Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2022
Location-Based Surgical Approaches for Orbital Tumor Resection
Tadaaki Morotomi1*, Narihiko Hirano1, Yasuhiro Sanada2, Mitsugu Fujita3, Koji Niwa4
1Department of Plastic and Reconstructive Surgery, Kindai University Faculty of Medicine, Osaka, Japan.
2Department of Neurosurgery, Kindai University Faculty of Medicine, Osaka, Japan.
3Center for Medical Education and Clinical Training, Kindai University Faculty of Medicine, Osaka, Japan.
4Nagumo Clinic Osaka, Osaka, Japan.
*Corresponding author: Tadaaki Morotomi, Department of Plastic and Reconstructive Surgery, Kindai University, Faculty of Medicine, Osaka, Japan. Tel: +81-72-366-0221, E-mail: [email protected]
Received Date: April 08, 2022
Published Date: May 04, 2022
Citation: Tadaaki Morotomi, et al. (2022). Location-Based Surgical Approaches for Orbital Tumor Resection. Mathews J Ophthamol. 7(1):27.
Copyright: Tadaaki Morotomi, et al. © (2022). This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ABSTRACT
Purpose: We investigated the site of tumor development, tumor tissue morphology, surgical approach, and method of selection and indications for a particular surgical method in patients who underwent intraorbital tumor excision. Methods: Surgical methods employed for orbital tumors at our facility between January 2010 and December 2021 were investigated. The relationship between the site of tumor development and surgical approaches, including osteotomy, was investigated. Results: The study included 92 patients, of whom 35 required osteotomy. Superficial orbital tumors were excised using a percutaneous or transconjunctival approach. Craniotomy was necessary to excise deep orbital tumors that developed above the optic nerve. Tumors that developed on the lateral side of the optic nerve were excised using lateral orbitotomy without craniotomy. Deep orbital tumors that developed on the medial and lower sides were excised by extending orbital osteotomy to adjacent sites as needed, for example, a combination of lateral orbitotomy and inferior rim osteotomy. Conclusions: Deep tumors extending to the orbital apex located in the upper and medial upper parts of the optic nerve require craniotomy, but other tumors can be excised under direct vision using single osteotomy or concomitant osteotomy at several sites, as needed. Keywords: Orbital tumor; Intraorbital tumors; Orbital surgery; Surgical approach; Endoscopic orbital surgery
INTRODUCTION
The volume of the orbit is approximately 25 mL, and comprises the eyeball, optic nerve, extraocular muscles, arteries and veins distributed in a complex manner, peripheral nerves, lacrimal gland, fat, and fibrous septum. Therefore, intraorbital tumors can have diverse origins, and thorough knowledge of the anatomy and planning a surgical approach corresponding with the tumor characteristics are important. In our department, we have determined an appropriate surgical approach to prepare a favorable surgical field that could prevent complications such as accessory injuries, corresponding to each case, including craniotomy, in cooperation with the neurosurgery department depending on the site of development of the tumor. Representative approaches to orbital tumors include the anterior approach via the palpebral skin (through the orbital septum), lateral approach (through the lateral orbital wall, Krönelein method [1], and transcranial approach through bilateral coronal sections in which the surgical field is accessed via orbital rim osteotomy or craniotomy. In this study, we investigated the site of tumor development, surgical approach, and method of selection and indications for a particular surgical method in patients who underwent intraorbital tumor excision at our department.
METHODS
We included 92 patients with intraorbital tumors who underwent surgical excision at our department from January 2011 to December 2021. Sex, site of tumor development, pathological diagnosis, and surgical approach were investigated.
In accordance with the regulations set forth by Human Investigations Committee of the Kindai University Faculty of Medicine, informed consent was obtained from all adults and from a parent or guardian of all subjects of less than 18 years of age.
RESULTS
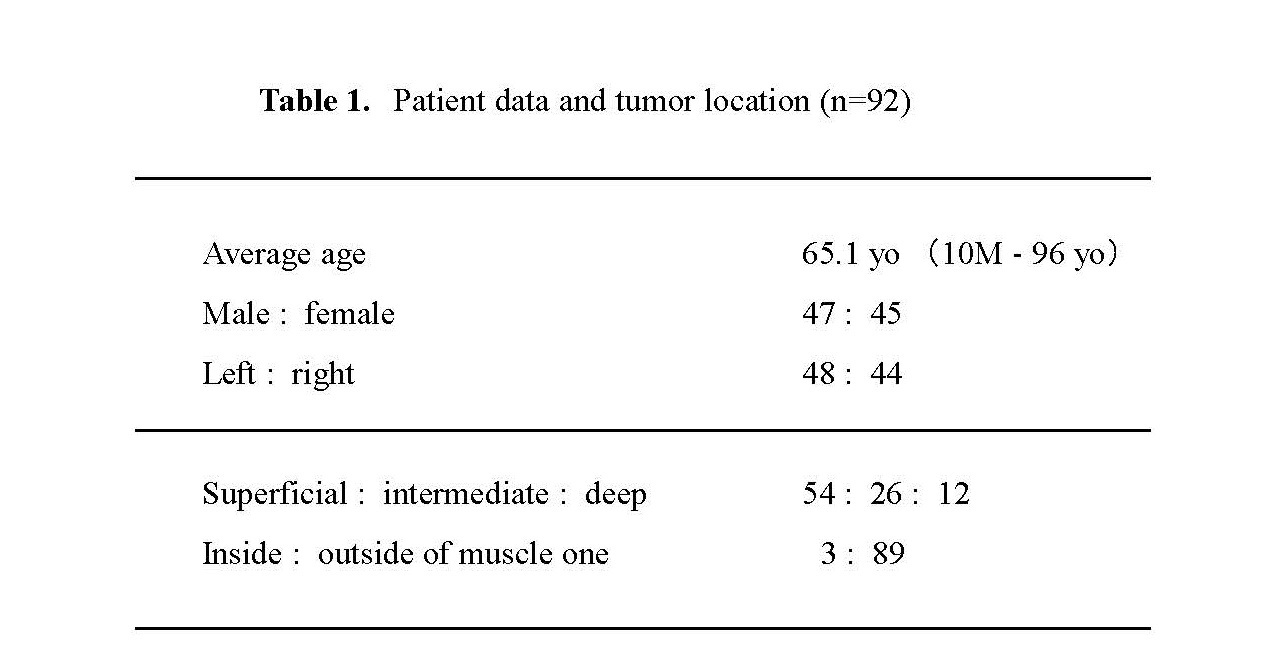
The mean age of the patients was 65.1 years (10 months–96 years), and 47 and 45 patients were male and female, respectively. The affected sides were the left and right in 48 and 44 patients, respectively. Tumor location was classified according to tumor depth (superficial, intermediate, and deep) and direction (upper/lower and medial/lateral with combinations) in the orbit, as shown in Figure 1.
