Information Links
Related Conferences
Previous Issues Volume 10, Issue 1 - 2025
Pathogenesis of Infantile Colic. Hypothesis
Michael D Levin*
Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus, Dorot. Medical Center for Rehabilitation and Geriatrics, Amnon veTamar, Netanya, Israel
*Corresponding author: Dr. Michael Levin, Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus, Dorot. Medical Center for Rehabilitation and Geriatrics, Amnon veTamar, Netanya, Israel, Tel: 972-538281393, E-mails: [email protected]; [email protected]
Received Date: April 06, 2025
Published Date: April 23, 2025
Citation: Levin M. (2025). Pathogenesis of Infantile Colic. Hypothesis. Mathews J Gastroenterol Hepatol. 10(1):29.
Copyrights: Levin M. © (2025).
ABSTRACT
Infantile colic syndrome describes a restless infant whose symptoms of severe pain begin at 2-3 weeks, peak at 5-8 weeks, and stop spontaneously at 4-6 months. The etiology and pathogenesis of the disease are unknown. There is no reliable evidence of symptom reduction under the influence of various treatment methods. Based on the literature analysis and our own research, a hypothesis of the etiology and pathogenesis of infantile colic is proposed. It develops in children with genetically determined lactose intolerance if full breastfeeding is interrupted before the cessation of functional regurgitation. The volume of sucked milk exceeds the capacity of the stomach. In such cases, the infant pours out excess milk. This contributes to the distension of the stomach. If the infant begins to receive food that requires treatment with hydrochloric acid, a change in the program occurs and along with the release of acid, a tenfold reduction in lactase formation occurs. Unhydrolyzed lactose causes the release of histamine from the mast cells of the small intestine, which leads to hypersecretion of hydrochloric acid. The child is restless because during regurgitation, hydrochloric acid causes painful reactions. This stops as soon as the capacity of the stomach corresponds to the volume of food eaten. In calm infants, the amount of lactase does not change after stopping breastfeeding. Stopping infant colic does not mean recovery, since the function of the LES is damaged during colic. In addition, lactose intolerance remains for life.
Keywords: Infantile Colic, Lactose Intolerance, Gastroesophageal Reflux Disease, Stomach Physiology in Infants, Lower Esophageal Sphincter Physiology, pH Monitoring, pH Impedance.
INTRODUCTION
The life and development of a newborn depends on the consumption of milk, which contains everything necessary for this purpose. The painful behavior of an infant 2 weeks after birth is associated with its nutrition, and there is reason to believe that colic occurs in those of them who have lactose intolerance.
LACTOSE INTOLERANCE
Modern concepts
The newborn receives mother's milk, which has everything necessary for its development and rapid growth. It contains protein and lactose. Lactose is a disaccharide sugar that is digested into glucose and galactose by the enzyme lactase, produced in the brush border mucosa of the small intestine. In all mammals, lactase concentrations are at their highest shortly after birth and decline rapidly after the usual age of weaning. In some children, lactase secretion remains high after weaning. In other cases, the transition to regular food, which requires processing with acid, the amount of lactase decreases to 10% of its initial level. The percentage of genetically determined primary lactase deficiency varies among different peoples. For example, among the Irish it is about 4%, among the peoples of northern Europe - 20%, among Ashkenazi Jews - 70%, and among the Chinese - 98% [1-3].
Since lactase levels decline from a peak at birth to less than 10% after weaning, this leads to lactose malabsorption. It is believed that unhydrolyzed lactose may be fermented in the colon by bacteria, which leads to the production of carbon dioxide, hydrogen, methane, proprionic and butyric acids (short-chain fatty acids). Fermentation ingredients and gas is the pathophysiological mechanism causing symptoms such as abdominal pain, cramps, borborygmi, bloating and flatulence, watery and acid diarrhea, nausea, and vomiting [4,5].
