Previous Issues Volume 2, Issue 2 - 2017
Prevalence and Causes of Visual Impairment among Patients in Juaben Hospital Eye Clinic, Ghana
Derrick Owusu Ansah
Department of Optometry and Visual Science, KNUST-Kumasi, Ghana.
Corresponding Author: Derrick Owusu Ansah, Department of Optometry and Visual Science, KNUST-Kumasi, Ghana, Tel: +233500016591 E-Mail: [email protected]
Received Date: 20 Jun 2017 Accepted Date: 05 Jul 2017 Published Date: 10 Jul 2017
Copyright © 2017 Ansah DO
Citation: Ansah DO. (2017). Prevalence and Causes of Visual Impairment among Patients in Juaben Hospital Eye Clinic, Ghana. Mathews J Ophthalmol. 2(2): 017.
ABSTRACT
Background: There is limited data on the magnitude of visual impairment (VI) and blindness in Ghana. This information is useful in planning preventive programs and improving on the eye-care services of hospitals to people in the nearby communities. Purpose: To determine the prevalence and causes of VI and blindness among eye clinic patients at the Juaben Hospital. Methods: A retrospective study was conducted among patients attending Juaben Hospital Eye Clinic from January 1st 2015 to June 30th 2015. Information on demographics, presenting visual acuity and diagnosis were obtained from patients’records. Statistical Package for Social Sciences version 16, USA was used for descriptive analysis. Chi-squared test was used to derive P values for statistical significance. Results: A total of 1198 patients consisting of 52% females and 48% males were studied. The prevalence of VI and blindness was 28.2% and 3.7% respectively. Cataract, refractive error and glaucoma were the leading causes of VI while glaucoma and cataract caused the most cases of blindness. The age group most affected by VI was the 50-100 years group with 250 out of 338 cases and the same age group had the highest number of blind cases with 41 out of 44 cases. The number of females with VI and blindness was greater than that of the males. Conclusion: There is a high prevalence of VI and blindness especially among persons aged 50 years and above. Majority of the patients were visually impaired and blind due to treatable or preventable conditions. The study suggests that education, low-cost cataract surgical, and refractive services will reduce the rates of VI and blindness.
KEYWORDS
Visual Impairment and Blindness; Cataract; Glaucoma; Hospital-Based Study; Low-Cost Cataract Surgical; Refractive Services.
INTRODUCTION
Visual impairment (VI) is a global health problem which affects all aspects of life. It presents educational, occupational and social challenges, with the affected persons being at risk of behavioral, psychological, and poor social integration[1]. It does not only have significant effects on the lives of those affected but it also presents a large social and economic cost to the country [1, 2]. The World Health Organization (WHO) defines visual impairment (VI) as presenting visual acuity (PVA) that is worse than 6/18, but better and equal to 3/60 or a corresponding visual field (VF) loss of less than 20 degrees around the central fixation in the better eye with presenting optical correction if any[3]. Blindness is defined as PVA of worse than 3/60, or a corresponding VF loss of less than 10 degrees around the central fixation in the better eye with presenting optical correction if any [3]. Previously, estimates of VI were based on corrected vision, but in order to assess the magnitude of VI caused by uncorrected refractive errors (URE), estimates need to be based on presenting visual acuity [4, 5]. The estimated number of people visually impaired in the world is 285 million, of whom 39 million are blind. Age and gender affect VI and it has been reported that prevalence increases with age and women have a significantly higher risk of developing VI than men in every region of the world [3]. It is estimated that globally, up to 75% of all blindness is avoidable (either preventable or treatable) [6]. Without intervention, the number of blind people might reach 76 million by 2020 because of a number of factors, primarily the rapid aging of populations in most countries [1, 7]. The principal causes of VI globally are uncorrected refractive errors (URE) and cataracts, 43% and 33 % respectively. Other causes are glaucoma, 2%, age related macular degeneration (ARMD), diabetic retinopathy, trachoma and corneal opacities, all about 1%. A large proportion of causes, 18%, are undetermined. The causes of blindness are cataract, 51%, glaucoma, 8%, ARMD, 5%, childhood blindness and corneal opacities, 4%, uncorrected refractive errors and trachoma, 3%, and diabetic retinopathy 1%, the other causes are 21% [3]. There is inadequate data on the prevalence rate of VI and blindness in Ghana [8].The paucity of reliable information on this contributes to problems in designing and evaluating eye care services in Ghana. The purpose of this study is to provide useful information on the prevalence and causes of VI and blindness and their relationship with age and gender among patients who reported at the Juaben Hospital Eye Clinic.