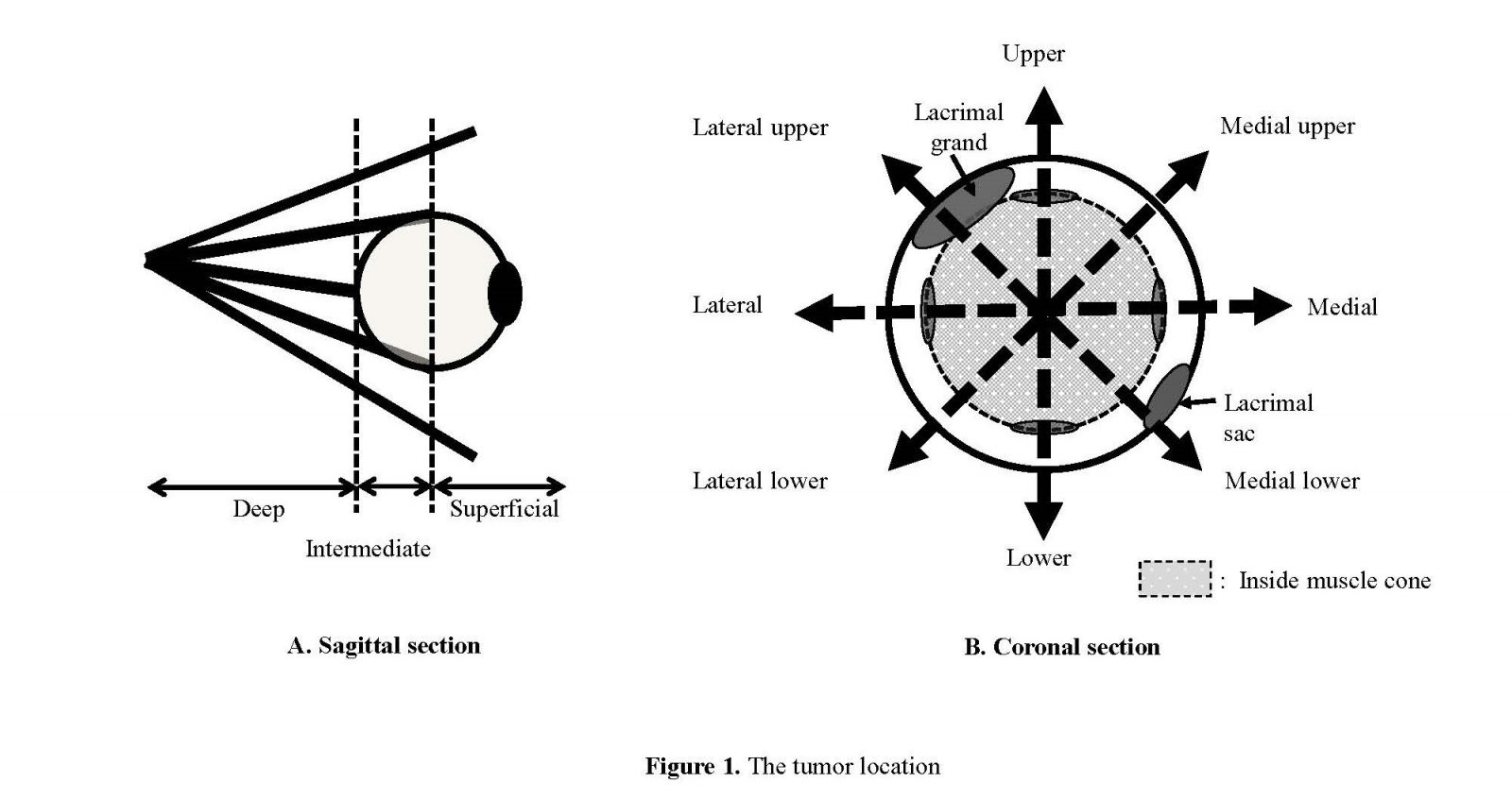
Fig 1: The tumor location: Tumor location was classified according to tumor depth (superficial, intermediate, and deep) and direction (upper/lower and medial/lateral with combinations) in the orbit, and inside or outside the muscle cone.
For the surgical approach, coronal sections of the head and orbitotomy (Fig 2.) were employed, depending on the case.
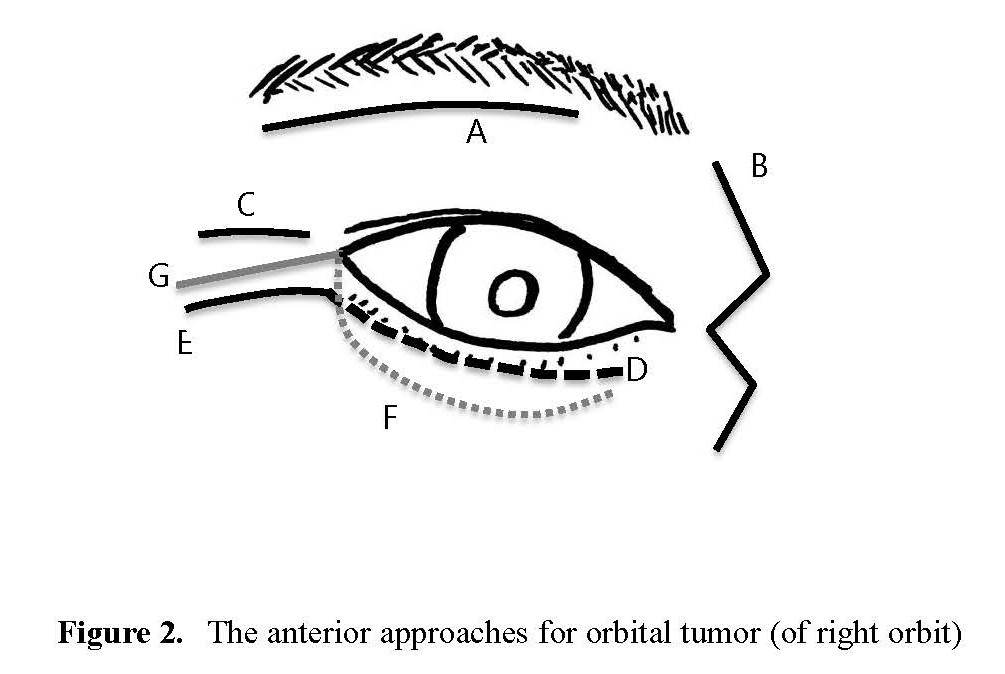
Fig. 2: The anterior approaches for orbital tumor (of right orbit), A: upper eyelid incision, B: medial incision, C: lateral incision, D: lower eyelid incision (subciliary incision), E: D with lateral canthal incision, F: incision of the lower palpebral conjunctiva, G: F with lateral canthal incision
The tumor depth was superficial, intermediate, and deep in 54, 26, and 12 patients, respectively. Tumors developed in and outside the muscle cone in 3 and 89 patients, respectively (Table 1.).