Literature analysis
This description of the pathogenesis of lactose intolerance contains two hypotheses. The first hypothesis is assumed that lactase is fermented in the colon by bacteria to form carbon dioxide, hydrogen, methane, proprionic and butyric acids. The second states that symptoms occur because of lactose fermentation by bacteria in the colon. The first hypothesis is confirmed by the increase in expired hydrogen and methane during the lactose breath test [4-6]. The second contradicts the clinical picture. Infants react to pain with anxiety, so it is impossible to assess their symptoms and the time of their appearance. In adult patients with lactose intolerance, in the presence of cardia dehiscence, when the contents of the stomach enter the esophagus immediately after eating, heartburn appears 15-30 minutes after drinking even a small amount of milk in a cup of coffee. Since the contents of the stomach enter the large intestine no earlier than 4.2 hours later [7], and lactose fermentation occurs gradually during slow movement through the large intestine, therefore, the appearance of heartburn after 15-30 minutes occurs under the action of another mechanism. Deng et al. found in adults that with “true positive” lactose intolerance complains of symptoms only after the substrate has entered the colon (usually 50–100 min). The difference in the time of symptom onset depends on the degree of damage to the LES. With complete failure of the LES (chalasia of EGJ) (Figure 1a & 1b), gastric chyme enters the esophagus immediately after lactose ingestion. This means that excess acid occurs in the stomach after 15–30 minutes. If the function of the LES is weakened to a lesser extent and it opens sometime after lactose ingestion, the patient does not associate the occurrence of heartburn with lactose ingestion. Figure 1d shows an X-ray of a patient after the Nissen fundoplication. The patient suffered from frequent severe heartburn, despite taking PPI. Heartburn temporarily disappeared only after drinking milk, since milk, being a base, neutralized the acid. After she stopped drinking milk, heartburn became rare and short-lived [8].
.png)
Figure 1. Esophageal radiographs are taken at high gastric pressure. Red arrows indicate the LES, yellow arrows indicate the proximal sphincter, which proximally closes the phrenic ampulla (p); white arrows indicate the aortic sphincter, which occurs because of acid retention in esophageal constriction at the level of the aortic arch. (a). At high pressure, the contracted LES does not close the EGJ. (b). The same patient. After 5 minutes of resting, free reflux is determined. The LES is shortened, and the hiatal orifice is dilated. Due to chalasia of EGJ, the patient feels heartburn as soon as acid appears in the stomach. (c). A patient with severe esophagitis with only extraesophageal symptoms. The length of the LES is more than 2 times shorter than the minimal normal limit. He wakes up at night because he chokes on saliva. This is due to the contraction of the aortic sphincter. After he swallowed a dense tablet with a diameter of 1.9 cm, almost all symptoms disappeared. The absence of pain syndrome indicates damage to the sensitive elements in the wall of the esophagus. (d). S-shaped esophagus in an elderly woman after Nissen fundoplication. The esophageal dilation has developed over the overly compressed LES. The red arrow shows the narrowing, which is mistakenly called the LES, displaced into the chest cavity. This is the proximal sphincter, the contraction of which closes the lumen of the phrenic ampulla proximally to create a high pressure in it, exceeding the pressure in the stomach. The long rigid antral gastritis (g) shows that hypersecretion of hydrochloric acid is not only a problem of the esophagus.
Secondly, heartburn is a reaction of the esophagus, not the large intestine. Such a rapid response to lactose intake indicates the presence of a humoral provocateur of hydrochloric acid hypersecretion. Recently, Aguilera-Lizarraga et al showed that injection of "food antigens (gluten, wheat, soy and milk) into the rectosigmoid mucosa of patients with irritable bowel syndrome induced local oedema and mast cell activation" [9]. It is known that mast cell activation leads to the release of histamine, and the histamine directly or through stimulation of gastrin secretion causes the release of hydrochloric acid. Thus, both lactose and other foods can cause the release of histamine from mast cells, like what occurs in allergies. I consider lactose to be the main cause of hypersecretion of hydrochloric acid, since in most patients with GER, in whom taking PPIs did not relieve symptoms, stopping the use of lactose-containing products led to significant improvement, even in cases where patients were unaware of milk intolerance.
An analysis of the literature shows that many assumptions are published that have no evidence. Some of them contradict reliable scientific facts. Our task is to isolate reliable data from the general mass of information that can be relied upon in scientific research.
