Information Links
Related Conferences
Current Issue Volume 8, Issue 2 - 2025
Numbing Thumb of Laparoscopic Surgeon: Report of Own Experience and Literature Review
Bharat Mani Banjade1,*, Lok Bahadur Kathayat2, Prakriti Kunwar3, Anup Shrestha4, Nabin Pokhrel5
1General Surgery, ADH. Atoll Hospital, Ministry of Health, Maldives
2General Surgery, James Paget University Hospital NHS Foundation Trust, Great Yarmouth, GBR
3Department of Anesthesiology, Kathmandu Medical College Private Limited, Kathmandu, Nepal
4General Surgery, Charak Memorial Hospital, Pokhara, Nepal
5Lecturer, General Surgery, Universal College of Medical Sciences, Rupandehi, Nepal
*Corresponding Author: Bharat Mani Banjade, General Surgery, ADH. Atoll Hospital, Ministry of Health, Maldives, Phone: +960 9786297, ORCID: 0000-0002-2849-6584, E-mail: [email protected]
Received Date: April 14, 2025
Published Date: August 21, 2025
Citation: Banjade BM, et al. (2025). Numbing Thumb of Laparoscopic Surgeon: Report of Own Experience and Literature Review. Mathews J Surg. 8(2):39.
Copyrights: Banjade BM, et al. © (2025).
ABSTRACT
Background: In this era of minimal invasive surgery, laparoscopy (key hole) is more frequently offered as the preferred approach. It has many advantages to the patient: for example, shorter hospital stay, less painful and early recovery. If laparoscopic instruments are not handled properly especially during difficult dissection and prolonged surgery, it may affect the health of the operating surgeon itself. One of such hazard is superficial nerve damage or neurapraxia. Case Report: Recently author experienced neurapraxia following repeated and prolonged laparoscopic surgery on his non-dominant thumb. It was managed conservatively with rest (abstinence) and watchful waiting. Thorough literature review and a small survey among other fellow surgeons revealed similar experience. Its causes, prevention and the management are discussed here with. Conclusion: Neurapraxia as a hazard in handling laparoscopic instruments seems under reported due to its benign and self-limiting course. Some modification in laparoscopic devices and knowledge of ergonomics can prevent such cases.
Keywords: Ergonomics, Hazards of Laparoscopic Instruments, Laparoscopic Surgery, Neurapraxia, Surgeon’s Thumb.
INTRODUCTION
In this era of modern surgical practice, the safety of the patient lies on top most priority. Taking this into consideration, minimal invasive surgery like laparoscopic or key hole is more frequently offered as the preferred approach. It has many advantages to the patient; for example, less painful, small scar, lower surgical site infection (SSI), shorter hospital stays and the most importantly early recovery. Prioritizing the patient's safety and the overall outcome is crucial, but this shouldn’t jeopardize the surgeon's health itself. Although this approach has mostly benefited patient, it has affected the health of healthcare providers as well and it is mostly to the surgeon in many ways. Among the many hazards of laparoscopic surgery, we aim to discuss one of the author’s own personal experiences with digital neurapraxia in this article. We also reviewed the existing literature on this topic and its prevention as well as its management.
CASE REPORT
Author is a right handed, young general and laparoscopic surgeon. He regularly performs laparoscopic surgeries such as appendectomies, cholecystectomies, hernia repair and diagnostic laparoscopy.
First event:
He noticed numbness and tingling sensation at the tip of his thumb on non-dominant hand, around 2 hours following his 2nd laparoscopic cholecystectomy of the day. Both of the surgery on the day had difficulties in Calot’s dissection. Operating time was 55 minutes and 75 minutes respectively. He had performed a difficult cholecystectomy 1 week back where he struggled in dissection of adhesions and the operating time was 200 minutes. His numbness was localized to the tip at ulnar boarder of the left thumb precisely medio-ventral aspect, around 3x2 cm in area which is supplied by superficial digital branch of median nerve.
Picture1
Numbness was continuous; tingling was on and off without relieving factors and marked on pressure. The two point discrimination in normal fingers was 6-8 mm but it was 10 mm in the involved thumb. There was no motor involvement. Rests of the fingers on same hand as well as on the opposite dominant hand were normal. The general health condition was essentially normal. Watchful waiting and abstinence of laparoscopic surgery was done for a week. Paresthesia persisted for 6 days and resolved completely in 9 days, indicating neurapraxia.
