Information Links
Related Conferences
Previous Issues Volume 4, Issue 1 - 2020
Over View Regarding Efficacy of Clostridium Botulinum Toxin (Botox) For the Management of Various Pathologies
Humaira Zafar1*, Irfan Ali Mirza2, Wajid Hussain3
1Professor of Pathology, Consultant Microbiologist, Al Nafees Medical College & Hospital, Islamabad
2Professor of Pathology & Head Department Of Microbiology, Consultant Microbiologist, Armed forces Institute of Pathology, Rawalpindi
3Assistant Professor of Pathology, Consultant Microbiologist, Department of Microbiology, Armed forces Institute of Pathology, Rawalpindi
*Corresponding author: Humaira Zafar, Prof. of Pathology, Consultant Microbiologist, Department of Pathology, Al Nafees Medical College & Hospital, Isra University Islamabad Campus, Pakistan, Tel: 0333-524-2761; E-mail: [email protected]
Received Date: September 18, 2020
Published Date: October 23, 2020
Copyright: Zafar H, et al. ©2020.
Citation: Zafar H. (2020). Over View Regarding Efficacy of Clostridium Botulinum Toxin (Botox) for the Management of Various Pathologies. Mathews J Pharm Sci. 4(1):02.
ABSTRACT
The Botulinum toxin or Botox is virulent factor produced by Clostridium botulinum. It belongs to a group of Gram positive spore forming rods. Botulinum toxin is a neurotoxin which is inhibiting the release of acetylcholine at neuromuscular junction. The resultant effect is paralysis of specific group of muscles. This Botulinum toxin comprises of seven neurotoxins. Amongst all of them toxin type A and B harbors clinical significance especially in the field of medicine, surgery, and dermatology. The optimum dose ranges from 15 – 20 units. The effect starts within 24 hours to two weeks and last until 3 to 6 months. However published data was limited to assess its efficacy in various conditions. Therefore this review article was planned to get the insight regarding clinical efficacy and side effects of botox for various disorders. The results extracted from the review of literature showed that it is safe with minimum side effects to treat many medical and surgical conditions.
Conclusion: Usage of Botox is safe for the management of various medicines, surgery disorders. The good results can be seen even used for cosmetic purpose. Careful approach should be opted for immunosuppressed patients due to serious side effects.
KEYWORDS: Clostridium botulinum, Botox, Clinical efficacy, Cosmetic use, Use for Anal Fissure, Use for Ophthalmic conditions, Use for Depression, Side effects, Contraindications
INTRODUCTION
Overview: The Botulinum toxin or Botox is virulent factor produced by Clostridium botulinum. It belongs to a group of Gram positive spore forming rods. Botulinum toxin is a neurotoxin which is inhibiting the release of acetylcholine at neuromuscular junction. The resultant effect is paralysis of specific group of muscles. However, excessive amount can result in botulism, which is an illness that affects nerves. This Botulinum toxin comprises of seven neurotoxins. Amongst all of them toxin type A and B harbors clinical significance especially in field of medicine, surgery and dermatology. The optimum dose ranges from 15 – 20 units. The effect starts within 24 hours to two weeks and last until 3 to 6 months [1,2].
History and Indications: Tracing back the history, usage of botox started from the field of ophthalmology in 1970s. With advancement in the field of medicine, its uses have stretched to manage many health disorders [1]. Botox comprises of seven types of neurotoxins. Amongst all of them types A and B harbors clinical significance. In the year 1994, the prolific effects of botox usage were observed for the management of facial wrinkles [3,4]. Afterwards various trials started to identify its efficacy for the treatment of glabellar frown lines, strabismus, blepharospasm, cervical dystonia, platysmal bands in the neck, acne vulgaris, lichen simplex, pompholyx (dyshidrotic eczema), dry skin, vascular abnormalities, second line management of anal fissure prior surgery, hyperhidrosis as well as synkinesis following facial surgery wrinkles around the lips (smoker’s lines) and marionette lines [5,6].
For the first time in the year 2002, Food and Drug Administration (FDA) approved the use of onabotulinum toxin type A. Initially it was approved for the cosmetic management of glabellar frown lines [2,7]. In 2006, the second preparation of onabotulinum toxin A was created in France. This in 2009 was than approved by FDA [8]. From that time till date its use is considered innocuous for cosmetic purpose [9]. The details regarding the history of botox and its uses are mentioned in table 1 [10].