INFANTILE COLIC
Modern concepts
It is believed that infantile colic is observed in 10–30% of infants, in which a healthy infant suffers from paroxysms of excessive, high-pitched, inconsolable crying, frequently accompanied by flushing of the face, meteorism, drawing-up of the legs and the passing of gas [10]. This syndrome is presented typically in the second or third week after birth, and peaks at 5 to 8 weeks of age; it usually resolves spontaneously by 4 months of age. As can be seen, none of these symptoms match those described in lactose metabolism in the colon. First, farting during straining is a common occurrence in newborns and cannot serve as evidence of excessive gas formation. Second, any statistical studies on the reduction of infant fussiness in response to treatment must consider that the strength and frequency of the pain syndrome varies over time in a sinusoidal pattern. To this day, some doctors consider these babies healthy on the grounds that the disease supposedly disappears without a trace by 6 months. The imperative for healthcare professionals is to reduce parental anxiety by offering reassurance and support [11].
Literature analysis
A. 10 years after the disappearance of colic, Savino et al. discovered pain and allergic disorders in these patients. Sleep disorders, fussiness, aggressiveness and feelings of supremacy are more frequent in children who suffer from colic during early infancy. The family history of gastrointestinal diseases and atopic diseases was significantly higher in infants with colic than in controls [12]. In other study the history of infantile colic, regurgitation, and functional constipation was detected respectively in 26.41, 25.31, and 30.16% of children diagnosed with functional gastrointestinal diseases compared to 11.34, 12.85, and 11.76% of healthy children [13]. Consequently, infantile colic is a serious disease that leads to remote pathological consequences. To avoid them, it is necessary to treat not the symptoms, but the disease. To do this, it is necessary to establish the etiology and pathogenesis of infantile colic.
B. Howard et al. in adjusted analyses "found that a diagnosis of colic predicted shorter full breastfeeding duration" [14]. This dependence is a generally accepted fact [15]. It is stated that lactase levels decline from peak at birth to less than 10% of pre-weaning infantile level in childhood [4].
I have not found a study that has determined a 10-fold decrease in lactase after stopping full breastfeeding. However, from the point of view of mammalian physiology, it seems likely. Obviously, after stopping breastfeeding in healthy animals, lactase secretion decreases sharply, since there is no need for it. In infants, while they are breastfed, the amount of lactase is sufficient to neutralize lactose, and this prevents the secretion of hydrochloric acid. If the transition to a replacement diet occurs too early, then in some cases this has no consequences, since genetic protection has appeared that does not reduce the amount of lactase. This is supported by statistical data. In Ireland, where dairy products have been consumed for many centuries, the prevalence of lactose intolerance is low, with approximately 4-5% of the population affected. Meanwhile, in China, where dairy products have only recently been used, the prevalence of lactose intolerance reaches 93%. In infants with lactose intolerance, there is a sharp reduction in the secretion of lactase after switching to a diet that requires treatment with hydrochloric acid [4]. Unsplit lactose affects the mast cells of the small intestine, which leads to the release of histamine, which itself or through the secretion of gastrin causes the secretion of hydrochloric acid in the stomach [9]. In such cases, if the mother is unable to breastfeed, the practice of using a wet nurse saves the infant from colic.
C. Kahn et al, using polygraphy discovered sleep normalized after milk was withdrawn, deteriorated after a challenge with milk, and normalized again on a second trial of milk elimination [16]. Rybak et al. have shown that in infants, several factors contribute to exacerbating colic, including a liquid milk-based diet [17]. These data support the role of milk as a trigger for infant colic.
D. Heine, using pH monitoring in infantile colic, found pathological acid exposure time (>10%) in 17.9% of infants, but found no relationship with total crying duration [18]. Similar results have been reported by other authors [19,20]. For example, Salvatore et al. found that a pathologic pH study (reflux index > 10%) was found in 21 of 100 (21%) infants. Esophagitis was present in 17 of 44 (39%). 38% of infants with a pathologic pH study had a normal esophageal biopsy and 53% of infants with histologic esophagitis had a normal pH study [19].
Comparison of these results irrefutably demonstrates that (1) all children with infantile colic have acid reflux into the esophagus; (2) the results of pH monitoring are less reliable than endoscopic detection of esophagitis and histological signs of inflammation in it. At the same time, it is known that endoscopy and conventional histological examination have low reliability; (3) the statement that the presence of acid with a reflux index < 10% is normal (2.4 hours over 24 hours) has not been proven anywhere and is absurd from the physiological point of view; (4) the statement that only 24-h impedance-pH monitoring can accurately diagnose GERD is an error that has no scientific basis, and serves only as advertising of diagnostic equipment.