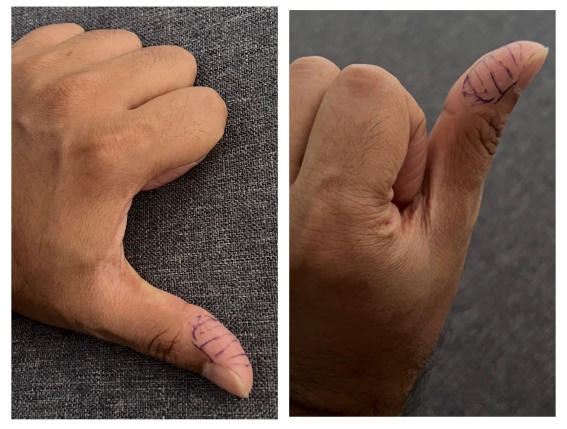
Picture1. Area of anesthesia on surgeon’s left thumb.
Second event:
Similarly, the author noticed similar numbness on the same thumb after 8 months of the previous experience. This time, the numbness was noticed 12 hours following a complicated cholecystectomy (operating time 250 minutes). The numbness was more localized to the ulnar aspect, 2x2 cm which was profound for 5 days, completely weaned on 8th day without additional treatment.
Third event:
Not limiting to that, author noticed similar numbness on the same thumb for the third time. This was 10 months following the second and 18th month of initial event. This time it was localized at medio-ventral aspect, 4x4 cm on the same thumb on non-dominant hand. This was noticed on 3rd day of the advanced laparoscopic training course where the author had handled the laparoscopic instruments for longer time (>240 minutes/day) for consecutive 3 days. Here he struggled to perform difficult and advanced steps like anastomosis and intra-corporeal suturing which generated extra pressure on the thumb. This resolved again spontaneously within 2 weeks by abstinence of laparoscopic surgery only.
Following this author decided to perform small online survey among colleague surgeons who were actively involved in laparoscopic surgery. Altogether 22 surgeons responded to the survey. Among them 17 denied any form of symptoms; however, 4 of them had some kind of numbness in their fingers but failed to recall exact location or duration. Surprisingly, one right-handed colleague remembered his left thumb getting numb for 2-3 weeks which resolved gradually without any treatment.
DISCUSSION
Laparoscopic surgery has become a mainstay of modern surgery, especially in general surgery, urology, gynecology and cardiothoracic surgery [1]. Apart from advantages of laparoscopic surgeries like less painful, small scar, lower rate of SSI, less hospital stays and early recovery, one of the disadvantage is longer operating duration. The surgeons expected to work long hours in operating theatres, seems to have affected their own health directly. They are experiencing a greater physical discomfort than in open surgery, mostly due to poor ergonomic design of instruments and their operating positions [1,2].
The hazards of laparoscopic surgery were explained long way back in early 1990s [1,3]. There are many other reported hazards, some of them are listed below [3-9].
- Musculo-skeletal disorders in physical body parts ranging from the neck (neck tension syndrome) shoulders, pectoral tendonitis, upper back and lower back to upper extremities.
- Nerve entrapment like ulnar and carpal tunnel syndrome including digital nerve neurapraxia.
- Surgical fatigue syndrome.
- Deterioration of visual acuity and functions of the ocular muscles.
- Minimal access surgery related surgeon morbidity syndromes.
- Pressure sore.
Digital nerve neurapraxia is not uncommon and have been reported sporadically. We did a thorough literature search in PubMed and Google Scholar with key words like ‘digital neurapraxia’, ‘surgeons thumb’, ‘hazards of laparoscopic surgery’, and ‘ergonomics in surgery’. We could find few reported cases, most of them were reported in 1990s and first decade of 2000. Advancement of laparoscopic tools and the acquisition of the laparoscopic skills by surgeons might have reduced the incidences in recent days and hence less reported [10].
Table 1 summarizes the reported literature with the details of authors, thumb and the nerves involved as well as the duration to resolve that condition.
Table 1. Literature review
|
Authors, Country (Date) |
Number of surgeons |
Involved thumb and the nerve |
Duration |
Treatment |
|
Majeed AW. Et al. in England (1993)[1] |
2 |
Both left thumb; Lateral digital nerve |
6 days; and 12 weeks |
Not mentioned |
|
Kano N. et al in Japan (1995) [2] |
2 |
Left Thumb 1, Right Thumb 1; Both lateral digital nerve |
Several hours to few days |
Not mentioned |
|
In Netherland (1995)[11] |
2 |
Thumb rest details not mentioned |
Few days; and >8 weeks |
Not mentioned |
|
Lee WJ et. Al in Korea (2001)[12] |
Not mentioned |
Thumb; Digital nerve (superficial branch of the radial nerve) |
Not available |
Not mentioned |
|
Lawther RE. et al in UK (2002)[4] |
20 |
9 Right, 6 Left and 5 Bilateral thumb; mostly ulnar aspect |
9 hours |
Not mentioned |
|
Verma GR in India (2004)[5] |
1 |
Right Thumb; Not mentioned about the nerve |
6 weeks |
Not mentioned |
|
Our case in Nepal (2025) |
2 |
Both Left Thumb; Proper palmer digital nerve branch of the median nerve, ulnar boarder |
2 weeks; and 3 weeks |
Conservative, rest and deferral of surgery |
Cutaneous innervation of thumb includes both median and radial nerve. Proper palmer digital branch of median nerve supply most of the thumb leaving an area on radial and or dorsal aspect starting in between nail bed and inter-phalangeal joint. This area is supplied by the dorsal digital branch of radial nerve [13,14] (Picture2).
