Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2023
Rectal Invasion by Metastatic Prostat Cancer 15 Years after Prostate Cancer Surgery
Vedat Goral1,*, Zeynep Bayramoglu2, Ozcan Yildiz3, Kerem Mert Goral4
1Department of Gastroenterology, Istanbul Medipol University Medical School Hospital, Istanbul, Turkey
2Department of Pathology, Istanbul Medipol University Medical School Hospital, Istanbul, Turkey
3Department of Medical Oncology, Istanbul Medipol University Medical School Hospital, Istanbul, Turkey
4Koc University Medical School, Istanbul, Turkey
*Corresponding author: Prof. Dr. Vedat Goral, Istanbul Medipol University, Medipol Mega Hospital Goztepe Mah. 2309 Sk. No: 6 Bagcilar 34214, Istanbul, Turkey. Tel: 0090 533 5256614. E-mail: [email protected].
Received Date: March 10, 2023
Published Date: March 27, 2023
Citation: Goral V, et al. (2023). Rectal Invasion by Metastatic Prostat Cancer 15 Years after Prostate Cancer Surgery. Mathews J Gastroenterol Hepatol. 8(1):18.
Copyrights: Goral V, et al. © (2023).
ABSTRACT
Prostate cancer is the most common cancer in men and has a high risk of metastasis. It often metastasizes to the iliac lymph nodes, bone, lungs, less frequently to the bladder, liver, and adrenals. The most common location for distant metastases is the bones. Although it is a frequently metastasizing cancer, rectal metastasis is rare. Few cases have been reported in the literature. In this case, we discuss the rectal invasion that occurred years later in a patient who presented with constipation and underwent prostate cancer surgery 15 years ago.
Keywords: Prostatic Cancer, Rectal Invasion, Prostat Cancer Surgery.
INTRODUCTION
Prostate cancer is the second most diagnosed cancer worldwide in men. Usually typical sites for metastasis include bone, lung, and liver. Prostate cancer with gastrointestinal involvement, particularly rectal, has been rarely reported in the literature. In this case, we discuss the rectal invasion that occurred years later in a patient who presented with constipation and underwent prostate cancer surgery 15 years ago.
CASE REPORT
Our patient (80 years old) had constipation refractory to drug therapy. He had a history of prostate cancer operation 15 years ago. He had no LHRH treatment. Colonoscopy was performed for the etiology of constipation. In the rectum, narrowing of the lumen and hard and thickening of the mucosa were detected (Picture 1). Six biopsies were taken from the rectum. In the biopsy, prostate adenocarcinoma metastasis was detected in the rectum. A microscopic examination of the rectal biopsy specimen revealed a glandular architecture with prominent nucleoli that infiltrated the rectal mucosa and submucosa (Figure 1 & 2). No intraepithelial neoplasia was found in the rectal mucosa. Immunohistochemical staining demonstrated NKX3.1 positivity (Figure 2); CK7, CK20 and CDX-2 negativity. Tumor cells were compatible with prostate origin in the presence of histopathological and immunohistochemical findings.
In abdominal MR examination; A mass lesion with ureteral invasion was detected in the patient who was known to have an operated prostate, whose radial extensions measuring up to 5 mm were observed, extending to the dentate line at the anorectal junction, which completely covers the rectum along its walls and narrows it almost completely. Small lymph nodes measuring up to 3 mm showing diffusion restriction were seen in the mesorectal fascia. In PSMA Ga-PET/BT; Intense pathologically increased PSMA uptake is observed in the tumoral lesion, which fills the lumen along a long segment into the rectum, infiltrates the seminal vesicle level on the left, and has blurred borders with the bladder (prostate ca metastasis?) In PSMA Ga-PET/BT; Intense pathologically increased PSMA uptake is observed in the tumoral lesion, which fills the lumen along a long segment into the rectum, infiltrates the seminal vesicle level on the left, and has blurred borders with the bladder (prostate ca metastasis?). Contamination and a few millimetric lymph nodes are observed in the mesorectal fat plane. Pathologically increased PSMA uptake is observed in the small lymph node in the right inguinal region (metastasis?). In the sclerotic lesion observed in the left pedicle of the third T8 vertebra, pathologically increased PSMA uptake is observed (metastasis?). PSA level was determined as 34.5 ng/ml (N:> 70 years, < 4.4 ng/ml).