MATERIALS AND METHOD
Study Area Juaben Hospital is one of the two primary government hospitals in the Ejisu-Juaben district, Ashanti, Ghana. According to the 2010 population and housing census, the municipal has a population of 143,762 (52.25% females and 47.75% males). The rural settlements accounts for 70% of the population while the urban centers take up 30% hence most of the patients using the hospital services are from the rural areas of the district[19]. Eye-care services at the hospital are provided by an ophthalmologist, an optometrist and ophthalmic nurses. Study Design The design was a retrospective study of patients who reported to the Juaben Hospital Eye Clinic from January 1, 2015 to June 30, 2015. Study Procedure All the patients registered and examined from January 2015 to June 2015 were included in the study; while patients who registered before and after the study period were excluded. Medical records of patients were retrieved from the hospital’s medical records department. Data from the medical records such as age, gender, visual acuity and diagnosis were noted. Names of patients were excluded from the data collection. The categorization of Visual Impairment and blindness in this study was based on the 10th revision of International statistical classification of diseases, injuries and causes of death as shown in (Table 1) [3]. In situations where there are multiple diagnoses, the disease which was easiest to manage was recorded as the primary cause of the Visual Impairment. A data sheet created with Microsoft excel 2010 was used to collect data from patients’ folders.
Table 1: Classifications of VI and Blindness.
| Visual Acuity | Classification |
| 6/6 – 6/18 | Normal vision |
| <6/18 – 6/60 | Moderate Visual Impairment (MVI) |
| <6/60 –3/60 | Severe Visual Impairment (SVI) |
| <3/60 | Blind |
Data Analysis The Statistical Package for Social Scientists (SPSS) version 16.2 (SPSS, Inc., Chicago, IL, USA) was used to analyze the data. Descriptive analysis and Chi-squared test were used to test for statistical significance; a p-value of < 0.05 was considered to be significant at 95% confidence interval.
ETHICAL CONSIDERATION Ethical clearance was obtained from the Ethical and Research Committee of Juaben Government Hospital. All data collected from the eye clinic medical records was not shared with anyone not involved in the study. Confidentiality of the information sought was ensured.
RESULTS
Social Demographics A total of 1198 case reports were included in this study comprising all the patients reporting to the Juaben Hospital Eye Clinic during the period of the study. 52% of the study population was women and 48% men. The age group most represented was 50-100 years at 43.7% followed by 15-49 years at 38.1% and the least was 0-14 years at 18.1%. The mean age was 42.83 with a standard deviation of 24.913. Table 2 and 3 shows the age and gender distribution of the study population.
Table 2: Distribution of the Study Population by Gender.
| Gender | Frequency | Percentage |
| Male | 575 | 48 |
| Female | 623 | 52 |
| Total | 1198 | 100 |
Table 3: Distribution of the Study Population by Age groups.
| Age group(years) | Frequency | Percentage |
|---|---|---|
| 0-14 | 217 | 18.1 |
| 15-49 | 457 | 38.2 |
| 50-100 | 524 | 43.7 |
| Total | 1198 | 100 |
Prevalence of Visual Impairment and Blindness The prevalence of VI and blindness in this study was 28.2% and 3.7% respectively. The study showed that 68.1% had normal vision, 23.8% had moderate visual impairment (MVI) and 4.4% had severe visual impairment (SVI). This is illustrated in table 4.
Table 4: Distributions of Visual Impairment and Blindness by Categories.
| Visual Impairment Category | Frequency | Percentage |
|---|---|---|
| Normal | 816 | 68.1 |
| Moderate visual Impairment | 285 | 23.8 |
| Severe visual impairment | 53 | 4.4 |
| Blind | 44 | 3.7 |
| Total | 1198 | 100 |
Cataract was found to be the leading cause of VI with 132 patients (39.05%). The other causes of VI included; uncorrected refractive errors 74 patients (21.60%), glaucoma 62 patients (18.34%), diabetic retinopathy 18 patients (5.33%), other retina diseases 14 patients (4.73%), age related macular degeneration(ARMD) 8 patients (2.37%), cornea diseases 8 patients (2.37%),hypertensive retinopathy 8 patients (2.37%), optic neuropathy 5 patients (1.48%), pan uveitis 5 patients (1.48%) and others 4 patients(1.18%). the causes of blindness were glaucoma 29 patients (65.91%), cataract 10 patients (22.73%), ARMD 2 patients (4.55%) and other retinal disease 2 patients (4.55%). The results showed more females were visually impaired and blind than the males. 54% of the visually impaired were females (150 MVI and 33 SVI) while 46% were males (135 MVI and 20 SVI) and the difference was statistically significant (p=0.03). The number of females who fell in the blind category was 24 against 20 blind males. The difference was statistically significant (p = 0.04). (Figure 1) illustrates the distribution of VI and blindness by gender.
