Information Links
Related Conferences
Previous Issues Volume 2, Issue 1 - 2023
Sinonasal Polyposis: Quality of Life After Surgical Treatment: About 21 Cases
Belasri Anas,* Fatima Zahra Essahli, Achraf Amine Sbai, Drissia Benlfadil, Azzedine Lachgar, Adil Abdnbestein, Fahd Elayoubi
Department of Otorhinolaryngology and Cervico-Facial Surgery, Mohammed VI University Hospital of Oujda, Morocco
*Corresponding author: Belasri Anas, Department of Otorhinolaryngology and Cervico-Facial Surgery, Mohammed VI University Hospital of Oujda, BP 4806 Oujda University 60049 Oujda, Morocco, Tel: 0655793630; Email: [email protected].
Received Date: October 19, 2023
Published Date: November 24, 2023
Citation: Anas B, et al. (2023). Sinonasal Polyposis: Quality of Life After Surgical Treatment : About 21 Cases. Mathews J Otolaryngol. 2(1):06.
Copyrights: : Anas B, et al. © (2023).
ABSTRACT
Nasosinusal polyposis is a major health problem with important socio-economic implications. Our work presents a retrospective study of 21 patients operated on for nasosinusal polyposis, over a 10-Month, from January 2017 to January 2019 in the Otorhinolaryngology Department of Mohammed VI University Hospital Center in Oujda. The average age of our patients 39, 8 with a range from 16 to 66 years with a male predominance (sex ratio of 1,3). The objective of our study is to evaluate the quality of life and the severity of individual symptoms in patients with nasosinusal polyposis, were measured using the Sino-Nasal-Outcome Test 22 (SNOT-22). The main preoperative symptom score was nasal obstruction with a main score of 4,3, Anosmia had the second highest preoperative score of 3, 63. The clinical course was marked by improvement in nasal symptomatology with an improvement rate of 43% for nasal obstruction, 54% for anosmia, 50% for the need to blow nose.
Keywords: Nasosinusal Polyposis, Score SNOT-22, The Quality of Life.
INTRODUCTION
Nasosinusal polyposis is an inflammatory disease of the mucosa of the nasal cavity and sinuses, due to multifocal and bilateral edematous degeneration of the mucosa of the lateral masses of the ethmoid. It is characterized by the presence of smooth gelatinous translucent and pyriform polypous lesions. It predominates very clearly in adults and is part of chronic inflammatory diseases of the respiratory mucosa, hence the interest in systematic research for asthma, intolerance to aspirin, and nasal allergy. Rarer pediatric forms should lead to a search for mucociliary dysfunction or cystic fibrosis [1-20].
The diagnosis of this condition has benefited greatly from the advent of endoscopy and computed tomography.
The treatment is always medical, sometimes surgical, depending on symptomatic discomfort, socio-professional impact, comorbidity, extent and severity of the disease.
The objective of our study: Is to evaluate the impact of surgery on symptoms linked to PNS and its interaction with long-term quality of life [21-30].
MATERIAL AND METHODS
Retrospective study spread over a period of 2 years from January 2017 to January 2019, bringing together 21 patients with PNS operated on in the Otolaryngology department of the Mohammed VI University Hospital in Oujda.
For our study we used the rhinosinusitis symptom score: composed of 22 items from the SNOT-22 questionnaire (Figure 1), asking the patient about the existence of specific symptoms of acute or chronic rhinosinusitis (nasal obstruction, taste and/or smell disorders,, anterior rhinorrhea, posterior rhinorrhea, sneezing) and on the existence of secondary and non-specific symptoms (facial pain, ear pain, dizziness) and on the overall discomfort felt in relation to the nose.
The patient had to qualify each symptom according to its subjective degree of severity. The result of each questionnaire was carried out by telephone.