This case was an interesting case for us. Years later, we encountered a case with rectal invasion of operated prostate cancer for the first time. The patient was referred to the medical oncology department. Treatment was started in medical oncology.
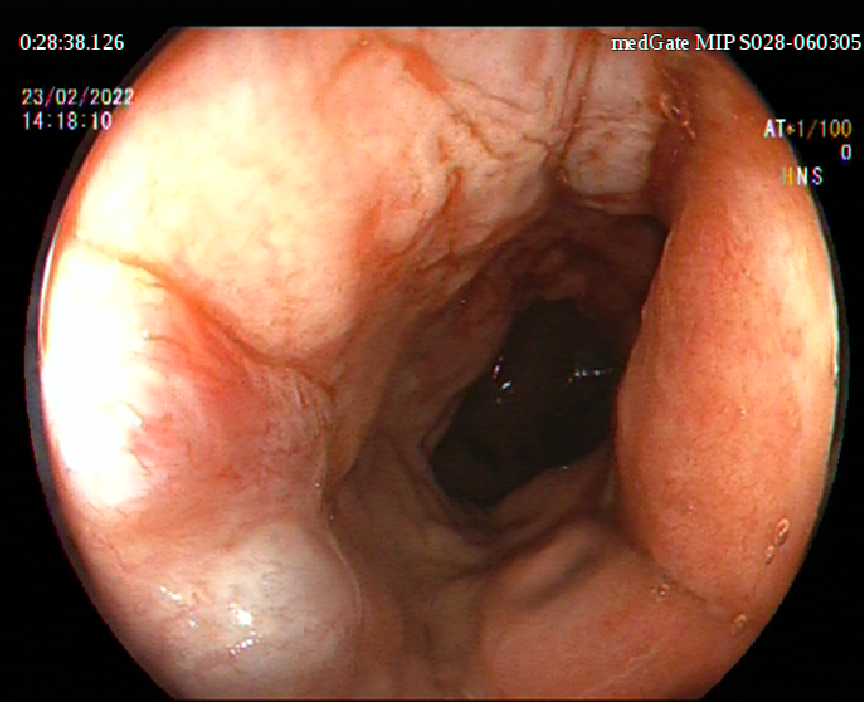
