Current Issue Volume 7, Issue 1 - 2024
Overview and Current Status of Hysteroscopy in Gynecology Practice
Naiknaware Sachin Vijay*
Parkview Hospital, Virar, India
*Corresponding Author: Naiknaware Sachin Vijay, Parkview Hospital, Virar, India; Email: [email protected]
Received Date: March 27, 2024
Publication Date: April 05, 2024
Citation: Vijay NS. (2024). Overview and Current Status of Hysteroscopy in Gynecology Practice. Mathews J Surg. 7(1):27.
Copyright: Vijay NS. © (2024)
ABSTRACT
Since its introduction in gynecology practice in 19th century hysteroscopy has been increasingly performed for various gynecology disorders, the commonest disorders that being diagnosed and treated with hysteroscopy are abnormal vaginal bleeding, endometrial polypectomy, sub mucous myopia resection, metroplasy, infertility evaluation and diagnosis of hyper plastic endometrium and sometimes transcervical resection of endometrium .in premenopausal women with regular menstrual cycles the optimum time for doing hysteroscopy is follicular phase of cycle after menstruation there is not strong evidence at present to support preoperative cervical dilatation. Nowadays there is increased preference for office based hysteroscopy as it is found to associate with cost effectiveness and higher patient satisfaction.
INTRODUCTION
Hysteroscopy is visualization of endometrial cavity with the aid of hysteroscope inserted through the cervix. it is performed for diagnostic and therapeutic indications In recent times modern gynecology has witnessed many technical and technological advances specially in minimally invasive surgery including hysteroscopy due to introduction of small diameter hysteroscope, saline use as a distention media and use of “Vaginoscopic techniques” [1] contributed widespread of hysteroscopy as gold standard technique for evaluation of uterine cavity.
Though laparoscopy has simply modified access to abdominal cavity, hysteroscopy enlighten for the first time the cramped and dark cavity which was not explored till mid-19th century. During 1980 “Traditional Techniques” were used for doing hysteroscopy in which a speculum and Vulsellum was used to hold the cervix and view the uterine cavity but now with the miniaturisation of scopes Vagino-scopic or “no touch technique’’ is being used for doing hysteroscopy. Vaginoscopic approach to Hysteroscopy was developed by Bettochi et al.
Aim of this article is to learn the basic principles required to undertake diagnostic and operative hysteroscopy and to discuss recent advances in hysteroscopic instruments and surgical techniques.
As we all know hysteroscope is used to diagnose intrauterine pathology and to perform surgery within the endometrial cavity. Hysteroscope allows inspection of uterine cavity as whole and allow to take guided biopsies of pathological lesions which could have been missed on doing blind dilatation and curettage. Hysteroscopy offers many benefits to patients requiring evaluation of uterine cavity specially in patient presented with abnormal uterine bleeding and and also in those patients who had been diagnosed on sonography to have some kind of uterine pathology.
FIGO classification system (PALM-COEIN, polyp, adenomyosis, leomyoma, malignancy & hyperplasia, Coagulopathy, ovulatory dysfunction, endometrial, iatrogenic, and not yet classified) adopted in 2011 integrates hysteroscopy findings into the evaluation of abnormal bleeding [2].
INDICATIONS
Hysteroscopy is performed for evaluation of endometrial cavity, endocervix and tubal Ostia. Common indications being [3,4].
• Abnormal uterine bleeding
• Endometrial polyps
• Thickened endometrium
• submucosal fibroids
• Chronic endocervicitis with leucorrhoea
• Endometrial hyperplasia
• Retained products of conception
• Correction of isthmocele
• persistent bleeding after MTP
• Diagnosis of mullein anomalies
• Abnormal findings as seen on sonography.
CONTRAINDICATION
• Active pelvic infection including genital herpes infection [5]
• Variable intrauterine pregnancy
• Known pyometra
• Known cervical cancer.