E. In the article by Blank M-L et al The authors concluded that "the appropriateness of PPI treatment should be questioned, as the majority of infants who received these drugs were not diagnosed with severe GERD" [18]. Another feature of infantile colic with confirmed GERD is the lack of effect of PPI on irritability, despite significantly reduced esophageal acid exposure [21-23].
The idea that healthy people may have physiological GER is a grossmistake. Babies suffer pain because acid damages the esophageal mucosa, regardless of its quantity. Therefore, reducing the residence time of acid to less than 10% under the influence of PPI does not significantly change the clinical picture. The recommendations of these authors are contrary to common sense, because if PPI "significantly reduced esophageal acid exposure", then they are a pathogenetic treatment that reduces the degree of damage to the esophagus. Secondly, it is known that symptoms are not always proportional to the pathophysiology of the process. Therefore, the goal is to treat disease, not the symptoms [17,18].
F. In an independent systematic review, the quality of the evidence in studies of the effect of dietary modification on the duration of restlessness in children was assessed as very low [24]. The most frequently published articles are about the benefits of probiotics. For example, in the article by Maldonado-Lobón et al. with PROBI-COLIC group, two groups of patients with infantile colic were compared. One group received simethicone, and the other probiotics. In both groups, crying times significantly decreased over 28 days. However, the percentage of reduction in the minutes of crying from baseline was significantly higher in the probiotics group [25]. The authors' conclusion that probiotic is safe and effective treatment for infantile colic is erroneous, since it is known that crying episodes tend to increase at 6 weeks and usually resolve spontaneously by the age of 3 - 6 months [10,25]. Thus, the reduction in symptoms is due not to treatment, but to the natural course of the disease. Ong et al. found that there is no clear evidence that probiotics are more effective than placebo at preventing infantile colic [26]. The one proven treatment is time, as this behavior tends to dissipate by 6 months of age [27]. This applies to other treatments. For example, Ahmed et al. found that the use of lactase was associated with a significant reduction in excessive crying compared with the placebo group (p < 0.05) [28]. This article cannot be considered scientific due to a conflict of interest, as the authors received "Funding Sources: RG Pharmaceutica (Pvt) Ltd" [28].
Conclusion
Literature analysis convincingly proves that infants with colic suffer from reflux of hydrochloric acid into the esophagus. These children, unlike calm infants, interrupted full breastfeeding and, since they had a need to treat food with hydrochloric acid, a change in the program occurred. Along with the release of hydrochloric acid, there is a sharp, tenfold decrease in the secretion of lactase. Therefore, the use of any dairy product containing lactose leads to the release of histamine from mast cells of the small intestine. Histamine and gastrin, the secretion of which it stimulates, lead to hypersecretion of hydrochloric acid. Reflux of acid into the esophagus causes infantile colic. It has also been shown that the use of pH monitoring has no diagnostic value, because the development of these studies is based on gross methodological violations. Numerous articles recommending their use are advertising for their manufacturers. The use of various treatment methods with an erroneous idea of the etiology and pathogenesis of the disease does not help patients. They are advertised by order of the manufacturers. Infantile colic occurs in babies with genetically determined lactose intolerance. In other babies, stopping full breastfeeding does not change the amount of lactase secreted, so they do not suffer from colic and GERD.
MY STUDIES OF INFANTILE COLIC PATHOGENESIS
Why does infant colic come and go at certain times?
A baby is born with a small stomach. It quickly gains weight because it sucks from 600 ml per day in the first month to a liter of milk in the fifth month. The shape of the stomach in a newborn resembles a retort. Gastric distention begins from the fundus and body of the stomach between the LES and the narrow antral part. In this case, the body of the stomach is located above the bulb of the duodenum. When the antral section expands, the stomach sags below the bulb (Figure 2). The stomach enlarges due to the large volumes of milk consumed. The baby burps up excess milk. If there is no acid in the stomach, it is calm. If acid appears, it causes damage to the esophagus, which is accompanied by pain. That is why the baby cries.
.png)
Figure 2. Barium X-ray of the stomach in patients with GERD. (b,c,d,e). Stages of gastric distension in infants.