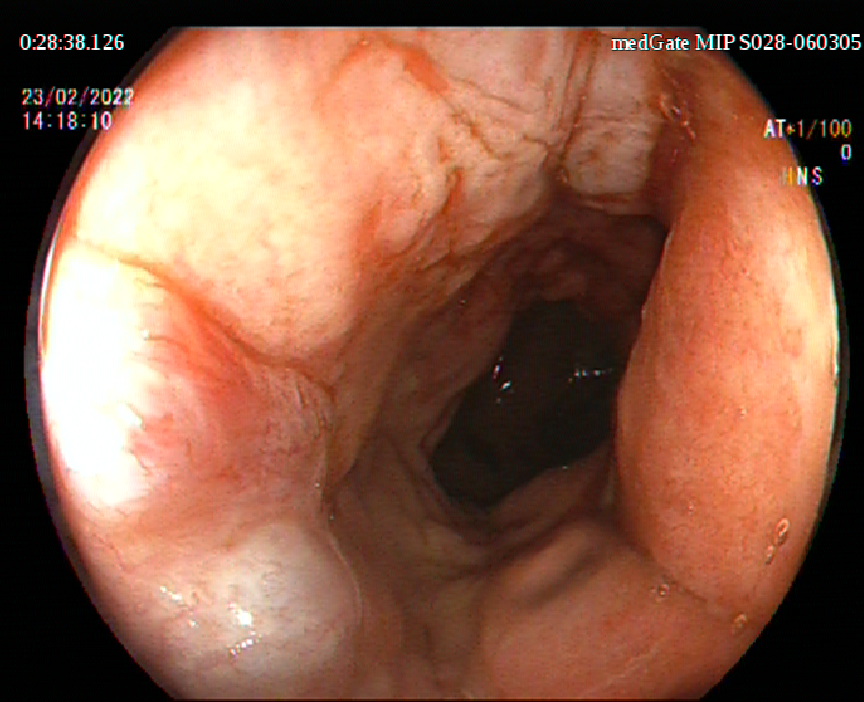
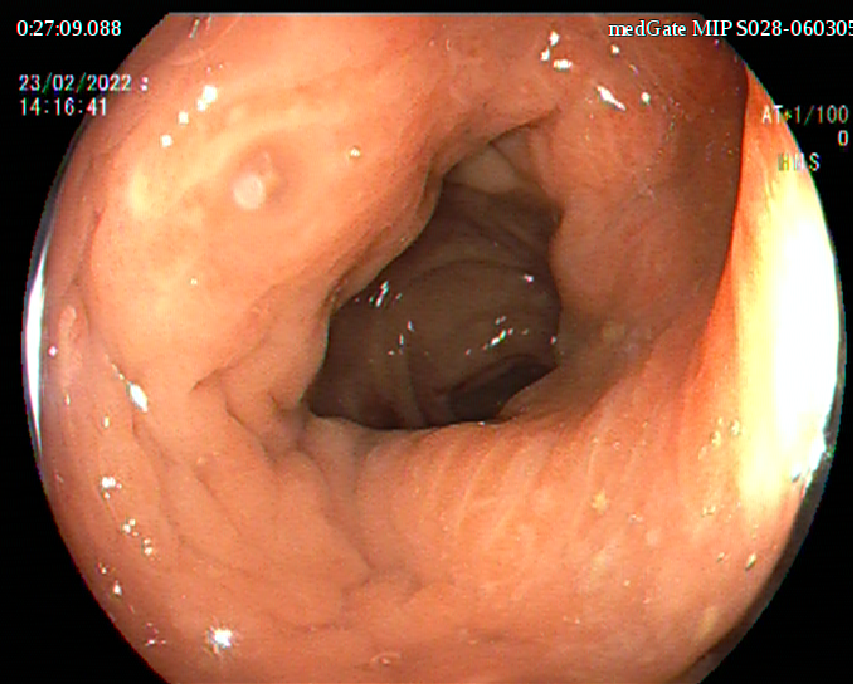
Picture 1. Thickness of rectal mucosa.
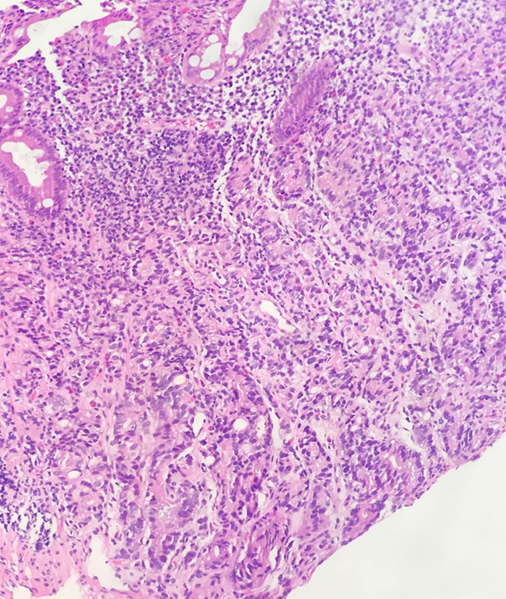
Figure 1. In the biopsy specimen of hematoxylin and eosin staining, there were prominent nucleoli in tumor cells under the surface epithelium.
