Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2023
Intimate Partner Violence Screening and Telemedicine Opportunities
Stowe Caroline*
Johns Hopkins University School of Nursing, 3908 Aeries Way, Virginia Beach, VA 23455, USA
*Corresponding author: Stowe Caroline, Johns Hopkins University School of Nursing, 3908 Aeries Way, Virginia Beach, VA 23455, USA, Tel: 8434254377; Email: [email protected].
Received Date: February 13, 2023
Published Date: March 10, 2023
Citation: Stowe C. (2023). Intimate Partner Violence Screening and Telemedicine Opportunities. Mathews J Nurs. 5(1):12.
Copyrights: Stowe C. © (2023).
ABSTRACT
Background: According to the Center for Disease Control, intimate partner violence (IPV) affects millions of people in the United States each year. IPV starts early and continues throughout the lifetime of both men and women. Methods: A group of healthcare providers who provide health care services via telemedicine were exposed to an educational session based on the United States Preventive Task Force (USPSTF) recommendations and then provided with an opportunity to practice what they had learned. It was determined if differences in knowledge after exposure to the session combined with a practice session were significant from pre-test scores. Results: Based on a 100 percent point scale, participants scored an average of 58% before exposure to the educational intervention and an average of 89% after participating. Participants strongly agreed that the program was useful for increasing knowledge of USPSTF recommendations for IPV screening. Conclusion: The educational intervention was effective in increasing competency in IPV screening among women of reproductive age. Post-test findings suggest that the intervention met the goal of increasing provider competency in IPV screening via telemedicine. This quality improvement project can serve as a foundation for IPV screening via telemedicine.
Keywords: Intimate Partner Violence, Telehealth, Telemedicine.
BACKGROUND AND PROBLEM IDENTIFICATION
Intimate partner violence (IPV) is a grave, preventable public health problem and includes sexual and physical violence, stalking and psychological harm inflicted by a current or former partner or spouse [1]. Approximately 1 in 4 women and nearly 1 in 10 men have experienced physical or sexual harm by an intimate partner during their lifetime [1]. Over 43 million women and 38 million men have experienced psychological aggression by an intimate partner in their lifetime [1].
On March 11, 2020, the World Health Organization (WHO) declared a pandemic due to the coronavirus disease 2019 (COVID 2019), and efforts to reduce transmission led to physical and social distancing measures worldwide. This need to decrease transmission also led to cancellation of in-office healthcare visits and accelerated the shift to telemedicine visits.
Research has shown that IPV can escalate during large-scale crises or catastrophes [2]. And with isolation comes fewer opportunities to seek help or safety. This is where telehealth can bridge this gap–and the evidence suggests that telehealth interventions for IPV provide !favorable outcomes with regard to perceived social support, health-related quality of life, adherence to postexposure prophylaxis, violent incidents, safety-promoting behaviors and healthcare use” [3,4]. At the asynchronous telemedicine company where I am employed, a greater than 50% increase in birth control requests and a greater than 100% increase in emergency contraception and STI testing request have been seen. Is there a component of IPV for these individuals and how should one provide the best care for these patients? The value for implementing this project is to follow evidenced based practice guidelines while fulfilling the mission of this company. Because the risk of not addressing this problem is severe–persistent violence, mental health decline and potentially even death.
The United States Preventive Services Task Force (USPSTF) recommends that clinicians screen for intimate partner violence (IPV) in women of reproductive age and provide or refer women who screen positive to ongoing support services (Grade B) [5]. To current knowledge, there are very few reviews on the use of IPV screening in telemedicine. Due to the lack of data on screening for IPV through telemedicine, a systematic review was complete to answer the following question: What are effective training interventions for Healthcare Providers (HCPs) to increase Intimate Partner Violence (IPV) screening?
Definition of Concepts
For the purpose of this review, the following terms are defined. The term intimate partner violence refers to physical violence, sexual violence, psychological aggression, or stalking by a romantic or sexual partner. Intimate partner violence screening refers to the use of a validated screening tool for screening, such as Humiliation, Afraid, Rape, Kick (HARK); Hurt, Insult, Threaten, Scream (HITS); Extended–Hurt, Insult, Threaten, Scream (E-HITS); Partner Violence Screen (PVS); and Woman Abuse Screening Tool (WAST). In this review, the term healthcare provider refers to physicians, registered nurses, physician assistants and advanced practice nurses. The term telehealth or telemedicine refers to the use of technology for communication between the patient and their healthcare provider. This can include a range of telephone, videoconference, and internet-based applications. Finally, the population that is the focus of this review is defined as otherwise healthy women of reproductive age.
