrome and related disorders are genetically and phenotypically heterogeneous ciliopathies characterized by the molar tooth sign. Various subtypes have been defined, including those with ocular (retinal dystrophy), hepatic, renal, or limb anomalies. This case does not fit neatly into the known subtypes, as the patient lacks renal, hepatic, or digital abnormalities.
The distinctive oculofacial dysmorphism in this case may represent a unique JS variant. There was no evidence of oral-facial-digital syndrome type VI (JS-OFD), as there was no oral or limb anomalies. The constellation of features aligns with the Joubert syndrome with oculofacial features (JS-OFG) pattern but appears to define a previously unreported combination [18-23].
We ruled out other syndromes with overlapping facial features, such as Cornelia de Lange and Smith-Lemli-Opitz, based on absence of associated systemic findings.
For many decades, the fields of clinical genetics and dysmorphology were largely absent from the Iraqi medical landscape.
There were no structured diagnostic pathways, no specialized centers for rare diseases, and minimal local literature to support genetic awareness or dysmorphic diagnosis. As a result, generations of patients with congenital abnormalities and inherited disorders remained undiagnosed or misclassified.
The transformation began with our early clinical observations in pediatric practice, which led to the recognition of patterns suggestive of specific syndromes. Gradually, through careful phenotyping, clinical photography, and correlating systemic findings with existing global data, we began to document and publish rare and very rare disorders observed among Iraqi children.
Common genetic and hereditary disorders in Iraq include the thalassaemias and hemophilias, for these disorders specialized clinics and centers have been established. In addition to Down syndrome which has been observed frequently, many other less common disorders have also been reported including polycystic kidney disease, achondroplasia, Duchenne muscular dystrophy, Werding Hoffman disease, Gaucher disease, mucopolysaccharidosis.
We have previously reported an uncountable number of the first described disorders in Iraq [24-28].
In this paper, we describe the first documented case of Joubert syndrome in Iraq which represents a novel dysmorphic oculofacial subtype of Joubert syndrome without limb involvement.
CONCLUSION
This case, the first documented case likely represents a unique, dysmorphic oculofacial form of Joubert syndrome (JS-OFG) without limb involvement. It suggests a novel subtype of Joubert syndrome, specifically with predominant oculofacial features and hypotonia, but notably without digital (limb) anomalies, potentially expanding the phenotype of Joubert syndrome with oculofacial features (JS-OFG).
ACKNOWLEDGEMENT
The author would to express his gratitude for the parents of the patient who accepted publishing her photo.
CONFLICT OF INTEREST
None.
REFERENCES
- Joubert M, Eisenring JJ, Robb JP, Andermann F. (1969). Familial agenesis of the cerebellar vermis. A syndrome of episodic hyperpnea, abnormal eye movements, ataxia, and retardation. Neurology. 19(9):813-825.
- Boltshauser E, Isler W. (1977). Joubert syndrome: episodic hyperpnea, abnormal eye movements, retardation and ataxia, associated with dysplasia of the cerebellar vermis. Neuropadiatrie. 8(1):57-66.
- Friede RL, Boltshauser E. (1978). Uncommon syndromes of cerebellar vermis aplasia. I: Joubert syndrome. Dev Med Child Neurol. 20(6):758-763.
- Curatolo P, Mercuri S, Cotroneo E. (1980). Joubert syndrome: a case confirmed by computerized tomography. Dev Med Child Neurol. 22(3):362-366.
- Aparicio Meix JM, Pascual Castroviejo I. (1980). Síndrome de Joubert. Estudio de un nuevo caso y revisión de la literatura [Joubert syndrome. Report of a new case and review of literature]. An Esp Pediatr. 13(7):625-632.
- Lindhout D, Barth PG, Valk J, Boen-Tan TN. (1980). The Joubert syndrome associated with bilateral chorioretinal coloboma. Eur J Pediatr. 134(2):173-176.
- Al-Mosawi AJ. (2019). New therapies for the treatment of spastic cerebral palsy. Medical Journal of Clinical Trials & Case Studies (ISSN: 2578-4838). 3(2):1-9.
- Al-Mosawi AJ. (2019). New therapies for Rett syndrome. Journal of Bio Innovation (e-ISSN 2277-8330). 8(3):301-307.
- Al-Mosawi AJ. (2019). The pattern of cerebral palsy in Iraqi children. MedLife Clinics (ISSN: 2689-5943). 1(1):1-9.