The tumor was located in the upper part of the orbit in 23 patients, upper medial side in 7, medial side in 6, lower medial side in 3, lower side in 13, lower lateral side in 5, lateral side in 8, and upper lateral side in 27 patients. Regarding skin incision in the orbital region, an incision was made in the upper eyelid in 50 patients, on the medial side of the orbit in 8, in the lateral canthal region in 2, lower eyelid in 14, lower eyelid with lateral canthus incision in 2, lower palpebral conjunctiva in 2, and lower palpebral conjunctiva with the lateral canthus in 4 patients (Table 2.).
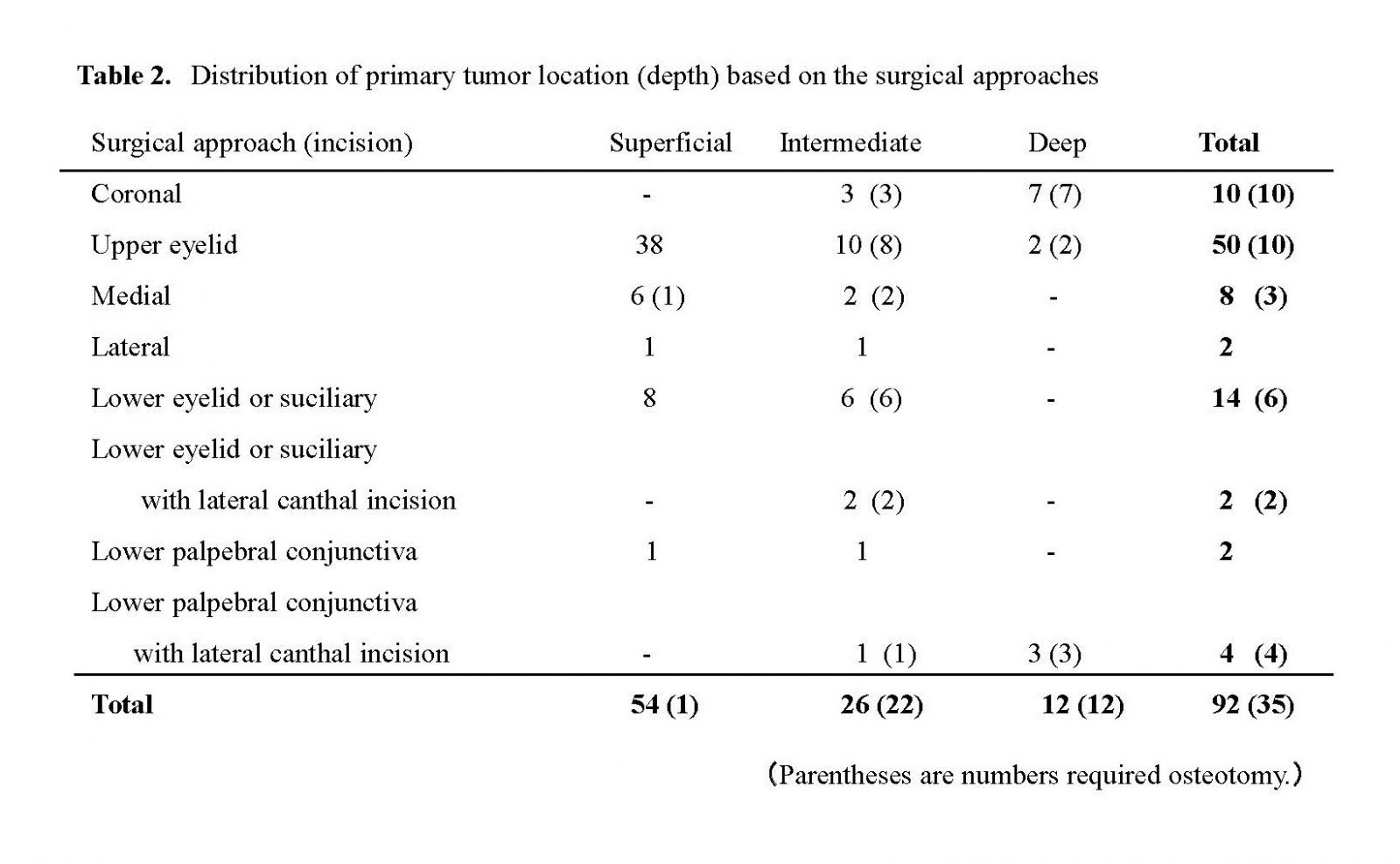
A coronal incision was made in 10 patients. The surgical approach for and depth of the tumor in each case are listed in Table 2. Osteotomy was performed to prepare the surgical field in 35 (38.0%) of 92 patients.
The details of the primary surgical approach are described herein:
*Coronal incision: This approach was used in 10 patients. Of these, the transcranial approach by craniotomy was employed in 2 patients, and the tumor location/depth/direction was in the muscle cone/intermediate/upper part of the orbit and outside the muscle cone/deep/upper part of the orbit, respectively. Superior orbital rim osteotomy was performed in 2 patients in whom the tumor location/depth/direction was outside the muscle cone/intermediate/upper part. Lateral orbitotomy was performed in 4 patients in whom the tumor location/depth/direction was outside the muscle cone/deep/lateral upper part of the orbit.
*Upper eyelid incision: Superior orbital rim osteotomy was performed in 8 patients.