• coagulopathy, coronary heart disease, excessive uterine bleeding are relative contraindications
OPERATIVE SET UP & INSTRUMENTS


Though office hysteroscopy can be carried out in an outpatient setting, operative hysteroscopy requiring prolonged time require operation theatre the equipments required are
• Video camera
• Monitor
• Cold light source
• Light cable
• Suction irrigation pump
• Hysteroscope
• Resectoscope
• Insufflations media
• Ancillary instruments
Electrosurgical unit
• Tissue retrieval devices
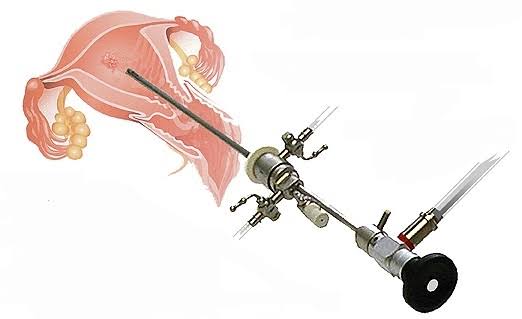
Hysteroscope used can be rigid or flexible, rigid scope consist of glass lenses alternating between air spaces surrounded by fiberoptic bundle to transmit the light to area to be inspected. They are available with 0 degree, 30/45 degree 70 degree angles it consist of 3 parts -eyepiece, barrel, & objective lens, while 0 degree scope give panoramic view of uterine cavity, increasing the viewing angle allows surgeon to inspect areas right or left of midline. Compared to flexible hysteroscope rigid scope can cause more pain but provide better optical quality and they are less costly. While using a hysteroscope total outer diameter and working length of hysteroscope is considered. Outer diameter of hysteroscope refers to diameter of sheath housing telescope & instruments. It ranges from 3 to 10mm working length of hysteroscope is measured eyepiece to distal tip and it measures 160 to 302mm. Operative hysteroscopy requires operative sheath with instruments, resectoscopes and hysteroscopic tissue retrieval system along with distending media.
Light source with connecting light cable attached to eyepiece is used to illuminate the operating field.
Uterine cavity is a potential space between anterior and posterior uterine walls and it endometrial tends to bleed on contact, dictation of uterine cavity is required to provide global view of endometrial cavity and to clear debris. distention media used can be gaseous and fluid, carbon dioxide is the only gas used in hysterocopy which was introduced for use during hysteroscopy in 1972 by H J Lindemann, used at an insufflation pressure of 100-120 mmHg and at a flow rate of 30-60mL/min to maintain an intra cavitary pressure of 40-60 mmHg (6) Two types of liquid distention media are used
1. High molecular weight -dextran
2. Low viscosity fluids which can be either hypotonic electrolyte free media such as Glycine and Sorbitol or isotonic electrolyte containing media such as normal saline and ringer lactate [7].
Surgical planning is most important part starting from patient selection to choosing a good operative setup. surgery starts with preoperative evaluation and preparation of patient starting with explaining and taking informed consent of the patient, patient should be informed about alternative diagnostic and treatment modalities, possible complications, need to abandon or stop the procedure due to any complication. Patient should be evaluated with regard to general condition, obstetric & surgical condition, medical allergies or any medical co-morbidity along with complete pelvic examination including bimanual vaginal examination. Regarding timing of hysteroscopy in premenopausal women proliferative or follicular phase is good for visualisation of uterine cavity and in postmenopausal women it can be done at any time. As many cases have difficulty while introducing the scope it become prudent to to cervical preparation or dilatation of cervix either my medical pharmacological means or by mechanical methods using dilators. Miso-prostol 200-400 ug 24-48hr prior can be used for cervix dilatation.
With everything in place procedure is started with positioning the patient in dorsal lithotomy position and introducing the speculum and use of tenaculum to hold the cervix, then introducing the hysteroscope through cervical os under direct endoscopic vision and then remove the speculum, now a days vaginoscopic or no touch technique is used while introducing smaller dimeter scopes during office hysteroscopy. Start evaluating from endocervix, its gland then advance the scope to inspect the endometrial cavity in systematic fashion with both Ostia, anterior and posterior uterine walls [8].
Sometimes we may face some operative challenges as
1. Cervical stenosis
2. Uterine malposition
3. Difficult uterine distention
4. Vision blur due to bleeding
The challenges that occur during hysteroscopic entry are bleeding, cervix laceration, perforation, vision challenges and unfavourable distention. Difficult entry can be due to cervical stenosis due to ionisation of cervix, LLETZ, previous curettage, Asherman’s syndrome, and Fothergill’s repair. Sometimes it is due to adhesion and fixed direction of cervix. To prevent this complication Misoprostol can be used 4-8 hrs prior to procedure and mechanical dilatation with hears dilator can be used also risk of false passage can be prevented by entry of hysteroscopre under direct vision. If there is severe stenosis put a scissor in operative channel and advances the scope while opening jaw of scissor while advancing the scope and sometimes cruciate incision can be taken on cervix to introduce the scope.