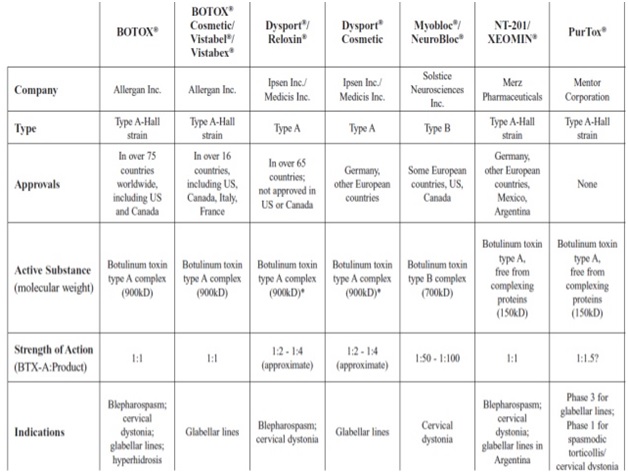
Table 1: Details for the history of botox and its uses [10].
Mechanism of Action for Botox: Botox acts by involving four main steps. In first step, which last approximately for 30 minutes, the toxin binds to the specific receptors on the surface of the presynaptic cells. The second step is characterized by internalization. This is an endocytic receptor-mediated process, which is energy-dependent. There is invagination of plasma membrane of nerve cells around the toxin-receptor complex. Thus, forming a vesicle containing toxin in nerve terminal. The third step is characterized by translocation. In this step disulfide bond is hewed and the 50-kDa light chain of the toxin is released across the endosomal membrane of the endocytic vesicle into the cytoplasm of the nerve terminal. The last and fourth step is a blocking step. In this step, light chain of serotypes A and E hamper the release of acetylcholine. This involves hewing the cytoplasmic protein (SNAP-25), which is required for curtailing acetylcholine vesicles on the internal side of nerve membrane at the neuromuscular junction [11]. The resultant effect of all this is the reversible relaxation of specific group of muscles [12]. The molecular structure for botulinum toxin is shown in figure 1 [13].
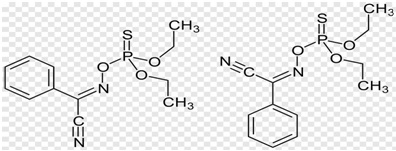
Figure 1: Molecular structure of Botulinum toxin [13].
Contraindication: Besides beneficial effects for management of many conditions, certain contraindications are there for its use. Amongst them the common ones includes myasthenia gravis, multiple sclerosis, pregnancy, breast feedings, eaton Lambert syndrome, amyotrophic lateral sclerosis, allergy or hypersensitivity to Botox, focal or systemic infections, neonates, children, and patients who had previously experienced lower eyelid surgery [14-16].
Dosage: The recommended dose for botox is 20 Units. However, it can vary with the gender and specific indication. For the management of glabellar frown lines, results were good for the dose of 20-40 units as compared to 10 units [7]. One published study reported that men usually requires higher dose as compared to women due to hormonal effects of testosterone and increased muscle mass [17,18]. It was identified that variation in this duration is because of different muscle arrangement [19]. One more study described that for men the effective starting dose is 40 Units [20].
Desired Clinical Effects: The desired clinical effect usually starts to appear on 1st to 4th days after injection. However, maximum reversible effects were seen between 1-4 weeks till 3-4 months. In case of persistent problem, the dose is recommended to be repeated after 6 months or 1 year [21].
Safety: Regarding the safety for botox usage, it harbors a broad margin of safety with a lethal dose of 50% (LD50) in humans. This can even reach upto 40 U/kg body weight (BW) [22,23]. Besides this the effects are reversible changes at nerve terminals and targeted muscles [24,25].
Side Effects: The commonly encountered side effects include pain at the injection sites, swelling, erythema, bleeding and headaches. They usually get resolved within 2-4 weeks time. The chances of appearance of side effects can be reduced by using thin needles and saline dilution prior procedure [26,27]. While in post injection period, use of simple systemic analgesics were found to be helpful for reduction in their severity. Nonetheless, all of them steadily resolve after the paralytic effect of the toxin dissolves [28].
