Information Links
Related Conferences
Previous Issues Volume 8, Issue 4 - 2023
The Application of Point-of-Care Ultrasound in ED Intubations and Airway Access: A Brief Systematic Review
Frank Wheeler1, James Espinosa1,*, Alan Lucerna2
1Department of Emergency Medicine, Jefferson Health NJ, Stratford, NJ, USA
2Program Director, Emergency Medicine, Jefferson NJ/Rowan University SOM, USA
*Corresponding Author: James Espinosa, Department of Emergency Medicine, Jefferson Health NJ, 18 East Laurel Road, Stratford, NJ 08084, USA. Email: [email protected]
Received Date: June 16, 2023
Publication Date: July 10, 2023
Citation: Wheeler F, Espinosa J, Lucerna A. (2023). The Application of Point-of-Care Ultrasound in ED Intubations and Airway Access: A Brief Systematic Review. Mathews J Emergency Med. 8(4):57.
Copyright: Wheeler F, et al. © (2023)
ABSTRACT
Intubation is an essential procedure performed on a routine basis in the Emergency Department. Unsuccessful intubations can be associated with deleterious outcomes. A systematic review was performed to investigate the accuracy of Point of Care Ultrasound (POCUS) in successful Endotracheal Tube (ET) tube confirmation, dynamically in ultrasound guided intubation and in identification of the cricothyroid membrane. This review demonstrated high sensitivity and specificity for ultrasound confirmation of ET tube placement, high success rate in ultrasound-guided intubation, and lower than expected accuracy in identifying the cricothyroid membrane. Ultrasonography should be considered for ET tube confirmation in patients in cardiac arrest and future applications of ultrasound may include dynamic guiding during the process of intubation.
Keywords: Airway access, Endotracheal tube confirmation with ultrasound, ultrasound guided intubation
INTRODUCTION
Securing an airway is a critical procedure completed performed routinely in the Emergency Department (ED). Failing to obtain an airway carries the risk of adverse consequences which can result in significant morbidity and death. Traditional methods of confirming endotracheal tube placement include auscultation for bilateral breath sounds as well as ascertaining for tube condensation. However, these findings have been found to be unreliable Kelly, et al. [1]. Many consider end-tidal waveform capnography to be the gold standard to confirm ET tube placement. However, in a patient in cardiac arrest, the sensitivity of this method decreases significantly [2].
Cricothyroidotomy is not routinely performed in the ED, but can be critical to establishing an airway with the failure of endotracheal intubation. Success of a cricothyrotomy is dependent on accurate identification of the cricothyroid membrane. Identifying the cricothyroid membrane by inspection and palpation is significantly low, especially in patients that are obese [3,4].
This review will investigate the accuracy of point of care ultrasound (POCUS) in successful endotracheal tube (ET) tube confirmation, dynamically in ultrasound guided intubation and in identification of the cricothyroid membrane.
METHODS
This review was structured in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines for systematic reviews (P.R.I.S.M.A) guidelines [5].
A search was conducted of PubMed from inception to March 8, 2021. Bibliographies of selected studies were reviewed to ascertain for further relevant articles of interest. Inclusion criteria consisted of all case-studies, prospective trials, randomized controlled trials and meta-analysis assessing ultrasound applications during intubation, confirmation of tube placement following intubation as well as identification of cricothyroid membrane. Keywords utilized consisted of Cricothyroidotomy, Ultrasound, Tracheal intubation, Airway access, Endotracheal tube confirmation. All included studies must have provided data regarding success or failure of ultrasound applications discussed above. Any not pertinent to the subject matter were excluded as well as duplicates (Figure 1).
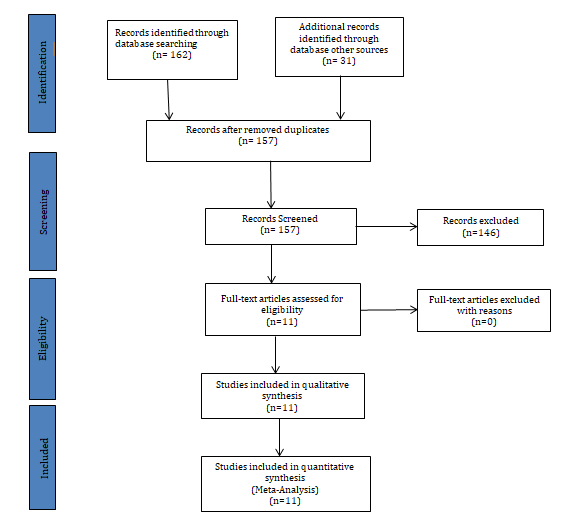
RESULTS
A total of 193 studies were identified. PubMed yielded 162 studies with other sources providing an additional 31 studies. After removal of duplicates, 157 studies were screened. Twenty studies were selected. Five studies were case reports. Three studies were meta-analysis. Ten studies were randomized controlled trials and two were review articles. This systematic review included 3,483 participants.
Two thousand nine hundred eighty-eight participants involved confirmation of endotracheal tube following intubation, 246 participants were involved identification of the cricothyroid membrane, and 269 participants were involved in ultrasound application in real-time intubation.
The overall sensitivity to confirm ET tube placement utilizing ultrasonography was 96.4% (95% CI 96.3975 ± 3.544). Specificity was 98.0% (95% CI 98.025 ± 1.364). Limitations were techniques utilized to confirm tube placement as well as sonographer training prior to studies. Accuracy of identification of cricothyroid membrane was 85.5% (95% CI 85.5 ± 8.82). Limitations was the variability in defining “accuracy”, ultrasound method utilized, and study populations. Study subjects who are morbidly obese will cause significant differences between accuracy of ultrasound and external palpation [6].