*Lower eyelid (subciliary) incision: This approach was applied in 14 patients (including 6 patients who underwent orbital rim osteotomy), mostly for tumors primarily located in the lower part.
*Lower eyelid (subciliary) incision with lateral canthal incision: Inferior orbital rim osteotomy was performed for tumors located outside the muscle cone, at an intermediate depth, and in the lower part.
*Incision of the lower palpebral conjunctiva with lateral canthal incision: This approach was used in 4 patients. Of these, lateral orbitotomy was performed in 2 patients, and the tumor location/depth/direction was in the muscle cone/deep/lateral lower part and outside the muscle cone/intermediate/lateral lower part, respectively. In the other 2 patients, lateral orbitotomy and inferior rim osteotomy were concomitantly performed, and the location/depth/direction was outside the muscle cone/deep/lower and medial parts, respectively.
Osteotomy was necessary in 1.8% (1/54) of the tumors located superficially, whereas it was performed in approximately 84.1% (22/26) of the tumors located at an intermediate depth (Table 2). For intermediate-depth tumors, a lateral orbital incision was used for tumors in the inferior and lateral inferior parts, superior orbital margin osteotomy was performed for tumors in the medial superior and superior parts, and coronal incision approach was required for tumors in the superior parts of the orbit. Osteotomy via a transcranial approach was performed for all tumors (12/12) located deep in the orbit in 2 patients, employing lateral or upper rim orbitotomy in 7, and a combination of lateral orbitotomy and inferior rim osteotomy in 3 patients.
The pathological diagnoses of the patients are shown in Table 3.
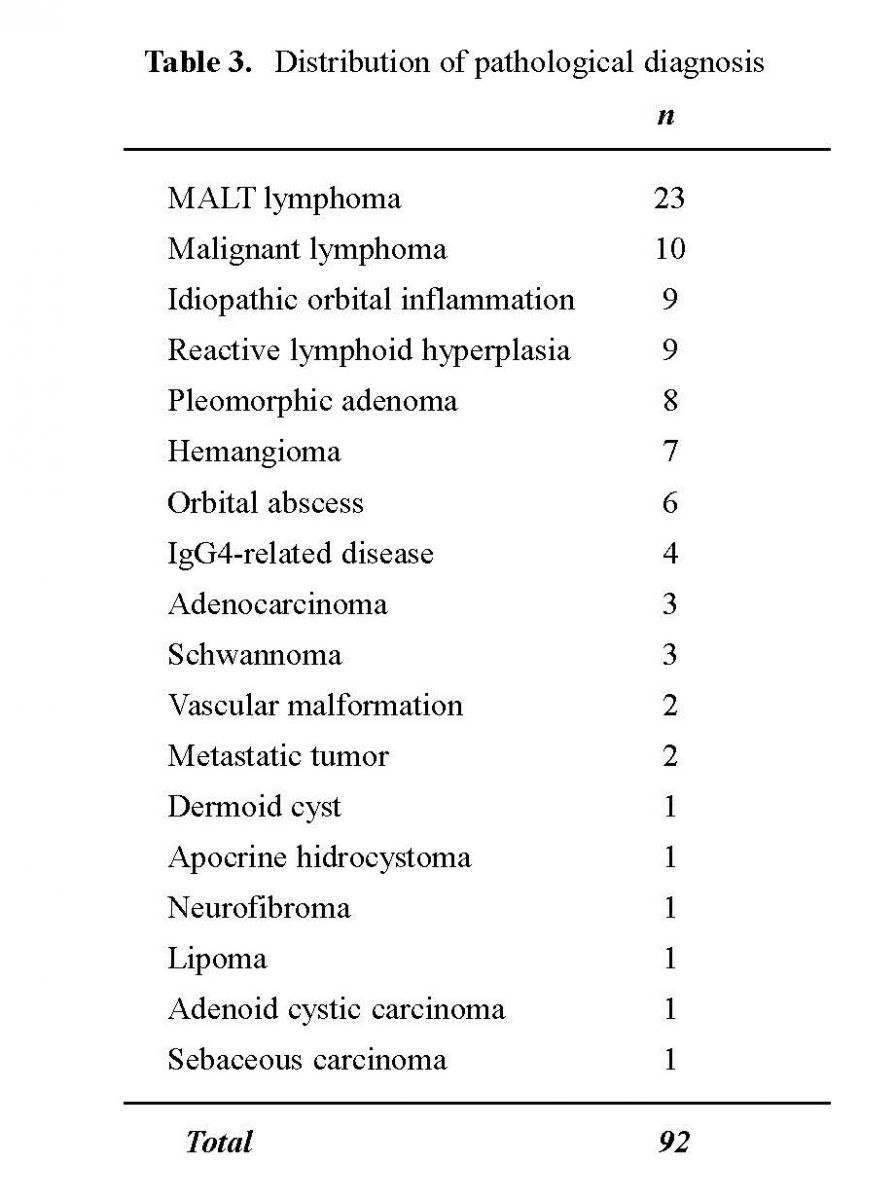
Lymphatic system lesions were evident in 42 (45.7%) of 92 patients. Malignant tumors were found in 40 (31.1%) patients. Of these, MALT lymphoma was evident in 23 patients, malignant lymphoma in 10, adenocarcinoma in 3, metastatic tumor in 2, adenoid cystic carcinoma in 1, and sebaceous carcinoma in 1 patient.
Representative case presentations
Case 1 (Fig 3.): A 67-year-old man was referred to our department with the chief complaints of ocular deviation and diplopia. A deeply located tumor was evident in the upper lateral part of the left orbit. The tumor was approached through a coronal section of the head for craniotomy. The temporalis muscle was detached from the temporal bone, and lateral orbitotomy was performed to excise the tumor. The osteotomy line was determined concomitantly using navigation during surgery. A histopathological diagnosis was venous hemangioma. After surgery, no complications occurred and diplopia improved.