Complications: The complication rate is minimum. It is recommended that before and after usage of ice at injection site will be helpful to reduce the emergence of complications. Besides this upright seating or standing position for 3-4 hrs should be a preferred position for patients [23,24]. One published study (1998), supported that use of botox in immunosuppressed patients can result in necrotizing fasciitis. So care must be taken to dig up good history prior the use of botox [29,30]. In one study it was concluded that for management of anal fissure, minor incontinence of feaces can be seen i.e 2/28 patients. The condition settles down with passage of time [31]. One more study concluded that the complications from botox in cases of anal fissure management can be mild bleeding, haematoma, and abscess formation [32]. However, in one more study it was observed that the healing rate form botox in cases of chronic anal fissure is 84.9%. It was predominant in females with a mean healing time of 4.68 weeks especially in cases having one fissure as compared to two i.e. both anterior and posterior. Nutshell was that it is a safe management option with minimal side effects [33].
CONCLUSION
Usage of Botox is safe for the management of various medicines, surgery disorders. The good results can be seen even used for cosmetic purpose. Careful approach should be opted for immunosuppressed patients due to serious side effects.
RECOMMENDATIONS
- Usage of botox for the management of various medicines, surgery disorders is safe practice having reversible desired effects.
- Immunological status must be evaluated careful prior recommending the use of botox.
- The dose of botox can range from 10 - 40 U/kg body weight (BW).
- It is recommended that before and after usage of ice at injection site will be helpful to reduce the emergence of complications, which are usually seen in minimum cases.
- The use of thin needles and saline dilution prior procedure helps in reduction for the appearance of side effects
CONTRIBUTION OF AUTHORS
Prof Humaira Zafar: Corresponding author, Concept initiation, drafting the entire manuscript. Prof Dr Irfan Ali Mirza: Supervising entire manuscript for technicalities, Discussion writing. Dr. Wajid Hussain: Gathered references based upon inclusion and exclusion criteria, Introduction write up.
CONFLICT OF INTERESTS
None to declare.
REFERENCES
- Awan KH. (2017). The therapeutic usage of botulinum toxin (Botox) in non-cosmetic head and neck conditions – an evidence based review. Saudi Pharm J. 25(1):18–24. doi:10.1016/j.jsps.2016.04.024.
- Satriyasa BK. (2019). Botulinum toxin (Botox) A for reducing the appearance of facial wrinkles: a literature review of clinical use and pharmacological aspect. Clin Cosmet Investig Dermatol. 12:223–228. doi: 10.2147/CCID.S202919.
- Markey AC. (2000). Botulinum A exotoxin in cosmetic dermatology. Clin Exp Dermatol. 25(3):173–175.
- Raspaldo H, Niforos FR, Gassia V. (2011). Consensus Group. Lower-face and neck antiaging treatment and prevention using onabotulinum toxin A: the 2010 multidisciplinary French consensus–part 2. J Cosmet Dermatol. 10(2):131–149. doi:10.1111/j.1473-2165.2011.00560.x.
- Almeida ART, Secco LC, Carruthers A. (2011). Handling botulinum toxins: an updated literature review. Dermatol Surg. 37(11):1553–1565.
- Michael AC, Kane MD. (2005). Botox injections for lower facial rejuvenation. Oral MaxillofacSurgClin North Am. 17(1):41–49. doi:10.1016/j.coms.2004.09.003.
- Cohen JL, Dayan SH, Cox SE, Yalamanchili R, Tardie G. (2012). Onabotulinumtoxin A dose-ranging study for hyperdynamic perioral lines. Dermatol Surg. 38(9):1497–1505. doi:10.1111/j.1524-4725.2012.02456.x.
- Flynn TC. (2012). Advances in the use of botulinum neurotoxins in facial esthetics. J Cosmet Dermatol. 11(1): 42–50. doi:10.1111/j.1473-2165.2011.00593.x.
- Klein AW. (2004). Complications with the use of botulinum toxin. DermatolClin. 22(2):197–205.
- Agarwal RK. Clostridial toxins; Botulinum toxins. Available from: [https://www.slideshare.net/RaviKantAgrawal/costridial-toxins-botulinum-toxin]. Retrieved on: Oct 15th 2020.
- Wollina U, Konrad H, Petersen S. (2005). Botulinum toxin in dermatology–beyond wrinkles and sweat. J Cosmet Dermatol. 4(4):223–227. doi:10.1111/j.1473-2165.2005.00195.x.