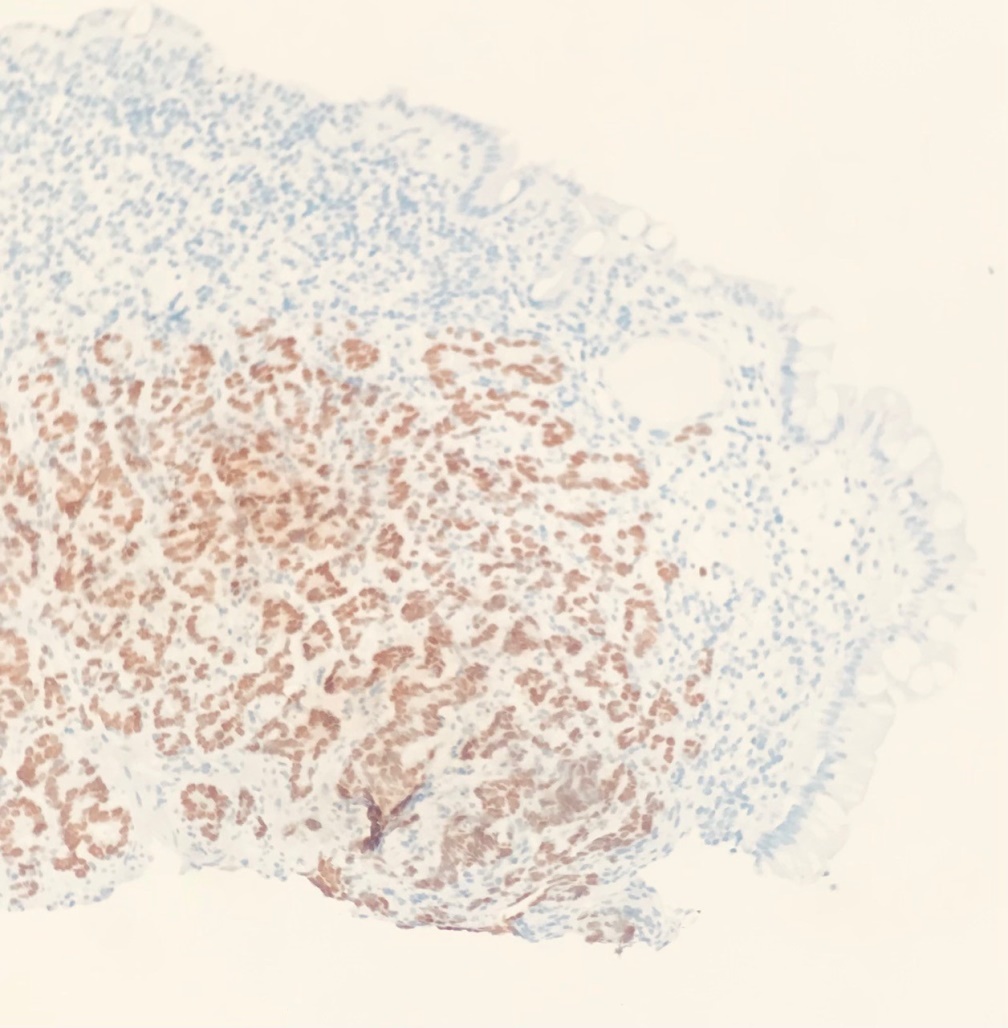
Figure 2. Immunohistochemical staining for NKX3.1 positivity shows strong expression in tumor cells but not in the normal rectal crypt.
DISCUSSION
Prostate cancer is the most common cancer in men and has a high risk of metastasis. It often metastasizes to the iliac lymph nodes, bone, lungs, less frequently to the bladder, liver, and adrenals. The most common location for distant metastases is the bones [1]. Although it is a frequently metastasizing cancer, rectal metastasis is rare. Few cases have been reported in the literature [1-3].