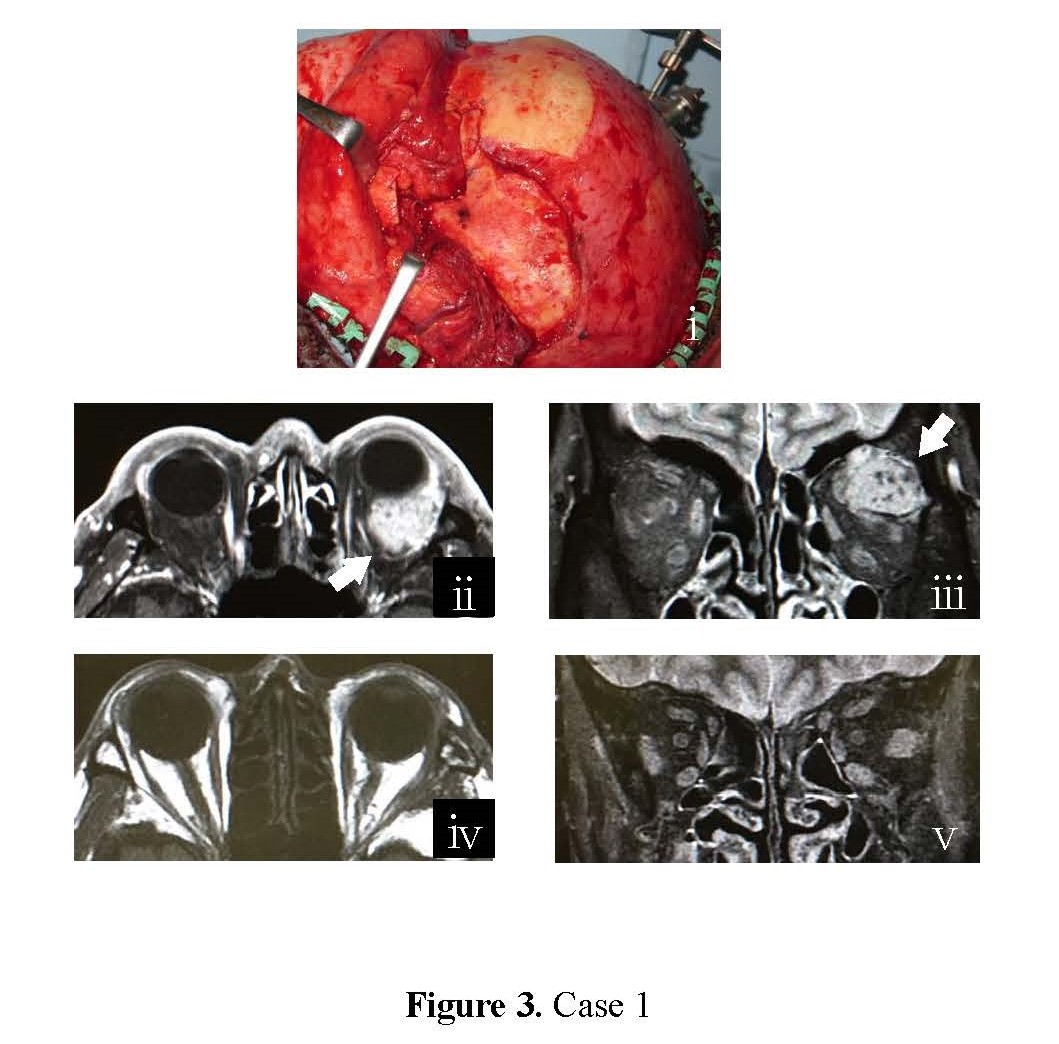
Fig 3: Case 1: The tumor was approached through coronal incision in preparation for the necessity of craniotomy. i) Lateral rim osteotomy by using coronal incision, ii) preoperative MRI (horizontal dislocation, arrow shows tumor), iii) preoperative MRI (coronal dislocation), iv) postoperative MRI (12 months after surgery, horizontal dislocation), v) postoperative MRI (12 months after surgery, coronal dislocation)
Case 2 (Fig 4.): A 38-year-old woman was referred to our department with complaints of visual disorders, ocular deviation, strabismus, eye movement disorder, and diplopia. A deeply located tumor was evident at the apex of the right orbit, on the medial side of the optic nerve. The tumor was approached through a combination of transconjunctival and lateral canthal incisions. Lateral and inferior rim osteotomies were performed in the orbit, and the orbital floor was exposed. The orbital apex on the medial side was approached by excluding the eyeball laterally and securing the visual field from the maxillary sinus, and the tumor was excised. A histopathological diagnosis was schwannoma. After the surgery, the visual disorder improved slightly, but the strabismus persisted.
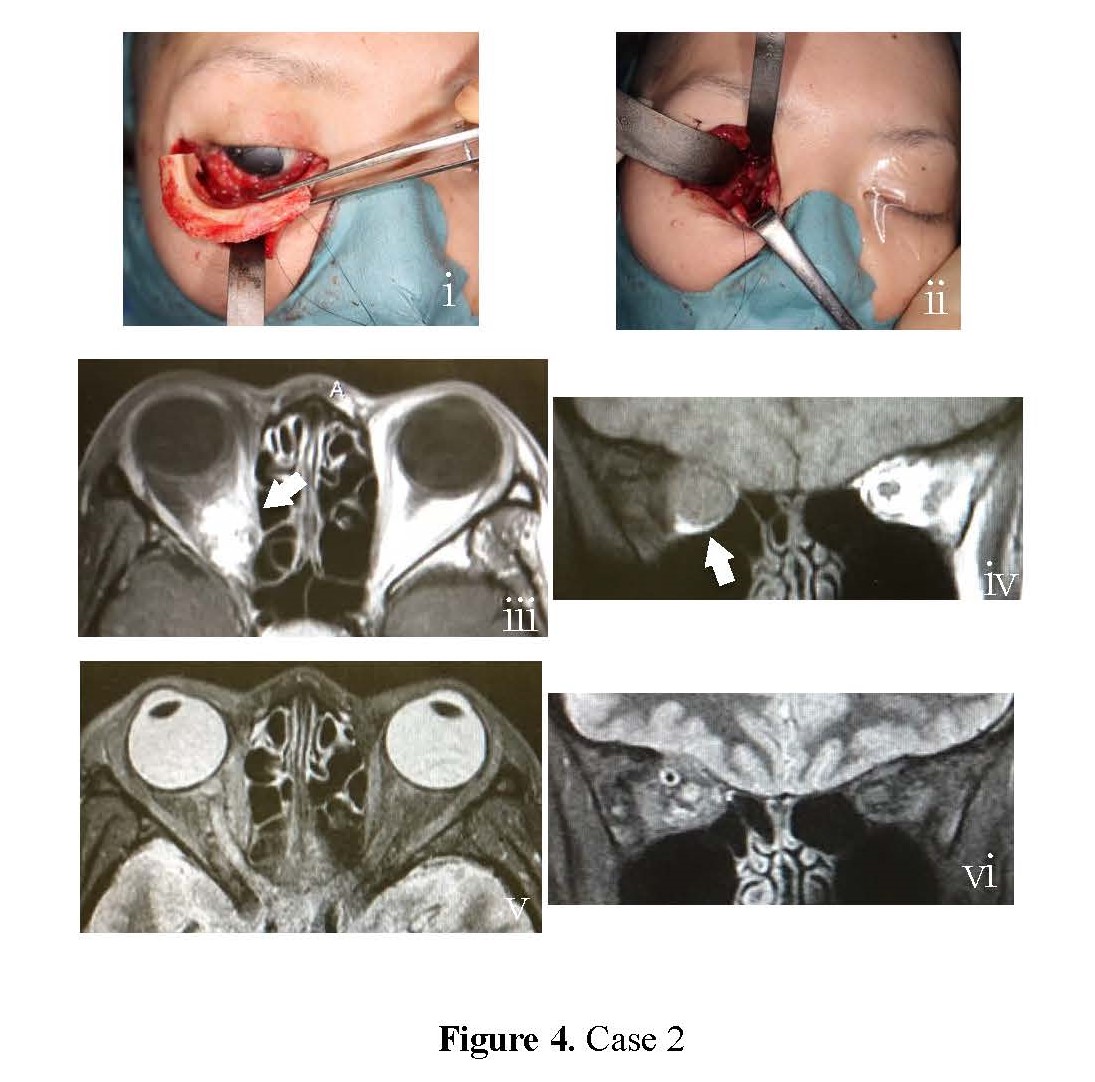
Fig 4: Case 2: Tumor located in deep, medial area was resected by using osteotomy of lateral and lower orbital rim. i) lateral and lower rim osteotomy, ii) an operative field securing of the orbital apex on the medial area, iii) preoperative MRI (horizontal dislocation, arrow shows tumor), iv) preoperative MRI (coronal dislocation), v) postoperative MRI (6 months after surgery, horizontal dislocation), vi) postoperative MRI (6 months after surgery, coronal dislocation)
DISCUSSION
Intraorbital tumors exhibit diverse histological findings. The intraconal type (tumors arising in the muscle cone) includes optic nerve meningioma, optic nerve glioma, schwannoma, and cavernous hemangioma, and the extraconal type (tumors arising outside the muscle cone) includes lacrimal gland tumor and meningioma1. In the present study, lymphatic system tumors occurred most frequently and accounted for approximately 45% of the tumors (Table 3.). The IgG4-related disease, proposed in 2001, has recently been attracting attention [2], but the ratio of IgG4-related disease was 7.7%, which may be because we started data collection in 2010.
An accurate preoperative determination of the histologic type and location of the tumor is important for planning surgical excision, which include relationship with the muscle cone, depth, direction, and extension to the orbital apex [3]. Nerve injury by surgical operation and postoperative intraorbital hematoma, which is a serious postoperative complication [4], can be avoided by a thorough knowledge of the anatomy. Most tumors that develop in the superficial region of the orbit can be excised through a percutaneous anterior approach; however, selecting the optimal approach is difficult in cases of tumors located at intermediate and deep sites, according to the classification of tumor depth used in this study. Assumptions pertaining to the need for orbitotomy alone or the transcranial method are often necessary.
