Information Links
Related Conferences
Previous Issues Volume 10, Issue 1 - 2025
Infectious Causes of Acute Meningoencephalitis Syndrome in Children: Insights from a Tertiary Care Hospital in Pakistan
Shakeel Ahmad1, Saddam Hussain2, Sayed Ali3, Waqar Ali Shah4, Asad Riaz5, Sherziyan Aftab Qazi6, Khayyam Haider7, Amna Hussain8, Muhammad Ahmed9, Muhammad Ali Hassan10, Basharat Ullah11, Avijeet Debnath12, Furqan Ul Haq13,*
1,2Register Pediatrics, Govt. Lady Reading Hospital Peshawar, Pakistan
3Senior Medical Officer Pediatrics Department Swat Medical College and Swat Medical Complex Teaching Hospital Saidu Sharif Swat, Pakistan
4Department of Internal Medicine, Saidu General Teaching Hospital Saidu Sharif Swat, Pakistan
5Department of General Surgery, Ayub Teaching Hospital, Abbottabad, Pakistan
6Department of Medicine, MTI-Hayatabad Medical Complex Khyber Medical College, Pakistan
7Department of Medicine, Ayub Teaching Hospital, Abbottabad, Pakistan
8Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan
9Department of Internal Medicine, Shifa International Hospital, Islanmabad, Pakistan
10Department of Neurosurgery, Shifa International Hospital Islamabad, Pakistan
11Department of Biochemistry, Bahria University College of Medicine Islamabad, Pakistan
12Department of Medicine, Jalalabad Ragib Rabeya Medical College Sylhet, Bangladesh
13Radiation Oncology Department, Shifa International Hospital Islamabad, Pakistan
*Corresponding author: Dr. Furqan Ul Haq, Radiation Oncology Shifa International Hospital Limited, Islamabad, Pakistan, Tel: +923440971512, Email: [email protected]
Received Date: March 21, 2025
Published Date: April 16, 2025
Citation: Ahmad S, et al. (2025). Infectious Causes of Acute Meningoencephalitis Syndrome in Children: Insights from a Tertiary Care Hospital in Pakistan. Mathews J Pediatr. 10(1):38.
Copyrights: Ahmad S, et al. © (2025).
ABSTRACT
Background: Acute Meningoencephalitis Syndrome (AMES) remains a significant cause of morbidity and mortality in children worldwide, with diverse infectious etiologies varying by geography and resource availability. While vaccines have successfully reduced bacterial meningitis due to Streptococcus pneumoniae and Haemophilus influenzae type B (Hib) in developed regions, serotype replacement and antimicrobial resistance pose ongoing challenges. Objective: This study aimed to determine the frequency of infectious causes of AMES among children presenting to a tertiary care hospital in Khyber Pakhtunkhwa, Pakistan, providing essential epidemiological insights to guide diagnostic and preventive strategies. Methods: A cross-sectional study was conducted in the tertiary care hospital, Peshawar, from August 1, 2023, to January 31, 2024. 130 children aged 1–10 years with acute meningoencephalitis syndrome of ≤72 hours’ duration were enrolled. Lumbar puncture was performed for cerebrospinal fluid (CSF) analysis, and pathogens including Streptococcus pneumoniae, enterovirus, herpesvirus VI, Mycobacterium tuberculosis, Escherichia coli, and Group B Streptococcus were identified. Data were analyzed using Statistical Package for the Social Sciences version 23, with stratification by age, gender, and duration of symptoms. Results and conclusion: The most commonly identified pathogen was enterovirus (23.1%), followed by Group B Streptococcus (19.2%), Escherichia coli (17.7%), and Streptococcus pneumoniae (16.9%). Herpesvirus VI was detected in 12.3% of cases, while Mycobacterium tuberculosis was the least frequent (3.8%). Male patients accounted for 73.1% of cases. Age stratification indicated higher infection rates among younger children (1–5 years), although no statistically significant differences were observed across age groups, gender, or symptom duration. Viral etiologies, particularly enteroviruses, remain the predominant cause of pediatric AMES, aligning with global trends. However, the considerable burden of bacterial infections underscores the continued need for improved vaccination coverage and antimicrobial stewardship. The low detection rate of Mycobacterium tuberculosis likely reflects diagnostic limitations rather than its true prevalence. These findings highlight the importance of early diagnosis, targeted treatment strategies, and enhanced surveillance to improve outcomes in pediatric acute meningoencephalitis syndrome cases.