Clinical Question
In telemedicine, how does a healthcare provider’s (HCP) understanding of intimate partner violence (IPV) screening affect the HCP’s ability to appropriately screen for IPV?
Recommendations for Practice
The USPSTF recommends that clinicians screen for intimate partner violence in women of reproductive age and provide or refer women who screen positive to ongoing support services (Grade B) [5], so it is imperative that screening occurs - especially through telemedicine as we continue to live through this pandemic. It is clear from the current studies that individuals are open to using telehealth-based opportunities to report IPV and domestic abuse, but there remain concerns regarding confidentiality and the ability of the abused persons to reach out. Guidance is available to help train staff and healthcare professionals, and it must become a priority within the specific practice to ensure this is provided. Further research is imperative to further address healthcare professionals’ knowledge with IPV screening through telehealth modalities.
Theoretical Framework
The Health Belief Model (HBM) guided this project and was developed by social psychologists Hochbaum, Rosenstock and Kegels in the 1950’s. This model attempts to explain and predict health behaviors by focusing on the attitudes and beliefs of individuals. The framework considers the psychosocial, demographic and structural variables that affect health beliefs and perceptions of susceptibility, severity, benefits and barriers to a disease in shaping health behaviors [6]. Originally, there were 4 cognitions associated with this model: perceived susceptibility, perceived benefits, perceived seriousness, and perceived barriers. Additional constructs have been added since these were originally created: cues to action, modifying variables and self-efficacy.
The impetus to make health issues, like intimate partner violence, prominent in a person’s life is vital. An individual also needs to believe there is a perceived threat to their health. If a person is driven and identifies a health threat, they need to believe that a particular health recommendation would be beneficial in reducing the threat [7].
PROJECT DESIGN AND METHODS
This project aimed to increase healthcare providers’ understanding of IPV screening and awareness, provider comfort with validated and available screening tools and subsequently increases IPV screening rates among patients in a telemedicine setting. An educational update via a google document on IPV screening tools was delivered with a pre/post-test to assess the
HCPs ’understanding. These tests were administered immediately before and after reviewing the training session and were used to assess whether there was an increase in the level of knowledge and attitudes regarding IPV screening in telemedicine patients. A Likert-scale was used to evaluate the educational component. The initial questionnaire obtained demographics. The same questions regarding IPV screening and population were asked prior to and after the educational component. To further quantify provider’s understanding, we scheduled a screenshare with five of the providers who completed the educational update to practice screening and providing resources with a test patient. A new policy will be instituted at this clinical site regarding appropriate steps for IPV screening and referral process with resources (i.e. Domestic Violence Hotline + state information (Health Departments, etc). A text expander was created for all providers to use in these situations, and an algorithm created to provide easy to follow step by step guidance.
There are several key stakeholders in this project, including the HCPs evaluating patients for the above services, senior leadership teams to include non-clinical product/design, CEOs and engineers for the telemedicine platforms. The patient populations involved include female patients of reproductive age that can legally access care via a telemedicine platform. There are >400,000 active patients on the Nurx platform and as previously discussed, the kind of care offered includes: birth control, emergency contraception, STI testing, PrEP/PEP, HIV care, migraines, dermatology and HSV care.
The project took place over a 4–5-month period. The educational component with pre/posttest took less than 20 minutes from start to finish. The screenshare with the provider took less than 20 minutes. The estimated IPV lifetime cost was $103,767 per female victim and $23,414 per male victim, or a population economic burden of nearly $3.6 trillion (2014 US$) over victims ’lifetimes, based on 43 million U.S. adults with victimization history [8]. This estimate included $2.1 trillion (59% of total) in medical costs, $1.3 trillion (37%) in lost productivity among victims and perpetrators, $73 billion (2%) in criminal justice activities, and $62 billion (2%) in other costs, including victim property loss or damage [8]. Government sources pay an estimated $1.3 trillion (37%) of the lifetime economic burden.
The GMU IRB deemed this quality improvement project not meeting the requirements of research. Participation in the training was voluntary and information regarding the purpose of the project was provided to participants prior to delivery of the educational intervention.
Authorization was granted from the telehealth platform’s medical director to implement the quality improvement project. All participants received the same information and directions.
RESULTS
20 healthcare providers participated in the educational intervention. The majority of respondents were Nurse Practitioners (40%) followed by Physicians (30%), Physician Assistants (20%), and 1 Registered Nurse (10%) (See Figure 1). 95% of the respondents identified as white, not Hispanic or Latino, while 5% identified as black, Hispanic or Latino (See Figures 2 and 3).