The skin incision line is determined according to the tumor location, depending on its anterior or posterior location in the orbit, as described in a previous study [5]. We employed a simplified skin incision line, as shown in Figure 2. Generally, the types of osteotomy required for tumors located posteriorly in the orbit are as follows: 1) lateral orbitotomy (Krönelein method), 2) medial orbitotomy (through the Lynch incision), 3) superior rim osteotomy (transcranial method), and 4) inferior rim osteotomy (utilizing the maxillary sinus) [6]. Procedures based on tumor location have also been reported: (1) lateral orbitotomy (including bone removal) for tumors at the orbital apex on the lateral side of the optic nerve, (2) a combination of the transcranial method or lateral orbitotomy with medial orbitotomy for tumors at the orbital apex around the optic nerve except the lateral side, and (3) the transcranial approach for tumors involving the skull from the orbital apex [3]. Superficially located tumors did not require osteotomy in this study, but it may be required for tumors located at intermediate and deep sites. Since the method of determining tumor depth in this study (especially at the orbital apex) is different from that in previous reports, we investigated the procedure and significance of each type of osteotomy through a literature review.
Lateral orbitotomy was initially reported by Krönelein et al. in 1891 and is still widely used, with or without modifications [7]. Since injury to the extraocular muscles and nerves can be prevented by preparing a wide surgical field, lateral orbitotomy is useful to resect tumors located in the lacrimal fossa and lateral part of the orbit [8], and those at the orbital apex if located on the lateral side [6,9] We also recommend this procedure for the excision of tumors located at deeper and intermediate sites and in the upper lateral, lateral, and lateral lower parts of the orbit.
Under some certain conditions, tumors located in the upper part can also be resected through this approach. Also, combined with a nasal conjunctiva incision, the tumors located in the medial part may also be resected through this approach. However, lateral orbitotomy may not be regularly used for tumors located in the upper and medial parts because of the high risk of injuring the ophthalmic artery and nasociliary, abducent, oculomotor, and optic nerves.
The transcranial approach is employed for tumors located at the orbital apex, superior orbital fissure, and skull because any accessory injury can be prevented by direct visualization of the intraorbital nerves, blood vessels, and muscles [10,11]. This approach is useful for tumors located in deeper sites such as the anterior clinoid process of the sella turcica, superior orbital fissure, and on the medial side of the opening of the optic canal [12]. It is also indicated for tumors located in the muscle cone (especially, the region surrounded by the levator palpebrae superioris, superior oblique, and rectus superior muscles and the optic nerve) and deep tumors located at the orbital apex above the optic nerve. In this regard, the transcranial approach would injure levator palpebrae superioris, the superior lip elevators and superior rectus muscles, which must be thoroughly checked visually to avoid injury. Tumors can be approached from the medial or lateral side of the levator palpebrae superioris muscle [13]. In the 2 patients in whom the transcranial approach was employed, the tumor location/depth/direction were in and outside the muscle cone/intermediate and deep/upper part of the orbit, that is, the cranial side of the optic nerve, respectively. The transcranial approach is indicated for deeply located tumors present on the cranial side of the optic nerve (including the medial, upper, and lateral sides)[6], but we use the transcranial approach only for tumors located in the upper and medial upper sides of the optic nerve because it requires craniotomy, which induces strong surgical stresses.