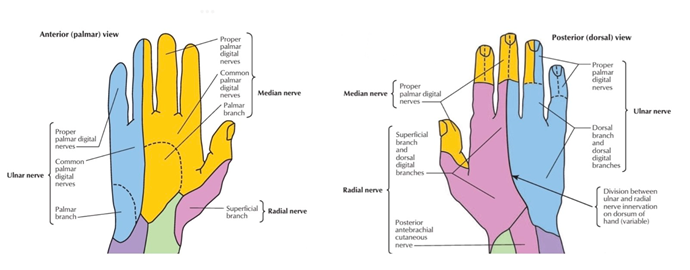
Picture 2. Distribution of nerve supply in thumb and hand [14].
Peripheral nerve injury can occur in different types of severity. The mildest form is called neurapraxia, and according to the Sunderland classification, it is considered as grade 1 [15]. Neurapraxia occurs when the myelin sheath of nerve is damaged due to focal demyelination or ischemia. Usually, neurapraxia is caused by crushing, ischemia, or traction, although other factors such as heat, electric shock, radiation, percussion, and vibration can also be involved. Despite the damage to the myelin sheath, the endoneurium, perineurium, and epineurium of the nerve remains intact [16].
These injuries have an excellent prognosis and they can be managed conservatively with orthotic measures like splints and support [17]. Otherwise this condition is self-limiting but, sometimes it may alter tactile sensation to an extent that the surgeon's performance is impaired in subsequent operations. Neurologists have tried analgesics, antidepressants, anticonvulsants, corticosteroids and anesthetics in the treatment of such cases [17]. Most of the injuries recover within a week but some may take around 8–12 weeks [18,19]. Persistent compression can result in a delayed recovery or full recovery thereby causing permanent damage to the digital nerve, recommending preventing repeated injury.
Other similar conditions are reported where they have documented a similar constellation of symptoms and the etiology. These include numbing thumb in bowlers, jewelers, cherry pitters, baseball players, and massage therapists [20-23]. The main stay of treatment in all of such condition has been conservative as in surgeon’s thumb, with recommended rest, relief of pressure, and avoidance of the inciting activity. Duration to resolve this condition is variable 1-12 weeks [1,5]. When symptoms remain refractory to conservative measures, surgery is the alternative option. Several techniques have been described including neurolysis, neurectomy, and transposition of the ulnar digital nerve.
Difficult dissection or lengthy retraction can cause the pressure on the operator’s digital nerves causing digital neurapraxia [1,5]. Due to the instrumentation with the arms in abduction the force exerted by the four fingers has to be counteracted by a force of the thumb which is transverse on the digital axis [11].
The reason of excessive pressure exerted over the thumb ring of the handle may be due to jaw movements that are mainly brought about by the thumb ring of instrument. And involvement of left thumb in cholecystectomy may be due to continuous pressure applied while retracting Hartman’s pouch with left instrument which lacks the lock system. Another frequently used instrument is the laparoscopic dissecting forceps. The thumb grip is at the back of the mobile arm of this instrument. While dissecting tissues, the force is transmitted from thumb to handle ring and then to the tip of instrument. In this process the lateral surface of thumb repetitively and forcibly presses against the inner aspect of thumb ring of the handle resulting in pressure changes on the skin and digital neurapraxia of thumb. Oversized or uneven distributed pressure to the hand caused by the handle is another potential cause of injury [24].
Although some modifications in new laparoscopic instruments have been made, the design itself, poor ergonomics and the prolong duration of surgery are the main causes of this condition. Ergonomic handles can improve surgeon performance and protect surgeon from potential injuries. Only with a close engagement between the surgeon and the ergonomist will the eventual design of handles for laparoscopic surgical instruments be optimized [24].
CONCLUSION
Digital neurapraxia is a common condition which seems to be under reported due to its benign course and spontaneous recovery without the need of additional treatment. On long run there is possibility of limitation in surgeon’s skill due to permanent damage which may require surgical intervention. Improved ergonomics could be achieved by redesigning instruments with larger contoured surface areas and without angular elevation. This should reduce the pressure transmitted to the operator's digital nerves and lower the frequency of this complication. Some modifications in instruments and good ergonomic knowledge in handling laparoscopic instruments may help to prevent such condition.