- Khawaja HA, Perez HE. (2001). Botox in dermatology. Int J Dermatol. 40(5):311–317.
- Botulinum toxin. Available from: [https://pngio.com/PNG/a120058-botulinum-toxin-png.html]. Retrieved on: Oct 15th 2020.
- Rzany B. (2007). Requirements and rules In: Philipp M, editor. Botulinum Toxin in Aesthetic Medicine. Berlin: Springer. 21:24.
- Gart MS, Gutowski KA. (2016). Overview of botulinum toxins for aesthetic uses. Clin Plast Surg. 43(3):459–471. doi:10.1016/j.cps.2016.03.003.
- Cula GO, Bargo PR, Nkengne A, Kollias N. (2013). Assessing facial wrinkles: automatic detection and quantification. Skin Res Technol. 19(1):243–251. doi:10.1111/j.1600-0846.2012.00635.x.
- Maio DM, Rzany B. (2007). Injection technique In: Rzany B, editor. Botulinum Toxin in Aesthetic Medicine. New York: Springer Verlag Berlin Heidelberg. 25:26.
- Carruthers JA, Lowe NJ, Menter MA. (2002). A multicenter, double-blind, randomized, placebo-controlled study of the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J Am Acad Dermatol. 46(6):840–849.
- Carruthers A, Carruthers J. (2005). Upper face treatment In: Carruthers A, Carruthers J, editors. Botulinum Toxin. 1st ed. Philadelphia: Elsevier Saunders. 31:43.
- Bauman L. (2009). Botulinum toxin In: Baumann L, Elsaie ML, Grunebaum L, editors. Cosmetic Dermatology. 2nd ed. New York: McGraw Hill. 169:190.
- Klein AW. (2004). Contraindications and complications with the use of botulinum toxin. Clin Dermatol. 22(1): 66–75. doi:10.1016/j.clindermatol.2003.12.026.
- Ascher B, Talarico S, Cassuto D. (2010). International consensus recommendations on the aesthetic usage of botulinum toxin type A (Speywood Unit)–part II: wrinkles on the middle and lower face, neck and chest. J Eur Acad Dermatol Venereol. 24(11):1285–1295. doi:10.1111/j.1468-3083.2010.03728.x.
- Maio M, Rzany B. (2007). Patient selection In: Botulinum Toxin in Aesthetic Medicine. Springer. 11:19.
- Carruthers A, Carruthers J, Said S. (2005). Dose-ranging study of botulinum toxin type A in the treatment of glabellar rhytids in females. Dermatol Surg. 31(4):414–422.
- Hexsel C, Hexsel D, Porto MD, Schilling J, Siega C. (2011). Botulinum toxin type A for aging face and aesthetic uses. Dermatol Ther. 24(1):54–61. doi:10.1111/j.1529-8019.2010.01378.x.
- Cox SE, Adigun CG. (2011). Complications of injectable fillers and neurotoxins. Dermatol Ther. 24(6):524–536. doi:10.1111/j.1529-8019.2012.01455.x.
- Klein AW. (2003). Complications, adverse reactions, and insights with the use of botulinum toxin. Dermatol Surg. 29(5):549–556.
- Ogden S, Griffiths TW. (2008). A review of minimally invasive cosmetic procedures. Br J Dermatol. 159(5):1036–1050. doi:10.1111/j.1365-2133.2008.08845.x.
- Latimer PR, Hodgkin SAN, Vakalis RE, Butler AR. (1998). Necrotising fasciitis as a complication of botulinum toxin injection. Evans Eye. 12(2):51-53. doi: 10.1038/eye.1998.9.
- Nigam PK, Nigam A. (2010). Botulinum Toxin. Indian J Dermatol. 55(1):8–14. doi: 10.4103/0019-5154.60343.
- Radwan MM, Ramdan K, Azab IA, Fikri M, Zidan A. (2007). Botulinum toxin treatment for anal fissure. Afr Health Sci. 7(1):14–17.
- Poh A, Tan KY, Choen SF. (2010). Innovations in chronic anal fissure treatment: A systematic review. World J Gastrointest Surg. 2(7):231–241. doi: 10.4240/wjgs.v2.i7.231.
- Soltany S, Hemmati HR, Toussy JA, Salehi D, Toosi PA. (2020). Therapeutic properties of botulinum toxin on chronic anal fissure treatment and the patient factors role. J Family Med Primary Care. 9(3):1562-1566.