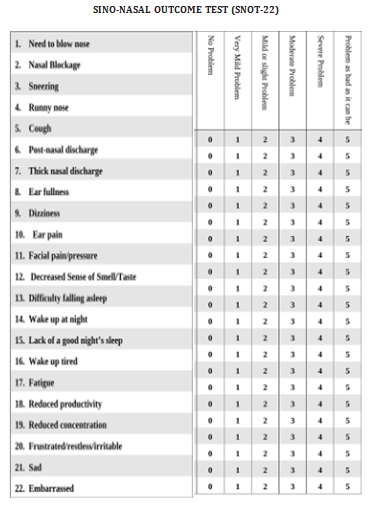
Figure 1. Rhinosinus symptoms score adapted from the SNOT -22, are rated from 0 (No problem) to 5 (very severe problem).
RESULTS
The average age of our patients was 39.8 years (extremes of 16 and 66 years). A male predominance was noted with 12 (57.2%) male patients compared to 9 (42.8%) female patients. The M/F sex ratio was 1,3 [31-40].
The most common symptom was nasal obstruction 95% of patients, Anosmia was reported by 90%, need to blow nose 85% of patients, the other most common symptoms were runny nose 71% and c 66%, facial pain and dizziness reported 14% of patients.
The principal preoperative symptom score was nasal obstruction, with a mean score of 4.35, with altered sense of smell or taste having the second highest preoperative score, 3.63 in patients with nasal polyps, need to blow nose was the third highest score with a mean of 3.27, thick nasal discharge and postnasal drip also had a high score of 2.6, facial pain was in the lower range preoperatively.
The elements covering aspects of health-related quality of life, waking up tired and waking up at night represented the main complaints of patients with an average score of 2.72 and 2.42 respectively.
Improvement in symptom scores after surgery were significant for all elements of the SNOT-22 in our patients: In our series the three main symptoms: nasal obstruction, altered smell/gout and need to blow nose: Are improved by 43%, 54%, 50% respectively in terms of rating.
All postoperative scores improved by at least 40%, with 16 items improving by more than 50% at 10 months postoperatively.
Generally, the average SNOT-22 total score before the operation was 45.4 which decreased to 18.27 postoperatively, improving by 59.75%.
DISCUSSION
Nasosinusal polyposis PNS is defined as a chronic inflammatory disease of the nasal mucosa, bilateral and multifocal, externalized in the nasal cavity in the form of polyps [26,30], which can alter the quality of life [41-50].
The exact prevalence rate is unknown and can be estimated between 1% [31] and 4% of the population [32].
The average age of patients was 39.8 years with extreme ages (16-66 years) in our series, the review of the literature shows a male predominance [35,38].
The evaluation of quality of life in clinical practice is an additional parameter that can be used to evaluate the effectiveness of various treatments: corticosteroid therapy represents the basis of medical treatment [41].
-general corticosteroid therapy: prednisolone 1mg/kg/day or methylprednisolone 0.8mg/kg/day for 10 days, associated with oral antibiotic coverage with amoxicillin and clavulanic acid at a dose of 1g morning and evening for 10 days.
-local corticosteroid therapy: spray of inhaled corticosteroid daily at the rate of two sprays per nostril per day (fluticasone 50cmg).
The patient returned after 3 months, the significant points of effectiveness of the basic treatment are: improvement of nasal obstruction, reduction or disappearance of anosmia. if the symptoms are well controlled, simple local corticosteroid therapy will be continued for months.
Other treatments can be used:
-Antihistamines in the event of an associated allergy or if the symptoms of nasal hyperreactivity are poorly controlled by local corticosteroid therapy [51-69].
-Immunostimulants and immune modulators [70,71]: sometimes make it possible to reduce the frequency and importance of superinfections in the PNS, especially in winter.
-crenotherapy [72]: After liberation of the nasal cavities, after medical treatment or after polypectomy.
-saline nasal sprays [73].
Surgical treatment occupies a very important place in PNS that is advanced and resistant to medical treatment.
Surgical techniques for the nasal-sinus cavities in the context of PNS have evolved considerably in recent years, beginning with simple polypectomy and transfacial ethmoidectomy currently leading to endoscopic endonasal surgery [74,75].
The SNOT-22 questionnaire developed and validated by Hopkins et al. [76] is the most effective tool currently available to evaluate the severity and impact of clinical symptoms of PNS, examining data from 21 patients undergoing surgery for the PNS in comparison with studies of similar construction (Table 1).