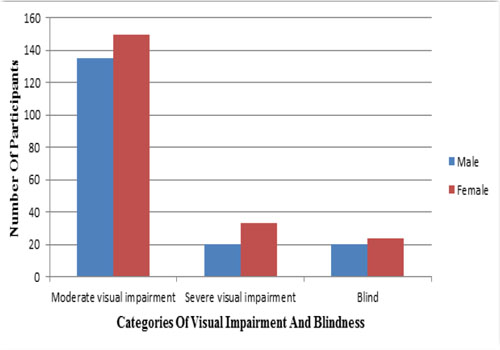
Figure 1: Frequency Distribution of Visual Impairment and Blindness by Gender.
The age group with the most VI case reports was 50-100 years with 250 patients (204 MVI and 46 SVI) then 15-49 years 75 patients (68 MVI and 7 SVI). The 0-14 year group was least affected with 13 patients all under MVI. The 50-100 years group had the most number of blind patients with a figure of 41 out of 44 blind patients followed by the 15-49 years group with 2 patients and least was the 0-14 group with 1 patient blind. The prevalence of VI and blindness appeared to increase with age and was statistically significant (p < 0.01).This is shown in (Figure 2).
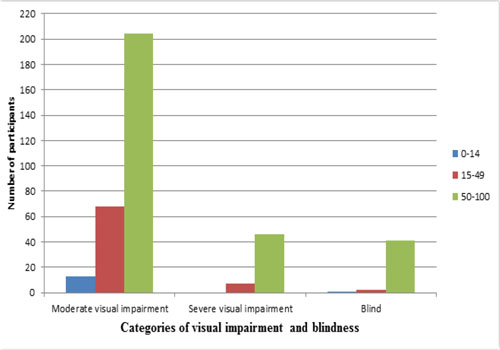
Figure 2: Frequency Distribution of Visual Impairment and Blindness by Age Group (years).
DISCUSSION
Demographic Characteristics of the Population The number of females (52%) was higher than that of the males (48%) in this study. Another Ghanaian study, the Tema Eye Survey also recorded a higher number of females (60.3%) than males(39.7%) [8]. Women are also adjudged to have a higher life expectancy than men [9]. This could result in the higher numbers of females than males. Persons aged 50 years and above made up 43.74% of the population followed by the 15-49 years group with 38.15% and the least was the 0-14 year group with 18.11% of the total. The higher number of persons aged 50 years and above can be as a result of the rapidly growing and expanding older population thus the increasing trend in life expectancy in developing countries [10].
Causes of Visual Impairment and Blindness Cataract, uncorrected refractive errors and glaucoma were found to be the leading causes of VI in this study. The major causes of blindness among the patients in the study were glaucoma (65.91%) and cataract (22.73%). This trend was consistent with the global estimates of VI and blindness [3, 11]. A comparable hospital-based study in Nigeria produced similar results with the major causes of VI being cataract and URE [12]. Similar findings were also seen in population-based studies conducted in Nigeria, South Africa and the Barbados [13-15]. Other studies have reported variable results. Studies in Kenya and Ethiopia reported cataract and cornea diseases as the main causes of blindness [14, 16, 17]. In Cameroon, Oye and Kuper found the major causes of blindness to be posterior segment diseases, followed by cataract and then optic atrophy. Cataract and URE were found to be the main causes of VI in the same study [18]. A population-based study done in Tehran reported URE, cataract and ARMD as the major causes of VI [19]. Another study in Brazil showed that URE caused the most cases of VI among the young while retinal disorders, cataract and Glaucoma caused the most blind cases [20]. In contrast to this study, results from the Beijing Eye Study presented cataract, degenerative myopia, glaucoma, cornea opacity and optic nerve damage as the main causes of VI and Blindness [21]. The differences in results among the various studies are probably due to differences in the definition of visual impairment and blindness, population’s characteristics, study area and methods. The results from this study show that the major causes of VI and blindness are treatable. Cataract accounted for the most visually impaired cases. This is probably because prevalence of cataract increases with age [22] and over 40% of the study population were over 50 years. The high numbers of uncorrected refractive error cases can also be attributed to inability to afford the service cost, especially those living in rural communities. Glaucoma and cataracts were the major cause of blindness in this study. Glaucoma can be treated if detected early [23]. The lack of awareness of Glaucoma may be the reason for the high rates. Also, the fear of surgery may also be responsible for most patients being blinded by cataract. Most people especially those in the rural areas have misconceptions about eye surgeries hence opt to avoid it totally.
