Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2023
Merits of Percutaneous Nephrolithotomy for Large and/or Complex Renal Stones “Retrospective Study”
Sami A Abbas*
National Institute of Urology & Nephrology, Cairo, Egypt
*Corresponding author: Sami A Abbas, M.D, National Institute of Urology & Nephrology, Cairo, Egypt; E-mail: [email protected].
Received Date: February 06, 2023
Published Date: March 15, 2023
Citation: Abbas SA. (2023). Merits of Percutaneous Nephrolithotomy for Large and/or Complex Renal Stones “Retrospective Study”. Mathews J Urol Nephrol. 5(1):13.
Copyrights: Abbas SA. © (2023).
ABSTRACT
Background: Percutaneous Nephrolithotomy (PNL) is a well-established technique for the removal of renal stones. Large and complex renal stones are difficult stones to deal with. Aim of Study: This study is to evaluate our results of PNL for the treatment of large and complex renal stones concerningstone-free rates (SFR) and complications. Patients and Methods: From From 2012 to 2022, four hundred and four renal units with large and/or complex renal stones were subjected to PNL. Eighty-nine per cent were males and 11% were females. The average stone surface area (SA) was 872mm2. Results: Stone-free rate (SFR) was 79% for cases submitted to PNL alone and 88.4% for those managed with auxiliary procedures. Hospital stay ranged from 2 to 21 days (Av. 3.6 days). The overall complication rate was 8% and was managed conservatively. Conclusion: PCNL is a safe and effective procedure for the management of large and complex renal stones. There was a significant decrease in the overall stone-free rate and increased complication rates with increased stone surface area. Stones >1500mm2 are difficult stones for any modality. A multimodal approach should be thought of for large and complex renal stones.
Keywords: Kidney, Kidney Calculi, Percutaneous Nephrolithotomy, Intracorporeal, Lithotripsy, Large, Complex, Minimally Invasive.
INTRODUCTION
SINCE its introduction into the endourologist's armamentarium almost 40 years ago [1], percutaneous nephrolithotomy (PNL) has become the standard of care for patients with large-volume nephrolithiasis.
Innovations in renal access, optics, radiology, and improvements in lithotripsy all contributed to that modern-day PNL is the minimally invasiveprocedure of choice for removing large and complex renal stones [2].
PATIENTS AND METHODS
Between March 2012 and September 2022, three hundred eighty-two patients with 404 renal units (bilateral in 22 cases) were diagnosed as having large and/or complex renal stones. They were managed by Percutaneous Nephrolithotomy (PNL) at (the National Institute of Urology and Nephrology, Cairo, Egypt).
Inclusion criteria involved patients with large (SA≥300mm2) and/or complex (Table 1) renal stones. The stone burden was measured according to the stone surface area (SSA) formula shown in Fig. (1) on plain UT [3], planimeter [4] or NCCT software [5].
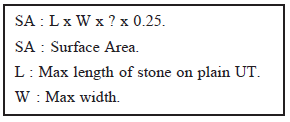
Figure 1. Stone surface area formula [3].
Eighty-nine Percent of patients were males and 11% were females. The mean age was 49.3 years (11-81 Ys).
Table 1. Complex renal stones.
|
Complex Renal Stones |
|
Multiple |
|
Complete Stag |
|
Partial Stag |
|
Caliceal infundibular stenosis |
|
Caliceal diverticulum |
|
Others |
Imaging of the urinary tract was carried out by plain UT and abdominopelvic ultrasonography (US) in all cases. On diagnosis of renal stones,non- contrast computed tomography (NCCT) or excretory urography (EXU) was done for detailed anatomy of the pelvi-caliceal system.
Technique
Most of the cases were operated upon under general anaesthesia. Epidural anaesthesia was used when indicated (14.8% 0f PNL sessions). An epidural catheter was inserted targeting a level between T6-T8. The sensory assessment was done using pinprick and motor assessment by Bromage score.
Opacification of the collecting system was usually achieved by retro-grade pyelography (RGP). Ultrasonography (US) was used to localizethe upper tract in a few cases. In all cases, the procedure was completed under full fluoroscopic control.