Kosugi and Vitor [35] analyzed a group of patients with chronic rhinosinusitis using SNOT-22, found that the most common and severe symptoms were nasal obstruction, anosmia and postnasal drip. , they demonstrated one of the symptom scores after nasal surgery.
More recently, Abdalla and Hopkins [36] conducted a study that aimed to assess individual symptoms based on the SNOT-22 in patients with RSC with or without nasal polyposis. They found that the top three symptoms in terms of severity and prevalence were nasal obstruction, anosmia and the need to blow nose, consistent with the EPOS2012 diagnostic criteria.
For our series we found that nasal obstruction and anosmia were the most frequent and serious symptoms, the need to blow nose was the third most serious symptom an average of 3.27.
Runny nose and thick discharge are also symptoms widely observed by patients preoperatively.
The least problematic symptoms are ear pain, facial pain and dizziness.
Table 1. Comparison of the SNOT-22 Score of Our series with studies of similar construction
|
Average Preoperative Symptom Score |
Average Symptom Score 1 Year Postoperative |
|||||
|
The Elements of The SNOT-22 Score |
Abdalla/Hopkin (36) |
Kosugi (35) |
Our Series |
Abdella/Hopkin (36) |
Kosugi (35) |
Our Series |
|
1-Need to blow your nose |
2.9 |
3 |
3.27 |
1.45 |
1.43 |
1.63 |
|
2-Sneezing |
1.9 |
3 |
1.77 |
0.8 |
1.69 |
0.95 |
|
3-Runny nose |
2.5 |
3.21 |
3.13 |
1.4 |
1.1 |
1.77 |
|
4-Post nasal discharge |
2.3 |
3.31 |
2.72 |
0.85 |
1.37 |
1.5 |
|
5-Thick nasal discharge |
2.4 |
2.76 |
3 |
1.1 |
1.33 |
1.63 |
|
6-Clogged ears |
1.6 |
2.66 |
1.22 |
0.6 |
0.98 |
0.58 |
|
7-Dizziness |
0.8 |
1.48 |
0.81 |
0.4 |
0.79 |
0.27 |
|
8-Ear pain |
0.6 |
1.43 |
1.36 |
0.3 |
0.65 |
0.27 |
|
9-Facial pain |
1.6 |
2.81 |
1.5 |
0.7 |
0.99 |
0.45 |
|
10-Nasal obstruction |
3.8 |
4.25 |
4.36 |
2.35 |
1.3 |
2.45 |
|
11-Cough |
1.3 |
1.79 |
1.09 |
0.4 |
1.12 |
0.27 |
|
12-Difficulty sleeping |
1.4 |
3.7 |
1.36 |
0.5 |
0.96 |
0.68 |
|
13-Waking up at night |
2.1 |
3.47 |
2.45 |
0.7 |
1.25 |
1.22 |
|
14-Poor sleep |
2.2 |
3.19 |
1.9 |
0.8 |
1.01 |
0.95 |
|
15-Wake up tired |
2.2 |
2.73 |
2.72 |
0.95 |
0.88 |
1.22 |
|
16-Fatigue during the day |
1.9 |
2.64 |
1.63 |
0.65 |
1 |
0.68 |
|
17-Loss of concentration |
1.6 |
2.75 |
1.5 |
0.6 |
0.83 |
0.58 |
|
18-Agitation/irritability |
1.8 |
2.35 |
1.77 |
0.7 |
0.97 |
0.95 |
|
19-Low moral |
1 |
3.42 |
1.9 |
0.3 |
0.9 |
0.68 |
|
20-Gene/discomfort |
1.4 |
2.55 |
1.22 |
0.8 |
0.62 |
0.54 |
|
21-Decrease in productivity |
1.6 |
2.22 |
1.36 |
0.7 |
0.27 |
0.4 |
|
22-Insomnia |
3.6 |
3.66 |
3.68 |
2.35 |
1.69 |
1.63 |
The impact of surgery on the postoperative symptom score is remarkable.
Exceptional short and long term results have already been reported in the literature. Abdalla and Hopkins [36] reported an improvement in quality of life for 56% of their patients with a follow-up duration of 3 months.