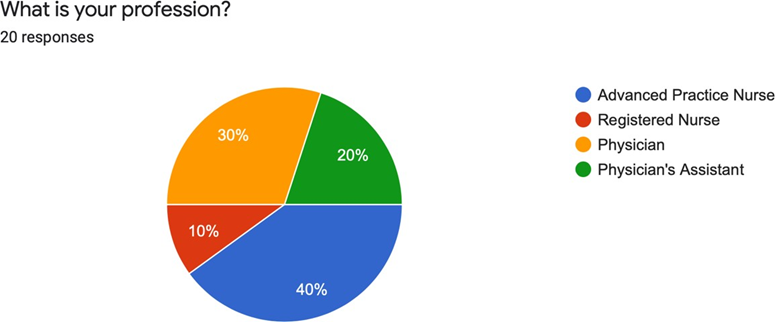
Figure 1. What is your profession?
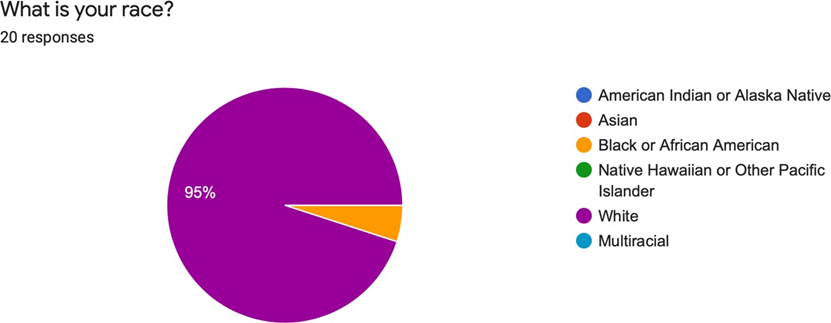
Figure 2. What is your race.
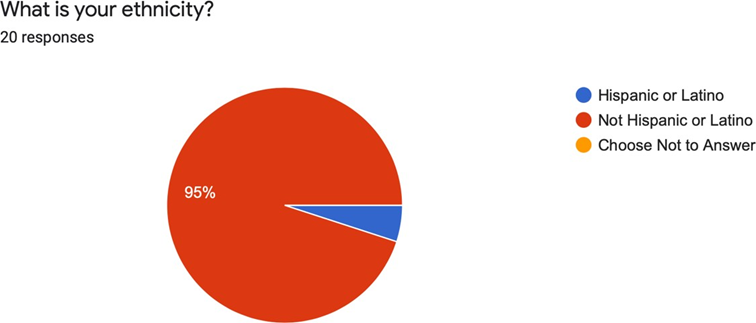
Figure 3. What is your ethnicity?
60% of the respondents report having been in clinical practice for 10 years or greater, with 30% reporting 6-10 years of practice and 10% having practiced for 0-5 years (See Figure 4). This is representative of the current provider pool at Nurx.
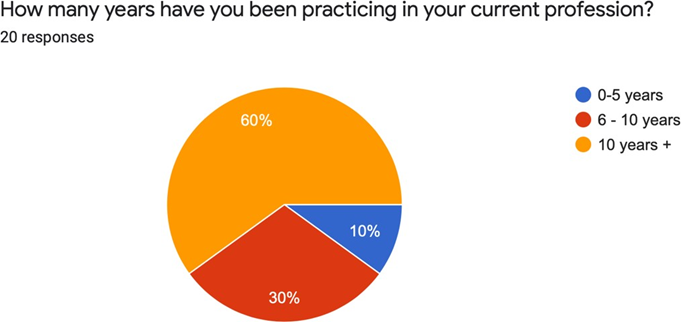
Figure 4. How many years have you been practicing in your current profession?
Pre-test scores based on four questions ranged between 45 and 70 percent while post-test scores ranged from 80 to 100 percent. Before exposure to the educational intervention, the average score for all participants was approximately 58 percent. After exposure, the average score for the entire participant group increased to 89 percent. This direction of change clearly indicated that exposure to the intervention resulted in an improvement in knowledge scores.
Pre-test results revealed that 70% of the participants correctly answered the question regarding the recommended level for IPV screening according to the USPSTF. By comparison, 85% correctly answered the question on the post-test. Only 40% of the respondents correctly identified the appropriate population recommended by the USPSTF for IPV screening compared to the 85% of the respondents who answered it correctly on the post-test. The percentage of individuals who recognized the appropriately screening interval per USPSTF rose from 50% to 85% post educational intervention, as well as the individuals who recognized the recommended screening tool by the USPSTF (from 55% to 78.9%).