The transcranial approach is generally selected to approach the medial side of the orbit, that is, for deeply located tumors on the medial side of the optic nerve, but an access route that does not require craniotomy is the one wherein the upper eyelid is vertically transected and the orbit is operated [5,6]. For tumors occupying 50% or more of the orbital volume, in addition to single orbitotomy performed on the lateral or medial side, inferior rim osteotomy is used to push the orbital contents into the maxillary sinus and secure a surgical field, and transection of the lacrimal sac is employed to widen the visual field on the medial side [6]. In addition, lateral rotation of the eyeball by adding lateral orbitotomy is effective for exposing the medial side [5,6]. Although these methods are minimally invasive with regard to the non-necessity of craniotomy, exposure may be insufficient to reach the orbital apex, and approaching the deep part of the tumor may be difficult. We performed osteotomy in the lateral part of the lower rim of the orbit to secure a visual field without craniotomy (Case 2). This method can provide an adequate visual field of the center of the lower orbital rim by en block osteotomy of the lateral orbital wall to prepare an “escape window”, and a tumor in the lower side of the orbit can be dropped into the maxillary sinus through this window to obtain an optimal visual field [14]. Lastly, a tumor located at the lower side of the orbit can be excised through the maxillary sinus using this method [15]. These methods are used to prepare the surgical field for the excision of tumors that develop in the lower side of the orbit; however, in our method, osteotomy is performed up to the lacrimal sac, and not discontinued at the center of the lower rim; when exposure is insufficient, the orbital floor over the medial orbital wall is removed, which will enable the excision of deep tumors located at the orbital apex in the medial and lower sides of the optic nerve without the need for craniotomy. In this type of osteotomy, lateral orbitotomy is performed to prepare a space for the rotation of the eyeball and use inferior rim osteotomy to remove the orbital floor and open the maxillary sinus, through which operation for tumors in the orbital apex on the lower medial side of the orbit can be performed under direct vision.
The protocol for the selection of tumor location-based surgical approaches and need for osteotomy based on our findings are shown in Figure 5.
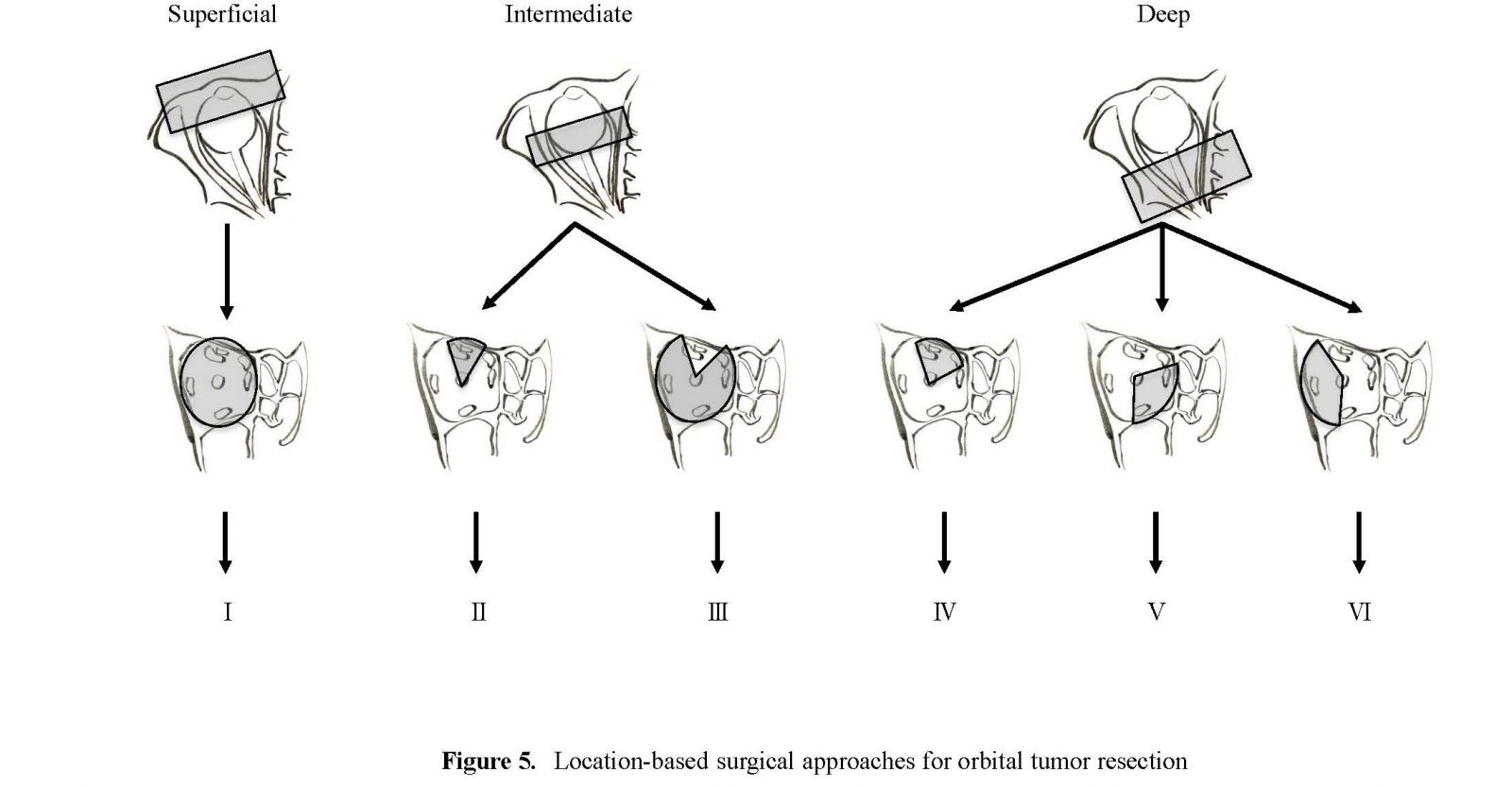
Fig 5: Location-based surgical approaches for orbital tumor resection I) Anterior approach with no osteotomy, II) Anterior approach with upper rim osteotomy, III) Anterior approach with lateral or lower or medial rim osteotomy, IV) Transcranial approach with orbital rim osteotomy, V) Anterior approach with lateral and lower rim osteotomy, VI) Transcranial or anterior approach with lateral rim osteotomy, or lateral and lower rim osteotomy
Figure 5-I shows a superficially located tumor. An incision line corresponding to the tumor location is determined, and the tumor is excised via a percutaneous or transconjunctival anterior approach. Figure 5-II shows a tumor located at an intermediate depth approached using upper blepharotomy or coronal section, and superior orbital rim osteotomy is performed as needed. Figure 5-III shows a tumor located at an intermediate depth, but not involving the upper part of the orbit. It is approached via a coronal section, and extension of the incision from the lower eyelid skin or conjunctiva to the lateral canthus is performed as needed, and the tumor excised using single orbitotomy (lateral side/lower rim/medial side). Figure 5-IV shows a deeply located tumor in the upper or medial upper side, and craniotomy via a transcranial approach is performed through the coronal section. Figure 5-V shows a deeply located tumor in the lower medial side, which is approached through an incision in the lower eyelid or conjunctiva, extending to the lateral canthus or via coronal section as needed. Osteotomy is performed on the lateral side and lower rim of the orbit, as shown in case 2, a wide visual field is secured, and the tumor is operated under direct vision. Figure 5-VI shows tumors developing in the upper lateral, lateral, and lower lateral sides. These are approached through an incision similar to that shown in Figure 5-V and excised using lateral orbitotomy alone or a combination of lateral and inferior rim osteotomies.