The UK Nasosinusinusal Polyposis Audit used the SNOT-22 to demonstrate a significant reduction in patients' symptoms following nasal surgery [72].
We showed in this study that surgery provided improvements in all symptom areas
All 22 post-operative score items improved by at least 40%. 16 items having improved by more than 50% 1 year after the operation. The average total score improved to a greater extent to 57.75% [77].
Table 2. Comparison of the total mean SNOT-22 score of our series with studies of similar construction
|
Author |
MEAN TOTAL Preoperative SNOT-22 SCORE |
AVERAGE TOTAL post-operative SNOT-22 SCORE |
|
ABDALLA [36] |
41 |
18.3 |
|
KOSUGI [35] |
60.02 |
16.02 |
|
Our Series |
45.4 |
18.27 |
The objective of our study: is to evaluate the quality of life and the severity of individual symptoms in patients with nasal polyposis were measured using the Sino-Nasal-Outcome Test 22 (SNOT-22). The impact of surgery on symptoms is remarkable with short-and long-term results reported. The main preoperative symptom score was nasal obstruction with a mean score of 4.3, anosmia obtained the second highest preoperative score of 3.63 in patients suffering from nasal polyps. The clinical evolution was marked by the improvement of nasal symptoms with an improvement rate of nasal obstruction at 43%, anosmia 54%, and the need to blow nose at 50%.
REFERENCES
- Legent F. (1981). Cahier d’anatomie. ORL. Tome II. Paris: Edition Masson.
- Pierre B, Jean-Marc C. (2005). Anatomie ORL. Paris: Médecine–Sciences Flammarion. pp. 178-229.
- Bouchet A, Cuilleret J. (1997). Anatomie 1: topographie descriptive et fonctionnelle: le S.N.C, la face, la tête egt les organes des sens. 2nd edn. SIMEP.
- Eloy P, Nollevaux MC, Bertrand B. (2005). Physiologie des sinus paranasaux. EMC-Oto-rhino-laryngologie. 2:185-197.
- Friedmann I, Bird ES. (1971). Ciliary structure, ciliogenesis, microvilli. (Electron microscopy of the mucosa of the upper respiratory tract). Laryngoscope. 81(11):1852-1868.
- Proetz AB. (1953). Essays on the Applied Physiology of the Nose. Missouri: Annals Publishing Company.
- Klossek JM. (1998). La physiologie nasosinusienne. Rev fr Allergo L. 38(7):579-583.
- Bonfils P, Didier A, Jankowski R, Pujet JC. (1997). Nasosinus polyposis and asthma: when two chronic diseases combine. Paris Symposium.
- le phénomène inflammatoire , [email protected].
- Plouin-Gaudon I, Clement S, Huggler E, Chaponnier C, François P, Lew D, et al. (2006). Intracellular residency is frequently associated with recurrent Staphylococcus aureus rhinosinusitis. Rhinology. 44(4):249-254.
- Stow NW, Douglas R, Tantilipikorn P, Lacroix JS. (2010). Superantigens. Otolaryngol Clin North Am. 43(3):489-502.
- Drake-Lee AB, Barker TH. (1984). Free and cell bound IgE in nasal polyps. J Laryngol Otol. 98(8):795-801.
- Robinson AM, Kern RC, Foster JD, Fong KJ, Pitovski DZ. (1998). Expression of glucocorticoid receptor mRNA and protein in the olfactory mucosa: physiologic and pathophysiologic implications. Laryngoscope. 108(8 Pt 1):1238-1242.
- Small P, Frenkiel S, Black M. (1981). Multifactorial etiology of nasal polyps. Ann Allergy. 46(6):317-320.
- Jankowski R, Wayoff M. (1992). Physiopathologie des sinus. Edition technique. Encycl Méd Chir. 204(16):A10.
- Peynegre R, Coste A. (1994). Polypose naso-sinusienne. Encycl Med Chir. Paris. Oto-rhinolaryngol. p. 10.
- Les Rhinorrhees. Available at: www.meduniv-tours.fr.