Patients were positioned prone in most of the cases. Supine position (36 cases) was used in patients with high body mass index (BMI).
Access to the pelvi-caliceal system was carried out through the lower posterior calyx in most of the cases. Middle or upper calyces accesses were also tried. Supracostal puncture was attained when necessary. The single puncture was performed in most of the cases and multiple punctures in complexrenal stones. Dilation of the tract was done by Alken sequential telescopic metal dilators or balloon dilators. Ampltz sheath with safety guide wire insertion was followed in all cases.
Lithotripsy of the stone (s) was done by Pneumatic and/or ultrasound lithoclasts in most cases. Ho-Yag Laser was used with flexible nephroscopy or ureteroscopy. A nephrostomy tube was inserted after completion of the procedure (18-20 CH) in most of the cases.
Post-operative control KUB films were attainedfor the determination of stone- free rate (SFR). Ultra-sonography and/or NCCT was done for lucent stones. Stone fragments ≥4mm were considered a failure. Anti-grade nephrostogram was done when clinically indicated (postoperative pain, fever, persistent leak, suspected pelvi-caliceal injuries...etc.).
Statistics
Univariate analyses (χ2 and t-test) and the Pearson correlation model were used to determine factors affecting complications and stone-free rate. The data were analyzed using Statistical Package for Social Sciences, version 22 (SPSS Inc., Chicago, IL). A p-value of <0.05 was considered statistically significant.
RESULTS
Four hundred and four renal units in 382 patients with large and/or complex renal stones were managed by PNL at (The National Institute of Urology and Nephrology, Cairo, Egypt) between March 2012 and September 2022.
The mean SSA was 872mm2 (Table 2). Complex renal stones were diagnosed in 54.2% of cases (Table 4,6).
Table 2. Stone surface area (mm2).
|
Min |
Max |
Mean |
±SD |
|
491 |
2551 |
872.4 |
401.9 |
Table 3. Stones Size and number.
|
Single |
Multiple |
|
|
No (%) |
338 (83.5) |
66 (16.5) |
|
Mean SSA (+SD) |
905 (429.2) |
704 (93.2) |
Table 4. Complex renal stones.
|
Complex Stones |
N |
% |
|
Multiple |
66 |
16.3 |
|
Complete Stag |
85 |
21 |
|
Partial Stag |
65 |
16.1 |
|
Infundibular stenosis |
2 |
0.5 |
|
Caliceal diverticulum |
1 |
0.3 |
|
Total |
219 |
54.2 |
Table 5. Stone distribution and configuration.
|
No Site |
Single |
Multiple |
Total |
|||
|
N |
% |
N |
% |
N |
% |
|
|
Pelvic |
170 |
42 |
12 |
3 |
182 |
45 |
|
Caliceal |
12 |
3 |
20 |
5 |
32 |
8 |
|
Pelvic & caliceal |
150* |
37 |
32 |
8 |
182 |
45 |
|
Kidney & upper ureter |
6 |
1.5 |
2 |
0.5 |
8 |
2 |
|
Total |
338 |
83.5 |
66 |
16.5 |
404 |
100 |
The mean operative duration was 95 min (23) Complication No% Management ranging from 55 to 150 min. The nephrostomy tube was removed post-procedural in a mean of 2.8 (1-10) days. The mean hospital stay was 3.6 (2-21) days.
The procedure was completed with PNL alone in 86.1% of cases and with auxiliary procedures in 13.9% (flexible ureteroscopy in 6.2% and SWL in 7.7% of cases).