Prevalence of Visual Impairment and Blindness The prevalence of VI and blindness in this study was 28.2% and 3.7% respectively. As compared to the population based survey on the prevalence of VI and Blindness which was done in Wenchi district with 2% VI and 1.7% blindness, this was very high [24]. A survey done in Tema came out with a result of prevalence of VI at 17.1% and blindness 1.2% [8]. In the National Blindness and VI survey in Nigeria the prevalence VI was 7.5% and that of blindness was 4.2% [13]. The reason for the higher prevalence of VI and blindness in this study compared to the above studies may be due to the differences in the definition of VI and blindness used in the various projects and the populations characteristics. Additionally, this study is hospital-based compared to those above, which were population-based. Hospital-based studies have been found to overestimate the occurrence and severity of diseases [25]. Factors such as level of education, inability to afford service cost, fear of the outcome of surgery and cultural beliefs are some of the barriers that prevent people from presenting for eye consultation and management of their eye problems resulting in high prevalence rates [14, 26].
Visual Impairment and Blindness: Association with Age and Gender Findings from this study showed that the prevalence of VI and Blindness increased with advancing age. Advancing age was found to have a positive association with VI and blindness. This was similar to the 2010 global estimates of prevalence of visual impairment [3]. Other surveys in Ghana, Nigeria and South Africa were consistent with this trend [8, 10, 13, 27, 28]. The reason for increase in the prevalence of VI and blindness with increasing age could be because most of the causes are age-related eye conditions. The number of females with visual impairment and blindness were also higher than the males in this study. Globally, females have been reported as having a significantly higher risk of visual impairment than males [3, 4]. This may be as a result of females’ relative longevity and lack of access to health care which is made preferentially accessible to males than females in some rural areas [29].
CONCLUSION
This study showed a high prevalence of VI and blindness. The major causes of VI and blindness were Cataract, URE and Glaucoma. This shows that most of the visually impaired and blind cases in this study were due to treatable or avoidable conditions. VI and Blindness were also seen to be higher in the elderly. There were also more females affected by VI and blindness than males.
LIMITATIONS
This is a hospital-based study therefore it is biased toward those seeking healthcare (eye-care services in this study); hence findings may be higher than would be seen in the population at large. Also, categorization of visual impairment and blindness are based on presenting, not corrected visual acuity. Another limitation was the scarcity of data on hospital-based studies in Ghana and other parts of Africa which led to the comparisons with population-based studies in the discussion. Socioeconomic differences may also influence prevalence and causes of visual impairment [27], hence should be taken into consideration when comparing these data with other studies.
RECOMMENDATIONS
It is recommended that treatment of cataracts and uncorrected refractive errors should be of top priority in order to reduce the high rates of VI. This can be done by introducing affordable services for optical correction of refractive errors and cheaper but effective cataract surgery procedures. With Glaucoma being the major cause of blindness and third most common cause of VI, it is necessary to develop programs that will help us detect Glaucoma in its early stages and manage appropriately. Frequent eye screening exercises and awareness creation must be encouraged in these rural and remote areas. It is also recommended that a population-based study be con-ducted to provide accurate data on the prevalence of VI and blindness in the entire country to get up to date figures which could help plan, evaluate and monitor the eye care services in Ghana.
REFERENCES
- Frick KD and Foster A. (2003). The magnitude and cost of global blindness: an increasing problem that can be alleviated. American journal of ophthalmology. 135(4): 471-476.
- Livingston P, McCarty C and Taylor H. (1997). Visual impairment and socioeconomic factors. British Journal of ophthalmology. 81(7): 574-577.
- Pascolini D and Mariotti SP. (2011). Global estimates of visual impairment: 2010. British Journal of Ophthalmology. 96(5): 614-618.
- Resnikoff S. (2004). Global data on visual impairment in the year 2002. Bulletin of the world health organization. 82(11): 844-851.