- Drouet M, Sabbah A, Le Sellin J, Bonneau JC, Fourrier E. (1990). Syndrome de Fernand Widal et intolérance aux sulfites: problèmes thérapeutiques en générale et ORL en particulier. Allerg Immunol (Paris). 22(3):90-96.
- Moneret-Vautrin DA, Wayoff M, Hsieh V, Wirte, Maria Y, Jankowski R. (1989). Le NARES, maillon evolutif de la triade de Fernand-Widal [NARES syndrome. A developing link in the Fernand-Widal triad]. Ann Otolaryngol Chir Cervicofac. 106(1):47-50.
- Poulichet JP. PNS: Acide arachidonique, prostaglandines, leucotrienes: Encycl Med Chir. Paris. ORL, 9-1988, 20395, A10, 3p.
- Bonfils P. (2011). Polypose naso-sinusienne. EMC (Elsevier Masson SAS, Paris), Oto-rhinolaryngologie. 20-395-A-10.
- Darrouzet V, Denoyelle F. (2005). Génétique et maladies ORL. Paris: Éditions de la Sociétéfrançaise d’ORL et de chirurgie de la face et du cou. pp. 231-272.
- Bachet C, Gevaert P, Cauwenberge PV. (1999). Nasal polyposis: a new concept on the formation of polyps. ACI International. pp. 130-135.
- Larsen PL, Tos M. (1991). Origin of nasal polyps. Laryngoscope. 101(3):305-312.
- Takasaka T, Kaku Y, Hozawa K. (1986). Mast cell degranulation in nasal polyps. Acta Otolaryngol Suppl. 430:39-48.
- Coste A. (2001). Poluposenasosinusienne. Encyclopédie orphanet juin.
- Crampette L. La presse médicale le 22-29 décembre 2001/0/n :39-40/cahier 2.
- Dessi P, Facon F. (2003). Polypose naso-sinusienne chez l’adulte. Encycl Med Chir; Oto-rhinolaryngologie. 20-395-A-10, 15p.
- Newton JR, Ah-See KW. (2008). A review of nasal polyposis. Therapeutics and Clinical Risk Management. 4(2):507-512.
- Giger R, Landis BN, Friedrich JP, Lacroix JS. (2005). Rhinosinusite chronique et polypose nasale. Schweiz Med Forum. 5:1054-1060.
- Drake-Lee AB, Barker TH. (1984). Free and cell bound IgE in nasal polyps. J Laryngol Oto. 98:795-801.
- Hedman J, Kaprio J, Poussa T, Nieminen MM. (1999). Prevalence of asthma, aspirin intolerance, nasal polyposis and chronic obstructive pulmonary disease in a population-based study. Int J Epidemiol. 28(4):717-722.
- Triglia JM, Nicollas R. (1997). Nasal and sinus polyposis in children. Laryngoscope. 107(7):963-966.
- Moalla J, Dhouib H, Kallel S, Sellami M, Charfeddine I, Ghorbel A. (2008). Complications orbitaires de la polypose nasosinusienne de l’enfant. J TUN ORL. 21:52-54.
- Kosugi EM, Chen VG, Fonseca VM, Cursino MM, Mendes Neto JA, Gregório LC. (2011). Translation, cross-cultural adaptation and validation of SinoNasal Outcome Test (SNOT): 22 to Brazilian Portuguese. Braz J Otorhinolaryngol. 77(5):663-669.
- Abdalla S, Alreefy H, Hopkins C. (2012). Prevalence of sinonasal outcome test (SNOT-22) symptoms in patients undergoing surgery for chronic rhinosinusitis in the England and Wales National prospective audit. Clin Otolaryngol. 37(4):276-282.
- Safaa L. Place de l'ethmoïdectomie fonctionnelle endonasale vidéo-endoscopique dans la prise en charge de la polypose naso-sinusienne. CHU-Hassan II-Fes. Thèse année2008, faculté de médecine et de la pharmacie–Fès.
- Chaouir S, Hanine A, Amic T, Abrouq A, Ameur MB. (2001). Les Polyposes Naso-Sinusiennes: Apport de la tomodensitométrie. A propos de 41 cas. Médecine du Maghreb. 58:30-33.