After completion of the post-test, participants were asked to evaluate their level of agreement on six items. The ratings capture the range of the respondents’ agreement or disagreement. Ratings were based on a five-point Likert scale of 1 to 5 in which 1=strongly disagree, 2=somewhat disagree, 3 = neither agree nor disagree, 4= somewhat agree and 5= strongly agree. Results revealed a generally high agreement that the training will likely increase the provider’s rate of IPV screening (M=4.47) Agreement scores for each item were not equal and ranged between 4.15-4.68. The strongest agreement received was for the importance of screening for IPV in clinical practice (M=4.68) while the lowest received was for how likely a provider would incorporate IPV screening into their clinical practice (4.15). (See Table 1).
Table 1. Evaluation of Training Session.
|
Question |
Mean |
|
This training session changed some of my attitudes about IPV screening in telemedicine. |
4.47 |
|
This training session will likely help increase my rate of IPV screening with my patients. |
4.42 |
|
This training session will encourage me to address IPV screening at my worksite. |
4.26 |
|
How likely are you to incorporate IPV screening because of this presentation? |
4.26 |
|
What barriers do you perceive to incorporating IPV screening in your current practice? |
“Time” |
|
How important is it for you to screen for IPV in your clinical practice? |
4.68 |
Table 2. Health Belief Model Construct Definitions.
|
Construct |
Definition |
|
Perceived severity |
How serious the condition/its consequences is Belief about getting a condition |
|
Perceived susceptibility |
Belief about costs (psychological + material) if action is taken |
|
Perceived Barriers |
Belief that its worth enacting new behavior to reduce risk |
|
Perceived Benefits |
What motives readiness to change |
|
Cues to Action Self-Efficacy |
Confidence to enact change |
DISCUSSION
The goals of this quality improvement project were to increase clinician knowledge of the USPSTF’s recommendation on intimate partner violence screening in telemedicine, to measure competency and to update policy at the clinical site for screening and referral. The Health Belief Model served as the framework for the development of the project. This framework was used to develop the educational intervention and the results show it was an effective guide in developing the educational intervention and pre-test and post-test results. The findings demonstrate an increase in knowledge/competency among the participants.
Providers were given the opportunity to verbalize common barriers to practice, and while many reasons were given, time was the most common reason (Figure 5). This was not an expected result based on the systematic review of the literature and pre-existing assumptions.
Figure 5. Intimate Partner Violence Screening and Referral: A Quality Improvement Initiative in Telehealth.
The assumption was that providers would find the lack of an integrated screening tool in the platform as the most common barrier based off the systematic review performed.
Participants scored an average of 66% higher on the post-test, which suggested that the educational intervention was successful in increasing provider awareness and knowledge, despite the small sample size of the study group. Outcomes support the conclusion that the educational session plus competency review by screenshare was effective. It is anticipated that the observed increases in IPV screening recommendations and policy implementation will translate to changes in screening recommendation behaviors. Discussions of the results were shared with the project chair and the clinical site medical director and clinical team lead group. I also presented my poster to our entire clinical team via our provider bimonthly meeting.
LIMITATIONS AND RECOMMENDATIONS
This quality improvement project could be used as a model for implementing similar educational interventions with policy updates in other telemedicine and in person clinic settings. Due to the limitation of the small sample size, it is recommended that the project be implemented with a larger number of participants in the future. Additionally, although exposure to the educational session plus screensharing for competency and comfort was effective in increasing immediate knowledge, it is not known the duration of this effect. Policy implementation is key in this area, but the need to track IPV screening rates in the telemedicine site to examine long-term impact as well as provider feedback is necessary.
Initially, when this project was designed, the plan was to put the survey updates on the product roadmap for 2022. During the midst of this project, a merger occurred between my clinical site and another telemedicine company. At this time, it is unknown what the product roadmap will include for 2022 as there are different platforms and priorities moving forward.
CONCLUSION
Intimate partner violence (IPV) is a serious, preventable public health problem and includes sexual and physical violence, stalking and psychological harm inflicted by a current or former partner or spouse [1]. At a time when patients are counting on telemedicine for connection and support from their healthcare providers, clinicians need to be able to screen for IPV and provide resources to all patients. It is known that telehealth interventions may be as effective as face-to-face interventions, and so being able to effectively screen for IPV is of utmost concern [9].
The objective of this project was to increase provider awareness, competency and to effect policy change regarding intimate partner violence screening in telemedicine. Outcomes of this project were based on a pre-test and post-test comparison, participant evaluation regarding the efficiency of the educational intervention and a screenshare to measure provider competency. The planned interventions were successful in increasing provider knowledge, comfort and ability to screen. To create sustainability, policy change was implemented and reinforced with providers at their monthly provider meeting, and a resource page was created in the provider manual for referrals, messaging touchpoints and USPSTF recommendation information. Healthcare providers play a vital role in prevention, screening and decision making with their patients [10-18].