ACKNOWLEDGEMENT
We gratefully acknowledge all the surgeons who participated in the survey and contributed to this research.
AUTHOR CONTRIBUTION
Bharat Mani Banjade is a primary and corresponding author. All other co-authors assisted in literature review, manuscript drafting and carrying out the survey. All authors approved the final manuscript.
COMPETING INTERESTS
We declare that we don’t have any competing interests
REFERENCES
- Majeed AW, Jacob G, Reed MW, Johnson AG. Laparoscopist's thumb: an occupational hazard. Arch Surg. 1993 Mar;128(3):357.
- Kano N, Yamakawa T, Ishikawa Y, Miyajima N, Ohtaki S, Kasugai H. (1995). Prevention of laparoscopic surgeon's thumb. Surg Endosc. 9(6):738-739.
- Sackier JM, Berci G. (1992). A laparoscopic hazard for the surgeon. Br J Surg. England. p. 713.
- Lawther RE, Kirk GR, Regan MC. (2002). Laparoscopic procedures are associated with a significant risk of digital nerve injury for general surgeons. Ann R Coll Surg Engl. 84(6):443.
- Verma GR. (2004). Pressure sore and digital neuropraxia of the thumb in laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 14(3):178-179.
- Catanzarite T, Tan-Kim J, Whitcomb EL, Menefee S. (2018). Ergonomics in Surgery: A Review. Female Pelvic Med Reconstr Surg. 24(1):1-12.
- Reyes DA, Tang B, Cuschieri A. (2006). Minimal access surgery (MAS)-related surgeon morbidity syndromes. Surg Endosc. 20(1):1-13.
- Belsole RJ, Greeley JM. (1988). Surgeon's acute carpal tunnel syndrome: an occupational hazard? J Fla Med Assoc. 75(6):369-370.
- El Boghdady M, Ewalds-Kvist BM. (2024). General surgeons' occupational musculoskeletal injuries: A systematic review. Surgeon. 22(6):322-331.
- Inaki N, Kanehira E, Kinoshita T, Komai K, Omura K, Watanabe G. (2007). Ringed silicon rubber attachment prevents laparoscopic surgeon's thumb. Surg Endosc. 21(7):1126-1130.
- van der Zee DC, Bax NM. (1995). Digital nerve compression due to laparoscopic surgery. Surg Endosc. 9(6):740.
- Lee WJ, Chae YS. (2001). Superficial nerve damage of thumb of laparoscopic surgeon. Surg Laparosc Endosc Percutan Tech. 11(3):207-208.
- Strandring S. (2016). Grays Anatomy: The Anatomical Basis of Clinical Practice. 41st ed. Elsevier.
- Atlas of Human Anatomy. (2019). 7th ed. Philadelphia, PA 19103-2899: Elsevier.
- SUNDERLAND S. (1951). A classification of peripheral nerve injuries producing loss of function. Brain. 74(4):491-516.
- Omejec G, Podnar S. (2020). Contribution of ultrasonography in evaluating traumatic lesions of the peripheral nerves. Neurophysiol Clin. 50(2):93-101.
- Ferrante MA. (2018). The Assessment and Management of Peripheral Nerve Trauma. Curr Treat Options Neurol. 20(7):25.
- Sunderland S. (1990). The anatomy and physiology of nerve injury. Muscle Nerve. 13(9):771-784.
- Zuckerman SL, Kerr ZY, Pierpoint L, Kirby P, Than KD, Wilson TJ. (2019). An 11-year analysis of peripheral nerve injuries in high school sports. Phys Sportsmed. 47(2):167-173.
- Viegas SF, Torres FG. (1989). Cherry pitter's thumb. Case report and review of the literature. Orthop Rev. 18(3):336-338.
- Thirupathi R, Forman D. (1983). The Jeweller's Thumb: An Occupational Neuroma A Case Report. Orthopedics. 6(4):438-440.
- Chen CC, Chien HF, Chen CL. (2014). Compression neuropathy of the ulnar digital nerves in the thumbs of a massage therapist. Ann Plast Surg. 72(6):649-651.
- Halsey JN, Therattil PJ, Viviano SL, Fleegler EJ, Lee ES. (2015). Bowler's Thumb: Case Report and Review of the Literature. Eplasty. 15:e47.
- Li Z, Wang G, Tan J, Sun X, Lin H, Zhu S. (2016). Building a framework for ergonomic research on laparoscopic instrument handles. Int J Surg. 30:74-82.