- Peynegre R, Coste A. (1994). Polypose naso-sinusienne. Encycl Med Chir. paris. Oto-rhinolaryngol. pp. 310-320.
- Rouvier P, Vandeventer G, El hkoury J, De Lanversion H. (1991). Les résultats à long terme (sur 5ans) de l’éthmoïdectomie dans la polypose invalidante. J Fr ORL. 40(2):102-105.
- BONFILS P. (2007). Evaluation of the combined medical and surgical treatment in nasal Polyposis. I: Functional results. Acta Oto-Laryngologica. 127(4):436-446.
- Darrouzet V, Denoyelle F. (2005). Génétique et maladies ORL. Paris: Éditions de la Société française d’ORL et de chirurgie de la face et du cou. pp. 231-272.
- Bachet C, Gevaert P, Cauwenberge PV. (1999). Nasal polyposis: a new concept on the formation of polyps. ACI international. pp. 130-135.
- Larcen PL, Tos M. (1991). Origin of nasal polyps. Laryngoscope. 101(3):385-388.
- Takasaka T, Kaku Y, Hozawa K. (1986). Mast cell degranulation in nasal polyps. Acta Otolaryngol Suppl. 430:39-48.
- Stephene Liwarek. polypose naso-sinusienne. diagnostic et prise en charge.
- Service ORL. Hôpital militaire Moulay Ismail–Meknès.
- Rombeaux PH, De Toeuf C., Hamoir M. (2001). Polypose nasosinusienne: résultats à un an de la chirurgie endoscopique endosinusienne suivie d’une corticothérapie topique chez 72 patients. Ann Otolaryngol Chir Cervicofac. 118(5):291-298.
- Chaouir S, Hanine A, Amic T, Abrouq A, Ameur MB. (2001). Les Polyposes Naso-Sinusiennes: Apport de la tomodensitométrie. A propos de 41 cas. Médecine du Maghreb. 85:30-33.
- Picry A, Mortuaire G, Szymanski-vandenhende C, Chevalier D, Leroy X. (2014). Caractérisation histopathologique de la polypose nasosinusienne et corrélations clinicohistologiques. Annales françaises d’oto-rhino-laryngologie et de pathologie cervico-faciale. 131(4):A161-A171.
- Bonfils P, Tran Khai Hoana N, Karmochkineb M, Laccourreyea O. (2014). Polypose naso-sinusienne et déficit en sous-classe d’immunoglobuline G Annales françaises d’oto-rhino-laryngologie et de pathologie cervico-faciale. 131(2014):157-162.
- BOUSAADANI AEL, JAHD BEL, SERHIER B, ABADA R, ROUBAL J, MAHTAR M. (2014). Etude évaluative sur l’impact du traitement médico-chirurgical des polyposis naso-sinusiennes sur la qualité de vie des patients. Annales françaises d’oto-rhinolaryngologie et de pathologie cervico-faciale. 131:A161-A171.
- Serrano E. (1987). Les Polyposes Naso-sinusiennes: Place Du Traitement Médical. Toulouse.
- Bonfils P. (1998). Medical Treatment of Paranasal Sinus Polyposis: A Prospective Study in 181Patients. Ann Otolaryngol Chir Cervicofac. 115(4):202-214.
- Jankowski R, Bodino C. (2003). Evolution of symptoms associated to nasal polyposis following oral steroid treatment and nasalization of the ethmoid--radical ethmoidectomy is functional surgery for NPS. Rhinology. 41(4):211-219.
- Batteur B, Strunski V, Caprio D, Berthet V, Goin M. (1994). Récidive de la polypose nasosinusienne après ethmoidectomie par voie endonasale. Aspects fonctionnels, endoscopiques, tomodensitométriques et implications chirurgicales [Recurrence of nasosinusal polyposis after ethmoidectomy by endonasal approach. Functional, endoscopic, x-ray tomographic aspects and surgical implications]. Ann Otolaryngol Chir Cervicofac. 111(3):121-128.