Educating providers on patient and provider barriers to screening for IPV appropriately can lead to further discussion and development of interventions to continue to address these barriers.
REFERENCES
- Centers for Disease Control and Prevention. (2021). Intimate partner violence |violence prevention injury. Centers for Disease Control and Prevention, CDC. Retrieved from: https://www.cdc.gov/violenceprevention/intimatepartnerviolence/index.html.
- Peterman A, Potts A, O'Donnell M, Thompson K, Shah N, Oertelt-Prigione S, van Gelder N. (2020). Pandemics and Violence against Women and Children. Center for Global Development.
- Abrahams IA, Ali O, Davidson L, Evans AC, King JK, Poplawski P, et al. (2010). Philadelphia behavioral health services transformation: Practice guidelines for recovery and resilience oriented treatment. Philadelphia, USA: Department of Behavioral Health and Intellectual Disability Services.
- Tiwari JN, Tiwari RN, Kim KS. (2012). Zero-dimensional, one-dimensional, two-dimensional and three-dimensional nanostructured materials for advanced electrochemical energy devices. Prog Mater Sci. 57(4):724-803.
- Curry S, Krist AH, Owens DK, Barry MJ, Caughey AB, Davidson KW, et al. (2018). Screening for intimate partner violence, elder abuse, and abuse of vulnerable adults: US Preventive Services Task Force final recommendation statement. JAMA. 320(16):1678-1687.
- Hochbaum G, Rosenstock IM. (1952). Health belief model. Washington, DC: United States Public Health Service.
- Rosenstock IM, Strecher VJ, Becker MH. (1988). Social learning theory and the health belief model. Health Education Quarterly. 15(2):175-183.
- Peterson C, Kearns MC, McIntosh WL, Estefan LF, Nicolaidis C, McCollister KE, et al. (2018). Lifetime economic burden of intimate partner violence among U.S. adults. Am J Prev Med. 55(4):433–444.
- Speyer R, Denman D, Wilkes-Gillan S, Chen YW, Bogaardt H, Kim JH, et al. (2018). Effects of telehealth by allied health professionals and nurses in rural and remote areas: A systematic review and meta-analysis. J Rehabil Med. 50(3):225-235.
- Bacchus L, Bullock L, Sharps P, Burnett C, Schminkey DL, Buller AM, et al. (2016). Infusing technology into perinatal home visitation in the United States for women experiencing intimate partner violence: Exploring the interpretive flexibility of an mHealth intervention. J Med Internet Res. 18(11):e302.
- Dutton M, James L, Langhorne A, Kelley M. (2015). Coordinated public health initiatives to address violence against women and adolescents. J Womens Health (Larchmt). 24(1):80-85.
- El Morr C, Manpreet L. (2020). Effectiveness of ICT-based intimate partner violence interventions: A systematic review. BMC Public Health. 20(1):1372.
- Emezue C. (2020). Digital or digitally delivered responses to domestic and intimate partner violence during COVID-19. JMIR Public Health and Surveillance. 6(3):e19831.
- Jack SM, Munro-Kramer ML, Williams JR, Schminkey D, Tomlinson E, Jennings Mayo-Wilson L, et al. (2021). Recognising and responding to intimate partner violence using telehealth: Practical guidance for nurses and midwives. J Clin Nurs. 30(3-4):588-602.
- Krishnamurti T, Davis AL, Quinn B, Castillo AF, Martin KL, Simhan HN. (2021). Mobile Remote Monitoring of Intimate Partner Violence Among Pregnant Patients During the COVID-19 Shelter-In-Place Order: Quality Improvement Pilot Study. J Med Internet Res. 23(2):e22790.
- Linde DS, Bakiewicz A, Normann AK, Hansen NB, Lundh A, Rasch V. (2020). Intimate Partner Violence and Electronic Health Interventions: Systematic Review and Meta-Analysis of Randomized Trials. J Med Internet Res. 22(12):e22361.
- Simon M. (2021). Responding to intimate partner violence during telehealth clinical encounters. JAMA. 325(22):2307-2308.
- Weller SJ, Tippetts D, Weston D, Aldridge RW, Ashby J. (2021) Increase in reported domestic abuse in Integrated Sexual Health (ISH) services in London and surrey during COVID-19 ‘Lockdown’: Successful application of national guidance on routine enquiry during rapid transition to remote telephone consultation. Sex Transm Infect. 97(3):245-246.