- Pascolini D. (2004). 2002 global update of available data on visual impairment: a compilation of population-based prevalence studies. Ophthalmic epidemiology. 11(2): 67-115.
- Foster A, Gilbert C and Johnson G. (2008). Changing patterns in global blindness: 1988-2008. Community eye health/International Centre for Eye Health. 21(67): 37-39.
- Pizzarello L. (2004). VISION 2020: The Right to Sight: a global initiative to eliminate avoidable blindness. Archives of ophthalmology. 122(4): 615-620.
- Budenz DL. (2012). Blindness and visual impairment in an urban West African population: the Tema Eye Survey. Ophthalmology. 119(9): 1744-1753.
- Salomon JA. (2013). Healthy life expectancy for 187 countries, 1990-2010: a systematic analysis for the Global Burden Disease Study 2010. The Lancet. 380(9859): 2144-2162.
- Kinsella KG and Phillips DR. (2005). Global aging: The challenge of success. Population Reference Bureau Washington, DC.
- Resnikoff S and Pararajasegaram R. (2001). Blindness prevention programmes: past, present, and future. Bulletin of the World Health Organization. 79(3): 222-226.
- Malu K. (2013). Blindness and visual impairment in north central Nigeria: a hospital based study. The Nigerian postgraduate medical journal. 20(2): 98-103.
- Dineen B. (2008). The Nigerian national blindness and visual impairment survey: Rationale, objectives and detailed methodology. BMC ophthalmology. 8(1): 17.
- Oduntan A. (2005). Prevalence and causes of low vision and blindness worldwide. African Vision and Eye Health. 64(2): 44-57.
- Hyman L. (2007). Prevalence and causes of visual impairment in the Barbados Eye Study. Ophthalmology. 108(10): 1751-1756.
- Mathenge W. (2007). Rapid assessment of avoidable blindness in Nakuru district, Kenya. Ophthalmology. 114(3): 599-605.
- Berhane Y. (2007). Prevalence and causes of blindness and low vision in Ethiopia. Ethiopian Journal of Health Development. 21(3): 204-210.
- Oye JE and Kuper H. (2007). Prevalence and causes of blindness and visual impairment in Limbe urban area, South West Province, Cameroon. British Journal of Ophthalmology. 91(11): 1435-1439.
- Fotouhi A. (2004). The prevalence and causes of visual impairment in Tehran: the Tehran Eye Study. British journal of ophthalmology. 88(6): 740-745.
- Salomão SR, Mitsuhiro MR and Belfort R. (2009). Visual impairment and blindness: an overview of prevalence and causes in Brazil. Anais da Academia Brasileira de Ciências. 81(3): 539-549.
- Xu L. (2006). Causes of blindness and visual impairment in urban and rural areas in Beijing: the Beijing Eye Study. Ophthalmology. 113(7): 1134.
- Brian G and H Taylor. (2001). Cataract blindness: challenges for the 21st century. Bulletin of the World Health Organization. 79(3): 249-256.
- Weinreb RN and Khaw PT. (2004). Primary open-angle glaucoma. The Lancet. 363(9422): 1711-1720.
- Moll A, van der Linden AJ, Hogeweg M, Schader WE, et al. (1994). Prevalence of blindness and low vision of people over 30 years in the Wenchi district, Ghana, in relation to eye care programmes. British journal of ophthalmology. 78(4): 275-279.
- Goldberg RJ, McManus DD and Allison J. (2013). Greater knowledge and appreciation of commonly-used research study designs. The American journal of medicine. 126(2): e1-8.
- Sacharowitz H. (2005). Visual impairment in South Africa: achieve-ments and challenges. African Vision and Eye Health. 64(4): 139-149.
- Cockburn N, David Steven, Karin Lecuona, Francois Joubert, et al. (2012). Prevalence, causes and socio-economic determinants of vision loss in Cape Town, South Africa. PloS one. 7(2): e30718.
- Guzek JP, Anyomi FK, Fiadoyor S and Nyonator F. (2005). Prevalence of blindness in people over 40 years in the Volta region of Ghana. Ghana medical journal. 39(2): 55-62.
- Shahriari H.-A, Izadi S, Rouhani MR, Ghasemzadeh F, et al. (2007). Prevalence and causes of visual impairment and blindness in Sistan-va-Baluchestan Province, Iran: Zahedan Eye Study. British journal of ophthalmology. 91(5): 579-584.