The spread of prostate cancer to colorectal tissues may occur in different ways [4-5]. Cancer can directly invade the rectum through Denonvilliers' fascia [6]. Because of the same lymphatic drainage of the rectum and prostate, metastasis can be seen through the lymphatic route [3]. Another very rare method is transplantation into perirectal or rectal tissue during needle biopsy [4]. In some autopsy series, invasion through adjacent rectum has also been shown in patients with prostate carcinoma [6].
In rectal metastasis due to prostate cancer, sometimes rectal bleeding, rectal discomfort or bowel obstruction may be present [7,8]. Our patient had chronic constipation that did not respond to drug therapy, and colonoscopy due to chronic constipation revealed thickening and irregularity in the rectal wall. In the biopsy taken from here, it was reported that the patient's findings were due to prostate cancer invasion. Our patient was referred to medical oncology for treatment. In the literature, rectal metastases due to prostate cancer have been rarely reported. In some literature, polypolypoid formation has presented as a polypoid mass or intestinal obstruction [8]. The possibility of metastasis should be considered in a patient with prostate cancer presenting with the complaint of rectal bleeding [9,10].
CONCLUSION
Patients with a history of prostate cancer should have regular check-ups. As in our patient, if there is a history of chronic constipation and especially a prostate cancer operation in the past, the patient should be checked at regular intervals, and colonoscopic control and serum CEA and PSA tests should be performed in male cases with chronic constipation. A biopsy should also be taken from the rectum for control purposes. In male patients with a history of prostate cancer, when malignancy is detected in the rectum, invasion due to prostate cancer should be considered first.
REFERENCES
- Obana T, Kishimoto M. (2021). A case of circumferential rectal wall thickening caused by prostate cancer invasion concomitant with ischemic colitis. Nihon Shokakibyo Gakkai Zasshi. 118(2):154-160. DOI: 10.11405/nisshoshi.118.154.
- Guo CC, Pisters LL, Troncoso P. (2009). Prostate cancer invading the rectum: a clinicopathological study of 18 cases. Pathology. 41(6):539-543. DOI: 10.1080/00313020903071611.
- Wadehra A, Alkassis S, Rizwan A, Yazdanpanah O. (2021). Rectal Invasion by Metastatic Prostate Adenocarcinoma. Cureus. 13(6):e15569. DOI: 10.7759/cureus.15569.
- Tang T, Yang Z, Zhang D, Qu J, Liu G, Zhang S. (2017). Clinicopathological study of 9 cases of prostate cancer involving the rectal wall. Diagn Pathol. 12(1):8. DOI: 10.1186/s13000-017-0599-2.
- Bowrey DJ, Otter MI, Billings PJ. (2003). Rectal infiltration by prostatic adenocarcinoma: report on six patients and review of the literature. Ann R Coll Surg Engl. 85(6):382-385. DOI: 10.1308/003588403322520726.
- Leibovici D, Spiess PE, Pisters LL. (2008). Rectal Wall Invasion of Locally Advanced Prostate Cancer: Comparison of Magnetic Resonance Imaging with Transrectal Ultrasound. Cancer Imaging: Lung and Breast Carcinomas. 2:637-640.
- Hon N, Lynn N, Chen TF. (2005). Rectal infiltration by prostatic adenocarcinoma: a report on six patients and review of the literature. Ann R Coll Surg Engl. 87(1):72-73. DOI: 10.1308/1478708051261.
- Uwagbale E, Onukogu I, Bodiwala V, Agbroko S, Sonpal N. (2021). Metastatic Prostate Cancer Presenting as a Rectal Polyp: A Rare Occurrence. Cureus. 13(5):e15115. DOI: 10.7759/cureus.15115.
- Gengler L, Baer J, Finby N. (1975). Rectal and sigmoid involvement secondary to carcinoma of the prostate. Am J Roentgenol Radium Ther Nucl Med. 125(4):910-917.
- Azzi P, Bossé D, Cagiannos I, Borowy-Borowski P, Tiberi D. (2022). Primary Adenosquamous Carcinoma of the Prostate with Rectal Invasion. Case Rep Urol. 2022:7613482. DOI: 10.1155/2022/7613482.