False passage cam sometime be occurs during insertion of scope it is recognized by visualizations of muscle filers with non visualisation of tubal Ostia, in this case remove back the scope slowly and try to identify the true cavity. If cavity could not be seen discontinue the procedure to prevent fluid from being absorbed through the injury and also adequate distention will not be achieved. False passage can be prevented by dilating the cervix slowly and stop as soon as internal os is seen. Put the scope into external os with inflow open and outflow shut and letting fluid pressure dilating the cervix.
Excessive bleeding can occur when endomyometrial junction is breached is in myomectomy or TCRE procedure. When the bleeding is excessive it produces the “JAPANESE FLAG SIGN” obscuring the field of vision. This bleeding can be managed by putting in Foley’s catheter with balloon inflation with 15-30ml go saline, packing with cause soaked in dilute vasopressin and bipolar coagulation.
Perforation can also occur during hysteroscopy with approximately 14 perforations per 1000 operations. Chances of perforation are more in resection of fundal and lateral adhesions it is diagnosed by collapse of cavity, rapid inflow of fluid,bowel or momentum can be seen and scope goes far inside the cavity. Management of perforation depends on what instrument perforated the uterus, if perforation by energy source then laparoscopy is needed and if perforation occurred by cold scissors patient can be observed. It can be prevented by applying current only when electrode is moving toward the operator and simultaneous use of ultrasound or laparoscopy guidance.
Embolism is dreaded complication that may occur when co2 is being used as distention medium but as co2 is soluble in blood emboli can resolve rapidly. Embolism can be prevented by
1. Purge all air from all tubings before introducing scope
2. Intra cervical vasopressin
3. Avoid Trendelenberg
4. Remove last dilator just before introducing scope
5. Limit repeated removal and reinsertion
6. Right equipment’s and setting
Hysteroscopy is technologically dependent and potentially dangerous so proceed only with good knowledge of procedure and equipment’s.
Complications from hysteroscopy are rare but some are potential life threatening some known complications are [9]
1. Uterine perforation
2. Cervical laceration
3. Urinary tract injury
4. Excessive fluid absorption
5. Bowel injury
6. Hemorrhage
7. Embolism
8. Electrosurgical injury
9. Infection
10. Rarely dissemination of tumor.
Recent advance in technology paved way for outpatient office hysteroscopy also introduction of morcellator and resectoscopes and tissue retrieval devises makes hystroscopy a safe, effective alternative to laparoscopic surgery for some intrauterine pathologies. And making it a gold standard tool for investigation and treatment of intrauterine pathologies.
RECENT ADVANCES
Office Hysteroscopy

Also known as see and treat hysteroscopy since 1990 because of small size of scope and less painful procedure it has gained widespread acceptance in clinical practice & currently office hysteroscopy is considered as gold standard for examination of uterine cavity and overcoming the limitations of d &c and other blind procedures [10] for office hysteroscopy either rigid or flexible scope of 4mm/ 2.9mm scope is used. Flexible scopes are less painful as compared to rigid ones requiring no cervical dilatation but they have some limitations
• Higher cost for purchase & maintenance go equipment
• Increased efforts for cleaning, disinfection & sterilisation
• reduced size of image seen on screen
• Fragile
• Difficulty in use in cases of intrauterine adhesions
Saline and co2 are most commonly used distention media used in office hysteroscopy now distention with normal saline is preferred due more patient comfort , its well tolerability & more cost effective also it provides good view in cases of intrauterine bleeding and also vagino-scopic or no touch approach is more easier with saline. Dictation pressure is maintained with electronically controlled suction irrigation pump obtaining constant pressure of < 70mmHg. So now a days office hysteroscopy should be the first option to be considered for diagnosing and treating vaginal, cervical and intrauterine pathologies.