Table 6. Stone in Calices with Infundibular Stenosis and Caliceal Diverticulum.
|
Stone Site |
Infundibular Stenosis |
Caliceal Diverticulum |
|
Caliceal single |
2 |
1 |
|
Multiple |
4 |
2 |
|
Pelvic & caliceal |
4 |
3 |
|
Total |
10 |
6 |
Table 7. SFR Relations.
|
Stone Free Rate |
p |
|
SSA |
0.039 |
|
Site |
0.143 |
|
Complexity |
0.015 |
|
Stone N° |
0.77 |
|
Stone Surface Area |
p |
|
Tract N° |
<0.001 |
|
Session N° |
<0.001 |
|
Operative time |
<0.001 |
|
Hospital Stay |
<0.001 |
|
Nephrostomy tube duration |
<0.001 |
|
Auxiliary procedure |
0.082 |
Table 9. Complications and their management.
|
Complication |
No |
% |
Management |
|
Bleeding |
8 |
2 |
Blood transfusion |
|
Persistent leak |
10 |
2.5 |
JJ stent |
|
Infection |
8 |
2 |
J J stent+antibiotics |
|
Perforation |
4 |
1 |
JJ stent |
|
A-V fistula |
2 |
0.5 |
Angio-embolization |
|
Colon injury |
1 |
0.3 |
JJ stent+conserve |
|
Total |
33 |
8.3 |
Table 10. Complication relations.
|
Complications |
p |
|
SSA |
0.165 |
|
Stone site |
0.646 |
|
Complexity |
0.441 |
|
Multiplicity |
0.494 |
|
Tract N° |
0.032 |
|
Session N° |
0.01 |
|
Operative time |
0.087 |
|
Hospital stay |
0.09 |
|
Nephrostomy tube duration |
0.091 |
Management of renal stones is a major issue for most urologists. Technological advances and changing treatment patterns have had an impact on current treatment recommendations, which have shifted towards endourologic procedures [6].
Although early on ESWL was used almost indiscriminately for the management of upper tract calculi, the limitations of the technique for large and complex stones became evident over time and PCNL became firmly established in the therapeutic armamentarium of nephrolithiasis [7]. PNL efficacy is little affected by stone size. Stones >20mm (>300 mm2) should therefore be treated primarily by PNL because SWL often requires multiple treatments [8]. The European Association of Urology guidelines [9] and the American Urological Association (AUA) guidelines [10] recommend PCNL for the treatment of renal stones ≥2cm (> 300mm2). In our study, the average SSA was >847mm2 (30mm).
Increasing expertise and technical modifications have expanded the role of PNL to include complex renal calculi, staghorn calculi (complete or partial) and multiple large bulk calculi [1]. PCNL mono- therapy for complex renal calculi has high success and clearance rates combined with minimal morbidity [11]. In our study, complex renal stones represented 52% of cases.
The American Urologic Association Guidelines for the Management of Staghorn Calculi stated, “Percutaneous nephrolithotomy should be the first treatment used for most patients with stones” [12]. In the UK, 30% of stones managed by PNL were staghorn calculi [13]. In our study, staghorn calculi represent 21% of cases.
Since 2000, PNL has made open surgery for complex renal stones obsolete in most countries [2]. Most urological centres worldwide report a need for open surgery in only 1-5.4% of cases. However, in developing countries, the rate of open stone surgery refers to up to 14% [14]. The most common current indications for open stone surgery include those with a complex stone burden; failure of ESWL or endourological treatment; anatomical abnormalities, morbid obesity, concurrent open surgery, renal transplantation, severe limb contractures and patient preference [20]. Even a nephrectomymay be performed when the involved kidney has negligible function [19]. In our series, no conversionto open surgery was needed.
For large and complex stones, multiple percutaneous accesses are often needed for stones re- moval from separate locations. However, the use of multiple accesses carries a higher risk of bleeding and complications compared with single access [21,22]. Multiple access tracts are needed in as many as 20% to 58% of percutaneous procedures. These multiple PNL access tracts are known to increase the risk of renal parenchymal injury [23-26].
In our study, 1/3 of cases were subjected to multiple tracts and this was significantly related to stone surface area and increased rate of complications.
Operative time of an average of 65-112 min was reported in PNL procedures for large and/or complex renal stones [27,28]. It was directly related to stone size.
This study showed the operative time of an average of 95 min (55-150). It had a statistically significantrelation with SSA.