- Fombeur JP, Ebbo D, Lecomte F, Simon D, Koubbi G, Barrault S. (1993). Résultats préliminaires de 132 ethmoïdectomies par voie endonasale [Initial results of 132 ethmoidectomies by endonasal approach]. Ann Otolaryngol Chir Cervicofac. 110(1):29-33.
- Settipane GA, Chafee FH. (1977). Nasal polyps in asthma and rhinitis. A review of 6,037 patients. J Allergy Clin Immunol. 59(1):17-21.
- El korbi A, Kolsi N, Alaya B, Ben rhaiem Z, Harrathi Z, Koubaa J. (2014). Polypose naso-sinusienne : existe-t-il des facteurs prédictifs de récidive après traitement chirurgical ? Annales françaises d’oto-rhino-laryngologie et de pathologie cervico-faciale. 131:A104-A160.
- Dufour X, Bedier A, Ferrie JC, Gohler C, Klossek JM. (2004). Diffuse nasal polyposis and endonasal endoscopic surgery: long-term results, a 65-case study. Laryngoscope. 114(11):1982-1987.
- Lund VJ, Mackay IS. (1993). Staging in Rhinosinusitis. Rhinology. 31(4):183-184.
- Freche Ch, Fantanel JP. (1996). L’obstruction nasale. Edition Arnette, Paris.
- Peynegre R, Coste A. (1994). Polypose naso-sinusienne. Encycl Med Chir. Paris. Oto-rhinolaryngol. pp. 310-320.
- Serrano E, Wessel F. (2003). La maladie de Fernand Widal. Diagnostic et traitement. Revue française d’allergologie et d’immunologie clinique. 43:135-137.
- Toma GA, Stein GE. (1968). Nasal Polyposis in Cystic Fibrosis. The Journal of Laryngology & Otology. 82:265-268.
- Wayoff M, Foliguet B, Bigel ML, Cordonnier JC, Lardenet J. (1982). L'intérêt du syndrome d'immotilité ciliaire en O.R.L [Importance of the immotile cilia syndrome in E.N.T. field]. Ann Otolaryngol Chir Cervicofac. 99(6):257-261.
- Wentges RT. (1972). Edward Woakes: the history of an eponym. J Laryngol Otol. 86(5):501-512.
- Alobid I, Benítez P, Bernal-Sprekelsen M, Roca J, Alonso J, Picado C, et al. (2005). Nasal polyposis and its impact on quality of life: comparison between the effects of medical and surgical treatments. Allergy. 60(4):452-458.
- Aboud SK, Husain S, Gendeh BS. (2014). Evaluation on quality of life in patients with nasal polyposis managed with optimal medical therapy. Allergy Rhinol (Providence). 5(1):2-8.
- Freche CH. (1996). La polypose naso-sinusienne de l’adulte : expérience personnelle. Revue officielle de la société française d’O.R.L. 37:42-50.
- Peynegre R, Coste A. (1994). Polypose naso-sinusienne. Encycl Med Chir paris. Oto-rhinolaryngol. pp. 310-320.
- Levenz J F, Debidour A. (1990). Thérapeutique thermale en ORL. Rev Off Soc Fr ORL. 4:53-58.
- Rabago D, Zgierska A, Mundt M, Barrett B, Bobula J, Maberry R. (2002). Efficacy of daily hypertonic saline nasal irrigation among patients with sinusitis. Randomized controlled trial. J Fam Pract. 51(12):1049-1055.
- Dessi P, Facon F. (2003). Polypose naso-sinusienne chez l’adulte. Encycl Med Chir. Oto-rhinolaryngologie. 20-395-A-10. p. 15.
- Stoll D, Dumon T, De Monredon O. (1998). Traitement chirurgical de la polypose nasosinusienne. Rev ft Allergol. 38(7):647-651.
- Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP. (2009). Psychometric validity of the 22-item Sinonasal Outcome Test. Clin Otolaryngol. 34(5):447-454.
- Hopkins C, Browne JP, Slack R, Lund V, Topham J, Reeves B, et al. (2006). The national comparative audit of surgery for nasal polyposis and chronic rhinosinusitis. Clin Otolaryngol. 31(5):390-398.