Selection of an approach for deeply located tumors may be difficult. In particular, when the lesion is malignant, the choice of surgical approach must consider the pathological nature of the lesion because transcranial and other osteotomy may lead to the spread of the lesion. Surgery for tumors located on the upper side is possible under direct vision through a transcranial approach and for tumors in the medial and lower sides through our approach, which is relatively simple and safe. However, the accuracy of the nasal endoscopic approach has improved, and its usefulness has been reported [16,17]. It may be necessary to investigate the usefulness of the endoscopic approach in patients in addition to direct approaches.
DECLARATIONS
None of the author has a conflict of interest to disclose.
FUNDING
None
CONFLICTS OF INTEREST
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
DATA AVAILABILITY STATEMENT
The data used to support the findings of this study are available from the corresponding author upon request.
ETHICAL STATEMENT
No animals were used in the research, please see the attachment for the human ethics document.
AUTHOR’S CONTRIBUTION
Tadaaki Morotomi make substantial contributions to conception; Narihiko Hirano, and Yasuhiro Sanada and Koji Niwa review the literatures, collect the data, and Tadaaki Morotomidraft the manuscript; Tadaaki Morotomi revise the review; Tadaaki Morotomi gives final approval of the version to be submitted and any revised version.
CONSENT TO PUBLISH
The participants have consented to the submission of the review to the journal.
REFERENCES
- Krönlein RU. (1889). Zur Pathologie und operativen Behandlung der Dermoidzysten der Orbita. Beitr Klin Chir 4:149-163.
- Hamano H, Kawa S, Horiuchi A, H Unno, N Furuya, et al. (2001). High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 344(10):732-738.
- Rubin PA, and Remulla HD. (1996). Surgical methods and approaches in the treatment of orbital disease. Neuroimagings Clinics of North America. 6(1):239-255.
- McCord CD Jr. (1988). Complications of orbital surgery. Otolaryngol Clin. North Am. 21(1):183-188.
- Robert C. Kersten, Jeffrey A. (2006). Duane's Clinical Ophthalmology. Vol 5: Chapter 86. Orbital Surgery, LIPPINCOTT WILLIAMS & WILKINS.
- Osguthorpe JD, Saunders RA, and Adkins WY. (1983). Evaluation of and access to posterior orbital tumors. Laryngoscope. 93(6):766-771.
- Amirjamshidi A, Abbasioun K, Amiri RS, Ali A, Hashemi SMR, et al. (2015). Lateral orbitotomy approach for removing hyperostosing en plaque sphenoid wing meningiomas. Description of surgical strategy and analysis of findings in a series of 88 patients with long-term follow up. Surg Neurol Int. 6:79.
- Bejjani G.K, Cockerham K.P, Kennerdel J.S, and J C Maroon. (2001). A reappraisal of surgery for orbital tumors. Part I: extraorbital approaches. Neurosurg. Focus. 10(5):E2.
- Arai H, Sato K, and Katsuta T. (1996). Lateral approach to intraorbital lesions: anatomic and surgical considerations. Neurosurg. 39(6):1157.
- Brusati R, Goisis M, Biglioli F, Guareschi M, Nucci P, et al. (2007). Surgical approaches to cavernous haemangiomas of the orbit. Br J Oral Maxillofac Surg. 45(6):457-462.
- Brusati R, Biglioli F, Mortini P, Raffaini M, and Goisis M. (2000). Reconstruction of the orbital walls in surgery of the skull base for benign neoplasms. Int J Oral Maxillofac Surg. 29(5):325-330.
- Mariniello G, Maiuri F, de Divitiis E. Bonavolontà G, Tranfa F, et al. (2010). Lateral orbitotomy for removal of sphenoid wing meningiomas invading the orbit. Neurosurgery. 66(6 Suppl Operative):287-292.
- Abuzayed B, Kucukyuruk B, Tanriover N, Zihni Sanus G, Canbaz B, et al.(2012). Transcranial superior orbitotomy for the treatment of intraorbital intraconal tumors: surgical technique and long-term results in single institute. Neurosurg. 35:573-582.
- Kosaka M, Mizoguchi T, Matsunaga K, Fu R, and Nakao Y. (2006). Novel strategy for orbital tumor resection: surgical "displacement" into the maxillary cavity. J Craniofac Surg. 17(6):1251-1258.
- Beriat G.K, Ataç G.K, Kocatürk S, Ezerarslan H, and Erdoğan E. (2013). A simple technique for removal of orbital tumors: transmaxillary approach. Kulak Burun Bogaz Ihtis Derg. 23(5):299-301.
- Campbell A.A, Grob S.R, and Yoon M.K. (2015). Novel Surgical Approaches to the Orbit. Middle East Afr J Ophthalmol. 22(4):435-441.
- Felippu A, Mora R, Guastini L, Peretti G. (2013). Transnasal approach to the orbital apex and cavernous sinus. Ann Otol Rhinol Laryngol. 122(4):254-262.