One of the most important factors in selecting the optimal surgical modality for the patient with nephrolithiasis is stone size because size has been shown to strongly influence SFR, the need for secondary procedures, and the complication rate [7]. The stone-free rate for cumulative stone burdens <20mm for both URS and SWL is acceptable and has less morbidity than PNL. Of these treatment options, PNL stone-free rates are the least affected by the stone size, while stone-free rates of both SWL and URS decline with increasing stone burden [29].
For stones with SSA averages ranging from 345-1128mm2 managed with PNL monotherapy, SFR ranged from 49-92% [27,30]. In our study, SSA ranged from 490-2250mm2 and SFR was 79% for PNL mono-therapy and 88% for auxiliary procedures.
Osman and his colleagues [31] reported a 67% of their patients were sufficiently treated by PNL, but 33% needed auxiliary measures. Hamamoto et al., [32] reported a 40% need for ancillary treatment. Auxiliary procedures were needed in only 14% of our patients.
A nephrostomy tube is placed at the end of percutaneous nephrolithotomy (PNL) to aid in hemostasis and drain the pelvi-caliceal system [33]. Historically, a large bore catheter was placed at the end of the procedure and left indwelling for several days to provide drainage and tamponade with the nephrostomy tract. The advantages of a large-bore catheter include reliable and efficient drainage, maintenance of the tract for a secondary procedure and prevention of bleeding from the tract. However, larger tubes are thought to be associated with increased patient discomfort and may not limit postoperative blood loss as initially thought [7]. However, smaller size tubes (≤20F) required less analgesia, less urinary leakage and a shorter hospital stay [34,35].
In our study, an 18-20 CH nephrostomy tube was fixed at the end of most cases. The tube was left for an average of 2.8 days (1-10) with a smooth postoperative course.
Recently, the tubeless approach showed less cost, postoperative pain, hospital stay and earlier return to normal activities than standard PNL [36].
The goal of any surgical stone procedure is complete stone removal. Although the single procedure SFR for PNL is high [37,38], the likelihood of residual fragments for large renal calculi is as high as 67%, using strict CT criteria [39].
Any 4mm residual fragments can be safely left behind after PCNL [40-42]. Postprocedural imaging to detect residual stone burden typically includes plain films, US, CT, and/or antegrade nephrostomy-gram. CT is the optimal post-PCNL imaging modality to detect residual fragments [39].
In this series, cases with residual fragments ≥4mm were considered a failure. Post-operative control KUB films were done in most cases. Ultrasonography and/or NCCT were done in selected patients (lucent stones).
Multiple studies reported hospital stays of 2-7 days post-PNL for large renal stones [28,30]. This was ominously related to the stone burden. On the other hand, Xue and his colleagues [43] stated that large renal stone size was statistically significantly associated with increased mean operative time but not with increased hospitalization.
In our series, an average of 3.6 days (2-21) was reported for the hospital stay. It demonstrated a significant relation with SSA.
Complication rates reported in the literatures associated with PNL ranged from 0-32% [27,28,30,44]. They include extravasation, the need for transfusion, and fever. Higher rates were reported when multiple tracts were needed [26,45,46].
In our study, we reported a total complication rate of 8.3% and all were managed conservatively. A significant relation was recorded with multiple tracts and multiple sessions. No significant relation was found with SSA, complexity, stone site, operative time or nephrostomy tube duration.
Epidural anaesthesia (EA) is a safe alternative to general anaesthesia (GA) for PNL with better pain relief, less PONV and less hospital stay. Hypotension due to sympathetic blockade is always a possibility. Postoperative shivering is higher in EA patients [47]. Patients' and surgeons' satisfaction is higher in GA cases [48]. EA has lower rates of postoperative fever [49], lower fluoroscopy, and time and fewer post-operative complication rates [50].
In our series, EA cases were used in 15% of PNL sessions. They showed less PONV and need postoperative analgesia. They also represented fewer patients' and surgeons' contentment (patient awareness and mobility).
CONCLUSION
The propagation of minimally invasive PNL was developed to reduce the morbidity and mortality associated with open renal surgery but still represents the most morbid of the minimally invasive surgical modalities for renal stone removal.