Electronic Suction Irrigation Pump ( Hysteromat)
It is a endoscopic automatic system for irrigation during hysteroscopy. It is a pressure controlled double roller pump that provides sufficient dilatation of uterine cavity with continuous fluid exchange at all times. It offers the benefit ensuring optimal visualisation & constant intrauterine pressure allowing surgeon to perform various intrauterine surgeries with ease.
Intrauterine Bigatti Shaver

Intrauterine Bigatti shaver was developed as an option for hysteroscopic morcellation with the intention to improve the results of conventional resectoscopy reducing by the number of complications, it consist of a 6 degree angled telescope with an integrated sheath and working channel into which a rigid shaver is introduced the diameter of outer sheath. Benefits of using IBS is sustained intraoperative visibility, short procedure time & definitive management of pathology, also it preserves endometrial integrity.
Bipolar Resectoscope
The resectoscope used in hysteroscopy consist of 2.9 / 4mm scope with 12 degree or 30 degree viewing angle to always keep the loop under vision. Two commonly used resectoscopes are monopoly and bipolar resectoscope while conventional hysteroscopy is using monopoly resectoscope in which current passes from the active electrode through the patient’s body toward returning electrode and the distention medium used is glycine. This system is potentially dangerous as since the electron flow s through the body outside the surgeons visual control before it returns to the generator to avoid this complication bipolar resectoscopes are introduced in which the current flows through the tissue is restricted to the area between the two electrodes loop that is under visual control of surgeon.
In conclusion hysteroscopic surgery has allowed gynaecological surgeon to treat various benign intrauterine pathologies via minimally invasive technique improving recovery time, treatment outcome and patient satisfaction.
CONCLUSION
From above literature we can see that many gynaecological operations can be performed with the use of hysteroscope and it will not be wrong to state that hysteroscopy will replace hysterectomy as a therapeutic option in specific cases of heavy menstrual bleeding and menorrhagia and will offer shorter hospital stay and reduced mortality and morbidity along with reduced cost. Now “Hysteroscope Is Being Seen As a Stethoscope Og Gynecologist”
REFERENCES
- Bettocchi S, Selvaggi L. (1997). A vaginoscopic approach to reduce the pain of office hysteroscopy. J Am Assoc Gynecol Laparosc. 4(2):255-258.
- Munro MG, Critchley HOD, Broder MS, Fraser IS, FIGO Working Group on Menstrual Disorders. (2011). FIGO classification system (PAL-COEIN) for abnormal uterine bleeding in non gravid women of reproductive age. Int J Gynecol Obstet. 113:3-13
- Orlando MS, Bradley LD. (2022). Implementation of office hysteroscopy for the evaluation and treatment of intrauterine pathology. Obstet Gynecol. 140(3):499-513.
- Weinberg S, Pansky M, Burshtein I, Beller U, Goldstein H, Barel O. (2021). A pilot study of guided conservative hysteroscopic evaluation of early miscarriages. J Minim Invasive Gynecol. 28(11):1860-1867.
- Price TM, Harris JB. (2001). Fulminant hepatic failure due to herpes simplex after hysteroscopy. Obstet Gynecol. 98:954-956.
- Pellicano M, Guida M, Zullo F, Lavitola G, Cirillo D, Nappi C. (2003). Carbon dioxide versus normal saline as a uterine distention media for diagnostic vagianoscopic hysteroscopy in infertile patients: a prospective randomised multi-centre study. Fertil Steril. 79:418-421.
- Cooper NA, Smith P, Khan KS, Clark TJ. (2011). A Systematic review of the effect of distention medium on pain during outpatient hysteroscopy. Fertile Steril, 95:264-271.
- Centini G, Lazzeri L, Petraaglia F, Luisi S. (2016). Modern operative hysteroscopy. Minerva Ginecol. 68(2):126-132.
- Shveiky D, Rojansky N, Revel A, Benshushan A, Laufer N, Shushan A. (2007). Complications of hysteroscopic surgery: “beyond the learning curve” J Minim I invasive Gynecol. 14:218.
- Sagiv R, Sadan O, Boaz M, Dishi M, Schechter E, Golan A. (2006). A new approach to office hysteroscopy compared with traditionalhysteroscopy: a randomised controlled trial. Obset Gynecol. 108:387.