- Al-Mosawi AJ. (2020). New Therapies for the treatment of ataxic cerebral palsy caused by kernicterus. EC Clinical and Medical Case Reports. 3(4):26-31.
- Al-Mosawi AJ. (2020). The experience with the use of nandrolone decanoate and pyritinol in children with cerebral palsy. Open Access Journal of Biogeneric Science and Research (ISSN: 2692-1081). 2(3):1-3.
- Al-Mosawi AJ. (2020). Cerebral palsy: A unique illustrated experience. Medico Research Chronicles (ISSN: 2394-3971). 7(4):2017-2239.
- Al-Mosawi AJ. (2021). The early treatment of a boy from Virginia with ataxic cerebral palsy. Journal of Pediatrics and Child Health. 2(4):1-5.
- Al-Mosawi AJ. (2019). The etiology of mental retardation in Iraqi children. SunKrist Journal of Neonatology and Pediatrics. 1(1):1-9.
- Al-Mosawi AJ. (2020). A Unique experience with mental and developmental retardation: Innovative Medical therapies for idiopathic mental retardation. EC Clinical and Medical Case Reports. 3(5):42-54.
- Al-Mosawi AJ. (2020). Recent uses of piracetam in pediatric neurology. SunKrist Neurology, Neurosurgery and Stroke Journal. 2(1):2020.
- Al-Mosawi AJ. (2020). Treatment of a boy with idiopathic mental retardation: From uneducable to educable. Progressing Aspects in Pediatrics and Neonatology (ISSN: 2637-4722). 2(5):1-6.
- Romani M, Mancini F, Micalizzi A, Poretti A, Miccinilli E, Accorsi P, et al. (2015). Oral-facial-digital syndrome type VI: is C5orf42 really the major gene? Hum Genet. 134(1):123-126.
- Erol S, Demirel N, Bas AY, Ozcan B, Celik IH, Isik DU. (2016). An unusual presentation of Joubert syndrome and related disorders in a newborn: Panhypopituitarism. Genet Couns. 27(3):367-371.
- Johnston JJ, Lee C, Wentzensen IM, Parisi MA, Crenshaw MM, Sapp JC, et al. (2017). Compound heterozygous alterations in intraflagellar transport protein CLUAP1 in a child with a novel Joubert and oral-facial-digital overlap syndrome. Cold Spring Harb Mol Case Stud. 3(4):a001321.
- De Mori R, Romani M, D'Arrigo S, Zaki MS, Lorefice E, Tardivo S, et al. (2017). Hypomorphic Recessive Variants in SUFU Impair the Sonic Hedgehog Pathway and Cause Joubert Syndrome with Cranio-facial and Skeletal Defects. Am J Hum Genet. 101(4):552-563.
- Niceta M, Dentici ML, Ciolfi A, Marini R, Barresi S, Lepri FR, et al. (2020). Co-occurrence of mutations in KIF7 and KIAA0556 in Joubert syndrome with ocular coloboma, pituitary malformation and growth hormone deficiency: a case report and literature review. BMC Pediatr. 20(1):120.
- Surisetti BK, Holla VV, Prasad S, Neeraja K, Kamble N, Yadav R, et al. (2021). Clinical and Imaging Profile of Patients with Joubert Syndrome. J Mov Disord. 14(3):231-235.
- Al-Mosawi AJ. (2011). Rare genetic disorders in Iraq. 1st ed., Saarbrücken; LAP Lambert Academic Publishing. ISBN: 978-3-8473-1702-9.
- Al-Mosawi AJ. (2018). The Uncommon and Rare Genetic Disorders in Iraq. 1st ed., Saarbrücken; LAP Lambert Academic Publishing. ISBN: 13:978-613-9-47346-5.
- Al-Mosawi AJ. (2019). Genetic and Hereditary Disorders in Iraqi Children. Ann Med & Surg Case Rep. 1(2):1-8.
- Al-Mosawi AJ. (2020). Clinical Genetics and Dysmorphology: Our Extraordinary Experiences. SunKrist Journal of Neonatology and Pediatrics. 2(1):1-10.
- Al-Mosawi AJ. (2025). New Clinical Disorders, Including Genetic and Dysmorphic Syndromes. LAP LAMBERT Academic Publishing. ISBN: 978-620-8-06396-2.