However, in recent years, efforts to reduce morbidity and increase the effectiveness and efficiency of the procedure are developing. In particular, micro and ultra-mini techniques are in their infancy and require further investigation. Also, efforts to increase the SFR of retrograde intra-renal surgery (RIRS) and flexible ureteroscopy (FURS) are put forth.
Both GA and EA are effective and safe in PNL. EA has fewer complications and lower consumption of postoperative analgesia. However, GA provides more satisfaction for patients and surgeons.
REFERENCES
- Fernström I, Johansson B. (1976). Percutaneous pyelolithotomy. A new extraction technique. Scand J Urol Nephrol. 10(3):257-259.
- Ghani KR, Andonian S, Bultitude M, Desai M, Giusti G, Okhunov Z, et al. (2016). Percutaneous Nephrolithotomy: Update, Trends, and Future Directions. Eur Urol. 70(2):382-396.
- Tiselius HG. (2008). How efficient is extracorporeal shockwave lithotripsy with modern lithotripters for removal of ureteral stones? J Endourol. 22(2):249-255.
- Bandi G, Meiners RJ, Pickhardt PJ, Nakada SY. (2009). Stone measurement by volumetric three-dimensional computed tomography for predicting the outcome after extracorporeal shock wave lithotripsy. BJU Int. 103(4):524-528.
- Lam HS, Lingeman JE, Russo R, Chua GT. (1992). Stone surface area determination techniques: a unifying concept of staghorn stone burden assessment. J Urol. 148(3 Pt 2):1026-1029.
- Türk C, Petřík A, Sarica K, Seitz C, Skolarikos A, Straub M, et al. (2016). EAU Guidelines on Interventional Treatment for Urolithiasis. Eur Urol. 69(3):475-482.
- Antonelli JA, Pearle MS. (2013). Advances in percutaneous nephrolithotomy. Urol Clin North Am. 40(1):99-113.
- Pearle MS, Nadler R, Bercowsky E, Chen C, Dunn M, Figenshau RS, et al. (2001). Prospective randomized trial comparing shock wave lithotripsy and ureteroscopy for management of distal ureteral calculi. J Urol. 166(4):1255-1260.
- Li S, Liu TZ, Wang XH, Zeng XT, Zeng G, Yang ZH, et al. (2014). Randomized controlled trial comparing retroperitoneal laparoscopic pyelolithotomy versus percutaneous nephrolithotomy for the treatment of large renal pelvic calculi: a pilot study. J Endourol. 8(8):946-950.
- Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. (2016). Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART II. J Urol. 96(4):1161-1169.
- Khalaf I, Salih E, El-Mallah E, Farghal S, Abdel-Raouf A. (2013). The outcome of open renal stone surgery calls for limitation of its use: A single institution experience. African J Urol. 19(2):58-65.
- Kukreja R. (2011). PCNL Monotherapy for Complex Renal Calculi. Urology. 78(Suppl 3A):S104.
- Armitage JN, Irving SO, Burgess NA, British Association of Urological Surgeons Section of Endourology. (2012). Percutaneous nephrolithotomy in the United kingdom: results of a prospective data registry. Eur Urol. 61(6):1188-1193.
- Rassweiler JJ, Renner C, Eisenberger F. (2000). The management of complex renal stones. BJU Int. 86(8):919-928.
- Al-Kohlany KM, Shokeir AA, Mosbah A, Mohsen T, Shoma AM, Eraky I, et al. (2005). Treatment of complete staghorn stones: a prospective randomized comparison of open surgery versus percutaneous nephrolithotomy. J Urol. 173(2):469-473.
- Assimos DG, Boyce WH, Harrison LH, McCullough DL, Kroovand RL, Sweat KR. (1989). The role of open stone surgery since extracorporeal shock wave lithotripsy. J Urol. 142(2 Pt 1):263-267.
- Segura JW. (1990). Current surgical approaches to nephrolithiasis. Endocrinol Metab Clin North Am. 19(4):919-935.