The overall success rate of ultrasound-guided intubation was 98% (95% CI 98 ± 1.96). Limitations included the variability is the study populations, methods of utilizing ultrasound throughout the intubation, limited sample size, and contexts in which studies were performed.
DISCUSSION
This systematic review demonstrates that ultrasonography is very accurate in confirming intubation. This correlates with previous studies demonstrating high efficacy in this respect [7]. Given capnography has been shown to be inaccurate in patients in cardiac arrest or massive pulmonary embolism and tube condensation has been shown to be a poor predictor of correct tube placement, ultrasound can be a useful modality to confirm endotracheal tube placement [1,8].
The traditional method of ascertaining bronchial placement of endotracheal tube has been auscultation of bilateral lungs sounds. However, recent studies have demonstrated auscultation of bilateral breath sounds is not specific for correct tube placement [9].
Ultrasound may also be a useful means to help demonstrate ventilation of both lungs. If ET tube is in correct position, bilateral equal motion of the diaphragm toward abdomen can be observed as well as bilateral lung sliding sign at the chest wall surface. If endobronchial placement is present, absence or restricted movement of the diaphragm as well as absence of lung sliding sign would be present on the non-ventilated side [10].
Ultrasound may also be used to perform intubation in real-time and a high rate of success with this method has been demonstrated. Marcinitak, et al. demonstrated characteristic real-time ultrasound findings throughout intubation [11].
These included identification of trachea and tracheal rings, visualization of vocal cords, widening of glottis as tracheal tube passes through, tracheal tube positioning above carina and chest wall movement upon ventilation. Esophageal intubation can be readily recognized by visualizing tube in the paratracheal space. Other studies have demonstrated ultrasound-guided tracheal intubation with a styleted tracheal tubes [12,13].
The accuracy of identifying the cricothyroid membrane was lower than expected. This may be secondary to the studies of interest were completing in those with difficult airways and morbid obesity. It can be postulated that this accuracy might be higher in those individuals with normal airways. The definition of accuracy was also very stringent in these studies, some only allowing success if identified with 5 mm of actual cricothyroid membrane. The actual clinical significance of performing an incision greater than 5 mm from actual cricothyroid membrane on the Cricothyroidotomy success rate is unknown.
CONCLUSION
Overall, these systematic reviews provides evidence of high sensitivity and specificity for ultrasound confirmation of ET tube placement, high success rate in ultrasound-guided intubation, and lower than expected accuracy in identifying the cricothyroid membrane. Ultrasonography should be considered for tube confirmation in patients in cardiac arrest and future applications of ultrasound may include intubation in real-time.
DISCLOSURE STATEMENT
None of the authors has any conflict of interest or financial issues to declare related to this publication.
REFERENCES
- Kelly JJ, Eynon CA, Kaplan JL, de Garavilla L, Dalsey WC. (1998). Use of tube condensation as an indicator of endotracheal tube placement. Ann Emerg Med. 31:575-578.
- MacLeod BA, Heller MB, Gerard J, Yealy DM, Menegazzi JJ. (1991). Verification of endotracheal tube placement with colorimetric end-tidal CO2 detection. Ann Emerg Med. 20: 267-270
- Aslani A, Ng S‐C, Hurley M, McCarthy KF, McNicholas M, McCaul CL. (2012). Accuracy of identification of the cricothyroid membrane in female subjects using palpation: an observational study. Anesth Analg. 114:987–992.
- You‐Ten KE, Desai D, Postonogova T, Siddiqui N. (2015). Accuracy of conventional digital palpation and ultrasound of the cricothyroid membrane in obese women in labour. Anaesthesia. 70:1230–1234.
- Moher D. Liberati A. Tetzlaff J. (2009). Preferred Reporting Items for Systematic Reviews and Meta-analyses: the PRISMA statement. Ann Intern Med. 151:264-269
- Siddiqui N, Yu E, Boulis S, You-Ten KE. (2018). Ultrasound Is Superior to Palpation in Identifying the Cricothyroid Membrane in Subjects with Poorly Defined Neck Landmarks: A Randomized Clinical Trial. Anesthesiology. 129(6):1132-1139.
- Tejesh CA, Manjunath AC, Shivakumar S, Vinayak PS, Yatish B, Geetha CR. (2016). Sonographic detection of tracheal or esophageal intubation: A cadaver study. Saudi J Anaesth. 10(3):314-316.
- Cook TM, Nolan JP. (2011). Use of capnography to confirm correct tracheal intubation during cardiac arrest. Anaesthesia. 66:1183-1184.
- Grmec S. (2002). Comparison of three different methods to confirm tracheal tube placement in emergency intubation. Intensive Care Med. 28(6):701-704.
- Hsieh KS, Lee CL, Lin CC, Huang TC, Weng KP, Lu WH. (2004). Secondary confirmation of endotracheal tube position by ultrasound image. Crit Care Med. 32:S374-S377.
- Marciniak B, Fayoux P, Hébrard A, Krivosic-Horber R, Engelhardt T, Bissonnette B. (2009). Airway Management in Children: Ultrasonography Assessment of Tracheal Intubation in Real Time? Anesth Analg. 108:461-465.
- Kundra P, Padala SRAN, Jha AK. (2020). Ultrasound guided tracheal intubation with a styleted tracheal tube in anticipated difficult airway. J Clin Monit Comput. 35(2):285-287.
- Fiadjoe JE, Stricker P, Gurnaney H, Nishisaki A, Rabinowitz A, Gurwitz A, et al. (2012). Ultrasound-guided Tracheal Intubation: A Novel Intubation Technique. Anesthesiology. 117:1389–1391.