When the stomach capacity reaches the volume of one feeding, the child stops regurgitating, the acid does not enter the esophagus and does not cause pain. But the child does not recover. Firstly, lactose intolerance, which causes hypersecretion of hydrochloric acid, remains for life. Secondly, the effect of acid on the LES during infantile colic leads to weakening of the LES. Thirdly, hypersecretion of hydrochloric acid causes damages not only to the LES and esophagus, but to the entire digestive tract, to a greater extent its upper section, including the stomach, duodenum and bile ducts.
I analyzed the state of the digestive tract of three generations of an Ashkenazi Jews family (Figure 3).
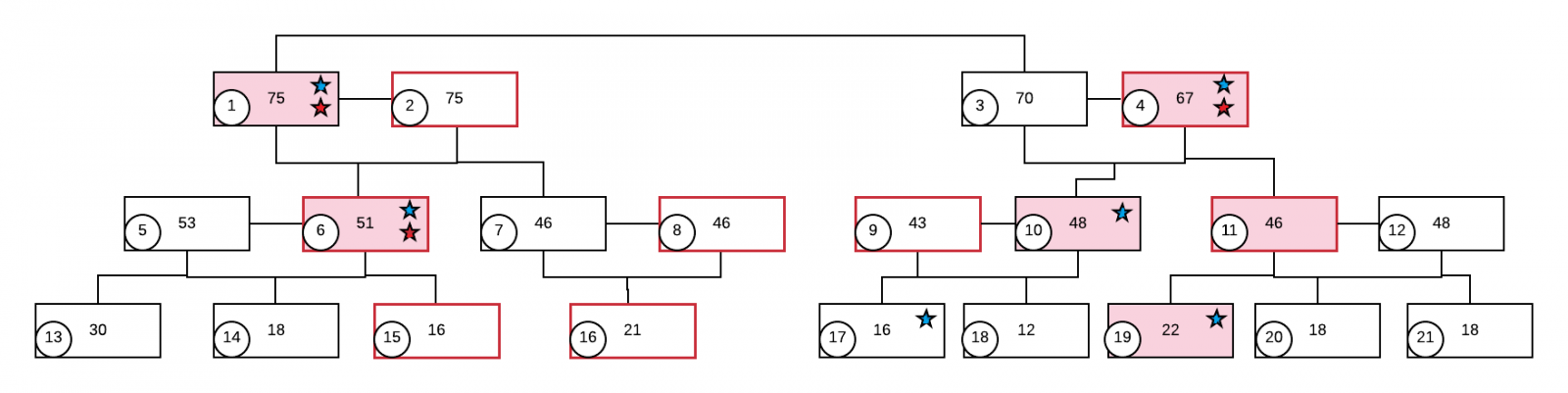
Figure 3. Three generations of a family, each member of which has his own number in the circle. Women - in a red frame. In the center of the square shows the age. A pink color indicates family members with a clear clinical picture of GERD. The blue asterisk is milk intolerance. The red star is a restless baby.
In patients older than 40 years with severe GERD and lactose intolerance, three interesting factors were found. (a) These patients were restless children in infancy. And those of their relatives who did not turn to gastroenterologists were calm babies. (b) Patients with GERD for many years after a troubled period in the first six months of life and before the onset of symptoms of GERD considered themselves healthy and consumed dairy products without any sensations. (c) The number of lactose-containing foods that provoked abdominal pain and/or heartburn decreased progressively with age. In some cases, it was enough to use a small amount of milk in coffee or a jar of yoghurt to suffer from severe heartburn or pressing chest pain.
These results are consistent with those of El-Serag et al., who performed a statistical analysis of the primary diagnosis of GERD. “Previous diagnoses of coronary artery disease, peptic ulcer disease, nonspecific chest pain, nonspecific abdominal pain, chronic obstructive pulmonary disease, and asthma were associated with a subsequent new diagnosis of GERD. A first diagnosis of GERD was associated with an increased risk of a subsequent diagnosis of esophageal adenocarcinoma, esophageal stricture, chronic cough, sinusitis, chest pain, angina, gallbladder disease, irritable bowel syndrome, or sleep problems” [29]. Figure 4 shows the incidence of primary diagnosis of GERD according to age.
.png)
Figure 4. Incidence of gastroesophageal reflux disease diagnosis in UK general practice [29].