- Paik ML, Wainstein MA, Spirnak JP, Hampel N, Resnick MI. (1998). Current indications for open stone surgery in the treatment of renal and ureteral calculi. J Urol. 159(2):374-378.
- Rocco F, Casu M, Carmignani L, Trinchieri A, Mandressi A, Larcher P, et al. (1998). Long-term results of intrarenal surgery for branched calculi: is such surgery still valid? Br J Urol. 81(6):796-800.
- El-Husseiny T, Buchholz N. (2012). The role of open stone surgery. Arab J Urol. 10(3):284-288.
- Netto NR Jr, Ikonomidis J, Ikari O, Claro JA. (2005). Comparative study of percutaneous access for staghorn calculi. Urology. 65(4):659-662.
- Kukreja R, Desai M, Patel S, Bapat S, Desai M. (2004). Factors affecting blood loss during percutaneous nephrolithotomy: prospective study. J Endourol. 18(8):715-722.
- Ganpule AP, Desai M. (2008). Management of the staghorn calculus: multiple-tract versus single-tract percutaneous nephrolithotomy. Curr Opin Urol. 18(2):220-223.
- Desai M, Jain P, Ganpule A, Sabnis R, Patel S, Shrivastav P. (2009). Developments in technique and technology: the effect on the results of percutaneous nephrolithotomy for staghorn calculi. BJU Int. 104(4):542-548.
- El-Nahas AR, Shokeir AA, El-Assmy AM, Mohsen T, Shoma AM, Eraky I, et al. (2007). Post-percutaneous nephrolithotomy extensive hemorrhage: a study of risk factors. J Urol. 177(2):576-579.
- Mousavi-Bahar SH, Mehrabi S, Moslemi MK. (2011). Percutaneous nephrolithotomy complications in 671 consecutive patients: a single-center experience. Urol J. 8(4):271-276.
- Valdivia JG, Scarpa RM, Duvdevani M, Gross AJ, Nadler RB, Nutahara K, et al. (2011). Supine versus prone position during percutaneous nephrolithotomy: a report from the clinical research office of the endourological society percutaneous nephrolithotomy global study. J Endourol. 25(10):1619-1625.
- Wang Y, Wang Y, Yao Y, Xu N, Zhang H, Chen Q, et al. (2013). Prone versus modified supine position in percutaneous nephrolithotomy: a prospective randomized study. Int J Med Sci. 10(11):1518-1523.
- Schmidt S, Miernik A. (2015). Extrakorporale Stoßwellenlithotripsie (ESWL) vs. perkutane Nephrolithotomie (PCNL) oder retrograde intrarenale Chirurgie (RIRS) bei Harnsteinen [Extracorporeal shock wave lithotripsy (ESWL) versus percutaneous nephrolithotomy (PCNL) or retrograde intrarenal surgery (RIRS) for kidney stones]. Urologe A. 54(9):1283-1286.
- Astroza G, Lipkin M, Neisius A, Preminger G, De Sio M, Sodha H, et al. (2013). Effect of supine vs prone position on outcomes of percutaneous nephrolithotomy in staghorn calculi: results from the Clinical Research Office of the Endourology Society Study. Urology. 82(6):1240-1244.
- Osman M, Wendt-Nordahl G, Heger K, Michel MS, Alken P, Knoll T. (2005). Percutaneous nephrolithotomy with ultrasonography-guided renal access: experience from over 300 cases. BJU Int. 96(6):875-878.
- Hamamoto S, Yasui T, Okada A, Taguchi K, Kawai N, Ando R, et al. (2014). Endoscopic combined intrarenal surgery for large calculi: simultaneous use of flexible ureteroscopy and mini-percutaneous nephrolithotomy overcomes the disadvantageous of percutaneous nephrolithotomy monotherapy. J Endourol. 28(1):28-33.
- Bellman GC, Davidoff R, Candela J, Gerspach J, Kurtz S, Stout L. (1997). Tubeless percutaneous renal surgery. J Urol. 157(5):1578-1582.
- Maheshwari PN, Andankar MG, Bansal M. (2000). Nephrostomy tube after percutaneous nephrolithotomy: large-bore or pigtail catheter? J Endourol. 14(9):735-737.