All studies show that the sharp increase in the diagnosis of GERD with age can be explained by an increase in detection, because of the appearance of typical and disturbing symptoms. It once again confirms that GERD can proceed and progress for a long time without symptoms. Its picture can be obscured by symptoms of damage to the stomach, duodenum and bile ducts, since they, like the esophagus, are damaged by hydrochloric acid. The above studies indicate that over time, the sensitivity of the esophagus decreases compared to the initial stage of the disease. This can only be explained by damage to the sensitive elements in the esophageal wall by the refluxant. For example, a sharp increase in esophageal erosion after POEM is not always accompanied by pain. The manifestation of GERD only by non-esophageal symptoms also indicates a decrease in pain sensitivity. Therefore, disturbing heartburn in the initial stage of the disease is a convincing symptom of GERD, and not a hypersensitive esophagus. Erroneous diagnosis of functional diseases instead of GERD is caused using pH monitoring and pH impedance, which should not be used due to the low reliability of the results.
Why are short episodes of reflux after regurgitation accompanied by prolonged anxiety?
The pathophysiology of GERD is characterized by mucosal edema and spasm of the LES, which increase proportionally to the time of acid exposure. The LES becomes rigid, which is manifested by weak contraction and weak relaxation. Peristalsis of the esophagus is impaired under the influence of acid. Its width increases. These changes increase by 5-8 weeks of life and are accompanied by increasing anxiety. Based on these assumptions; to eliminate the rigidity of the LES, we performed a dilation of the EGJ. For this, a Foley catheter was inserted into the stomach using a guide string. In the stomach, the catheter balloon was inflated to a diameter of 1-2 cm, after which the catheter was pulled out without hindrance. Studies were conducted in children with GERD under the age of one year, including infants with colic. A manometric study was performed before and immediately after this procedure. A significant increase in the tone of the LES and an increase in its response to stimulation compared to the values before the expansion of the LES was found. Stretching of the EGJ caused an obvious reduction in clinical symptoms of GERD. In most infants, a single stretch of the EGJ resulted in complete cessation of colic [30]. Shafik et al performed stretching of the LES in healthy volunteers. Lower esophageal sphincter balloon distension with 2 mL of saline produced esophageal pressure increase to a mean of 34.2 ± 5.3 cm H₂O (p < 0.001). They suggested that the lower esophageal sphincter dilatation initiates increased esophageal peristalsis, which clears the esophagus of the refluxed acid [31].
This method of LES distension is much simpler than pneumodilations or esophagomyotomy with fundoplication, which are used in case of erroneous diagnosis of esophageal achalasia (EA). In the analysis of 29 cases of EA in children and adolescents published in the literature, where radiographic examination was presented, only in one case the clinical and radiographic picture corresponded to EA. In 23 patients the radiographic picture corresponded to gastroesophageal reflux disease, including in 4 patients after high resolution manometry (HRM), which determined the diagnosis of EA. In 3 patients there was congenital stenosis of the esophagus and/or LES. In 2 cases the exact diagnosis could not be established. EGJ dissection was performed in 19 patients with GERD, and pneumodilations in 3 patients [32]. Temporary reduction of GERD symptoms was assessed as a positive effect of treatment. However, transection of an already weakened LES is always accompanied by transection of the esophagus above it and the stomach below the LES. Fundoplication only temporarily prevents reflux, while transection of the esophagus often leads to the development of a false diverticulum in which acid is retained, leading to the resumption of GERD symptoms [32].
Based on the above studies, it can be assumed that damage to the LES and esophagus by hydrochloric acid leads to impaired esophageal clearance of refluxant that entered the esophagus during regurgitation. Acid retention in the esophagus above the LES causes prolonged irritation and pain, which manifests as colic. The cessation of the child's restlessness after a single stretch of the EGJ is probably due to improved esophageal clearance. These studies explain why episodes of reflux do not coincide in time with intestinal colic.