- Pietrow PK, Auge BK, Lallas CD, Santa-Cruz RW, Newman GE, Albala DM, et al. (2003). Pain after percutaneous nephrolithotomy: impact of nephrostomy tube size. J Endourol. 17(6):411-414.
- Zilberman DE, Lipkin ME, de la Rosette JJ, Ferrandino MN, Mamoulakis C, Laguna MP, et al. (2010). Tubeless percutaneous nephrolithotomy--the new standard of care? J Urol. 184(4):1261-1266.
- Deem S, Defade B, Modak A, Emmett M, Martinez F, Davalos J. (2011). Percutaneous nephrolithotomy versus extracorporeal shock wave lithotripsy for moderate sized kidney stones. Urology. 78(4):739-743.
- Albala DM, Assimos DG, Clayman RV, Denstedt JD, Grasso M, Gutierrez-Aceves J, et al. (2001). Lower pole I: a prospective randomized trial of extracorporeal shock wave lithotripsy and percutaneous nephrostolithotomy for lower pole nephrolithiasis-initial results. J Urol. 166(6):2072-2080.
- Pearle MS, Watamull LM, Mullican MA. (1999). Sensitivity of noncontrast helical computerized tomography and plain film radiography compared to flexible nephroscopy for detecting residual fragments after percutaneous nephrostolithotomy. J Urol. 162(1):23-26.
- Portis AJ, Laliberte MA, Holtz C, Ma W, Rosenberg MS, Bretzke CA. (2008). Confident intraoperative decision making during percutaneous nephrolithotomy: does this patient need a second look? Urology. 71(2):218-222.
- Raman JD, Bagrodia A, Gupta A, Bensalah K, Cadeddu JA, Lotan Y, et al. (2009). Natural history of residual fragments following percutaneous nephrostolithotomy. J Urol. 181(3):1163-1168.
- Raman JD, Bagrodia A, Bensalah K, Pearle MS, Lotan Y. (2010). Residual fragments after percutaneous nephrolithotomy: cost comparison of immediate second look flexible nephroscopy versus expectant management. J Urol. 183(1):188-193.
- Xue W, Pacik D, Boellaard W, Breda A, Botoca M, Rassweiler J, et al. (2012). Management of single large nonstaghorn renal stones in the CROES PCNL global study. J Urol. 187(4):1293-1297.
- Al-Dessoukey AA, Moussa AS, Abdelbary AM, Zayed A, Abdallah R, Elderwy AA, et al. (2014). Percutaneous nephrolithotomy in the oblique supine lithotomy position and prone position: a comparative study. J Endourol. 28(9):1058-1063.
- Michel MS, Trojan L, Rassweiler JJ. (2007). Complications in percutaneous nephrolithotomy. Eur Urol. 51(4):899-906.
- Tefekli A, Ali Karadag M, Tepeler K, Sari E, Berberoglu Y, Baykal M, et al. (2008). Classification of percutaneous nephrolithotomy complications using the modified clavien grading system: looking for a standard. Eur Urol. 53(1):184-190.
- Virkar ND, Patkar GA, Rohit R, Tendolkar BA. (2016). A comparative study of combined spinal epidural anaesthesia and general anaesthesia in patients undergoing percutaneous nephrolithotomy. Int J Res Med Sci. 4(9):3760-3767.
- Moawad HS, El Hefnawy AS, Spinal VS. (2015). General anaesthesia for percutaneous nephrolithotomy: A prospective randomized trial. Egy J Anesthesia. 31:71-75.
- Kim SS, Lee JW, Yu JH, Sung LH, Chung JY, Noh CH. (2013). Percutaneous nephrolithotomy: comparison of the efficacies and feasibilities of regional and general anesthesia. Korean J Urol. 54(12):846-850.
- Cicek T, Gonulalan U, Dogan R, Kosan M, Istanbulluoglu O, Gonen M, et al. (2014). Spinal anesthesia is an efficient and safe anesthetic method for percutaneous nephrolithotomy. Urology. 83(1):50-55.