CONCLUSION
Infantile colic occurs mainly in children with genetic lactose intolerance if full breastfeeding is stopped before functional regurgitation ceases. From the moment the child begins to receive food that requires its processing with hydrochloric acid, a change in the program occurs. The secretion of hydrochloric acid is accompanied by a 10-fold decrease in the secretion of lactase. As a result, a significant amount of unhydrolyzed lactose causes the release of histamine from mast cells of the small intestine, which leads to hypersecretion of hydrochloric acid. For 4-6 months, regurgitation is since the child sucks out volumes of milk that exceed the capacity of the stomach. This mechanism ensures rapid stretching of the stomach. Regurgitation of excess food is a physiological necessity. If acid gets into the esophagus, this causes a painful reaction in the child, regardless of the pH of the gastric juice. In this case, both the mucous membrane of the esophagus and the function of the LES are damaged. Acid thrown into the esophagus during regurgitation is retained in the esophagus due to the impaired function of the LES and esophagus. This explains the prolonged restlessness after a single regurgitation. Balloon dilation of the LES can stop infantile colic. By 4-6 months of age, the stomach capacity corresponds to a single meal. By this time, the acid from the stomach stops flowing into the esophagus, which leads to the cessation of colic. This is how most people begin to experience gastroesophageal reflux (GER), which, regardless of the presence of symptoms, is a disease that requires treatment.
The disappearance of colic does not mean recovery. First, lactose intolerance remains for the rest of life. Second, damage to the LES function during the first months of life causes GERD symptoms in many children for several years: the child is restless, wakes up at night and calms down only after drinking liquid that washes away the acid from the esophagus. A wet spot appears on the pillow due to regurgitation. Anemia often occurs. Bad breath may appear. Subsequently, for many years, this person feels healthy. But GERD progresses without pronounced symptoms, because the acid damages sensitive elements in the wall of the esophagus.
The use of pH monitoring and pH impedance is meaningless because, firstly, the diagnosis is clear based on knowledge of etiology and pathogenesis. Secondly, due to methodological errors in their development, these methods diagnose only very severe cases of GERD. Because of this, more than 30% of patients did not receive pathogenetic treatment.
ACKNOWLEDGEMENTS
None.
CONFLICTS OF INTEREST
The author declares that there are no conflicts of interest.
REFERENCES
- Bhatnagar S, Aggarwal R. (2007). Lactose intolerance. BMJ. 334(7608):1331-1332.
- Camilleri M, Park SY, Scarpato E, Staiano A. (2017). Exploring hypotheses and rationale for causes of infantile colic. Neurogastroenterol Motil. 29(2).
- Zeevenhooven J, Koppen IJN, Benninga MA. (2017). The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers Pediatr Gastroenterol Hepatol Nutr. 20(1):1-13.
- Vandenplas Y. (2015). Lactose intolerance. Asia Pac J Clin Nutr. 24(Suppl 1):S9-S13.
- Rana SV, Malik A. (2014). Hydrogen breath tests in gastrointestinal diseases. Indian J Clin Biochem. 29(4):398-405.
- Newcomer AD, McGill DB, Thomas PJ, Hofmann AF. (1975). Prospective comparison of indirect methods for detecting lactase deficiency. N Engl J Med. 293(24):1232-1236.
- Roland BC, Ciarleglio MM, Clarke JO, Semler JR, Tomakin E, Mullin GE, et al. (2015). Small Intestinal Transit Time Is Delayed in Small Intestinal Bacterial Overgrowth. J Clin Gastroenterol. 49(7):571-576.
- Deng Y, Misselwitz B, Dai N, Fox M. (2015). Lactose Intolerance in Adults: Biological Mechanism and Dietary Management. Nutrients. 7(9):8020-8035.
- Aguilera-Lizarraga J, Florens MV, Viola MF, Jain P, Decraecker L, Appeltans I, et al. (2021). Local immune response to food antigens drives meal-induced abdominal pain. Nature. 590(7844):151-156.
- Savino F. (2007). Focus on infantile colic. Acta Paediatr. 96(9):1259-1264.
- Scott-Jupp R. (2018). Why do babies cry? Arch Dis Child. 103(11):1077-1079.
- Savino F, Castagno E, Bretto R, Brondello C, Palumeri E, Oggero R. (2005). A prospective 10-year study on children who had severe infantile colic. Acta Paediatr Suppl. 94(449):129-132.
- Indrio F, Di Mauro A, Riezzo G, Cavallo L, Francavilla R. (2015). Infantile colic, regurgitation, and constipation: an early traumatic insult in the development of functional gastrointestinal disorders in children? Eur J Pediatr. 174(6):841-842.
- Howard CR, Lanphear N, Lanphear BP, Eberly S, Lawrence RA. (2006). Parental responses to infant crying and colic: the effect on breastfeeding duration. Breastfeed Med. 1(3):146-155.
- Sommermeyer H, Krauss H, Chęcińska-Maciejewska Z, Pszczola M, Piątek J. (2020). Infantile Colic-The Perspective of German and Polish Pediatricians in 2020. Int J Environ Res Public Health. 17(19):7011.
- Kahn A, François G, Sottiaux M, Rebuffat E, Nduwimana M, Mozin MJ, et al. (1988). Sleep characteristics in milk-intolerant infants. Sleep. 11(3):291-297.
- Rybak A, Pesce M, Thapar N, Borrelli O. (2017). Gastro-Esophageal Reflux in Children. Int J Mol Sci. 18(8):1671.
- Heine RG, Jordan B, Lubitz L, Meehan M, Catto-Smith AG. (2006). Clinical predictors of pathological gastro-oesophageal reflux in infants with persistent distress. J Paediatr Child Health. 42(3):134-139.
- Salvatore S, Agosti M, Baldassarre ME, D'Auria E, Pensabene L, Nosetti L, et al. (2021). Cow's Milk Allergy or Gastroesophageal Reflux Disease-Can We Solve the Dilemma in Infants? Nutrients. 13(2):297.
- Salvatore S, Hauser B, Vandemaele K, Novario R, Vandenplas Y. (2005). Gastroesophageal reflux disease in infants: how much is predictable with questionnaires, pH-metry, endoscopy and histology? J Pediatr Gastroenterol Nutr. 40(2):210-215.
- Blank M-L, Parkin L. (2017). National Study of Off-label Proton Pump Inhibitor Use Among New Zealand Infants in the First Year of Life (2005-2012). J Pediatr Gastroenterol Nutr. 65(2):179-184.
- Gieruszczak-Białek D, Konarska Z, Skórka A, Vandenplas Y, Szajewska H. (2015). No effect of proton pump inhibitors on crying and irritability in infants: systematic review of randomized controlled trials. J Pediatr. 166(3):767-70.e3.
- Moore DJ, Tao BS, Lines DR, Hirte C, Heddle ML, Davidson GP. (2003). Double-blind placebo-controlled trial of omeprazole in irritable infants with gastroesophageal reflux. J Pediatr. 143(2):219-223.
- Gordon M, Biagioli E, Sorrenti M, Lingua C, Moja L, Banks SS, et al. (2018). Dietary modifications for infantile colic. Cochrane Database Syst Rev. 10(10):CD011029.
- Maldonado-Lobón JA, Blanco-Rojo R, Maldonado J, Ali MA, Almazán MV, Suanes-Cabello A, et al; PROBI-COLIC group. (2021). Efficacy of Bifidobacterium breve CECT7263 for infantile colic treatment: an open-label, parallel, randomised, controlled trial. Benef Microbes. 12(1):55-67.
- Ong TG, Gordon M, Banks SS, Thomas MR, Akobeng AK. (2019). Probiotics to prevent infantile colic. Cochrane Database Syst Rev. 3(3):CD012473.
- Crotteau CA, Wright ST, Eglash A. (2006). Clinical inquiries. What is the best treatment for infants with colic? J Fam Pract. 55(7):634-636.
- Ahmed M, Billoo AG, Iqbal K, Memon A. (2018). Clinical Efficacy Of Lactase Enzyme Supplement In Infant Colic: A Randomised Controlled Trial. J Pak Med Assoc. 68(12):1744-1747.
- El-Serag H, Hill C, Jones R. (2009). Systematic review: the epidemiology of gastro-oesophageal reflux disease in primary care, using the UK General Practice Research Database. Aliment Pharmacol Ther. 29(5):470-480.
- Trojan VV, Levin MD, Makhlin AM. Method for the treatment of gastroesophageal reflux in children. - AS (USSR). No. 1780724.- Publ. BI. 46.-1990.
- Shafik A, Shafik I, El-Sibai O, Mostafa R. (2005). Effect of lower esophageal sphincter distension and acidification on esophageal pressure and electromyographic activity: the identification of the "sphinctero-esophageal excitatory reflex". Ann Thorac Surg. 79(4):1126-1131.
- Levin MD. (2024). Esophageal achalasia or gastroesophageal reflux? Pediatric cases analysis. Gastroenterol Hepatol Open Access. 15(6):174-184.