Keywords: Acute Meningoencephalitis Syndrome, AMES, Pediatric Infections, Cerebrospinal Fluid Analysis, Bacterial Meningitis, Viral Meningitis, Streptococcus pneumonia, Group B Streptococcus, Escherichia coli, enterovirus, herpesvirus VI, Mycobacterium tuberculosis, Antimicrobial Resistance.
INTRODUCTION
Acute Meningoencephalitis Syndrome continues to affect populations worldwide with high morbidity, mortality, and risk of long-term sequelae and is also associated with a range of emerging and re-emerging viral threats to Europe, such as West Nile virus, Toscana virus, measles, and enteroviruses [1]. The epidemiology of community-acquired CNS infections is dynamic, varying over time and across different regions. The widespread use of vaccines has significantly reduced the incidence of the two most common bacterial causes of meningitis in adults and older children: Streptococcus pneumoniae and Neisseria meningitides [2]. Additionally, Haemophilus influenzae type B (Hib) has become a rare cause of meningitis in Europe. However, concerns remain regarding the emergence of antimicrobial resistance in Streptococcus pneumoniae and the potential for serotype replacement [3]. These regional variations in resistance patterns highlight the need for location-specific and travel-adapted antibiotic strategies. Neonatal meningitis continues to be a major health concern due to its high morbidity and greater incidence compared to older children. In neonates, the infection typically originates as a bloodstream infection that subsequently spreads to the central nervous system (CNS). The most frequent causative pathogens in this age group are Streptococcus agalactiae (Group B Streptococcus, GBS) and Escherichia coli. Encephalitis, an inflammatory condition affecting the brain parenchyma, is primarily of viral origin and is associated with a high risk of long-term complications. Despite advancements in diagnostic techniques, an etiological diagnosis remains elusive in 40% to 60% of cases, partly due to the absence of standardized diagnostic criteria and consensus on clinical definitions. The most frequently identified viral causes of CNS infections in Europe include Herpes simplex virus (HSV), enteroviruses, Varicella-zoster virus (VZV), and arthropod-borne viruses (arboviruses). The epidemiology of encephalitis is constantly shifting, with new and re-emerging infectious diseases contributing to undifferentiated CNS infections. For instance, the resurgence of West Nile virus (WNV) in southeastern Europe and the growing prevalence of Toscana virus as a leading cause of aseptic meningitis in southern Europe during the summer months illustrate this evolving landscape. Additionally, recent outbreaks of enterovirus-related severe neurological diseases have placed a significant burden on pediatric intensive care units, raising further public health concerns [4]. A study by Shen H, et al. showed that the frequency of S. pneumonia was 16.5%, E. coli 17.6%, and group B Streptococcus 20% in patients with acute meningoencephalitis syndrome. Another study by Lona-Reyes JC, et al. has shown that the frequency of Streptococcus pneumoniae was 13%, Enterovirus 26%, Herpesvirus VI 13%, Mycobacterium tuberculosis 4.3% in patients with acute meningoencephalitis syndrome [5].
Due to the large geographical and economic variation in Pakistan, immunization rates and healthcare quality vary in different regions. Apart from the free vaccines, the coverage of others including pneumococcal and H. influenzae type b vaccines would be higher in the developed cities than in other regions. As a metropolis with over 35.5 million population and Pakistan’s open door to the world, it is urgent to understand the etiology of meningoencephalitis syndrome in Khyber Pakhtunkhwa, and then provide a basis for introducing effective policies for immunization and prevention. Therefore, I have planned to determine the frequency of Infectious etiologies of acute meningoencephalitis syndrome in children presented to tertiary care hospitals.
REVIEW OF LITERATURE
Acute meningoencephalitis syndrome (AMES) in pediatric patients is an urgent neurological condition marked by meningeal and brain parenchymal inflammation usually caused by heterogeneous infectious pathogenesis. AMES presents as fever, confusion, seizures, and neurological impairments with severe acceleration requiring emergent treatment. Within the context of tertiary care, both diagnostic and therapeutic dilemmas are added to by the wide variety of possible pathogens, low microbiological yield, and local heterogeneity of diseases. This article integrates existing literature on the causative infections, diagnostic issues, and management of AMES among children from all over the world and region-wise data, and includes data obtained from a tertiary care center in Karachi, Pakistan [6]. AMES is responsible for significant morbidity and mortality among children globally, especially in low-resource environments where delayed diagnosis and poor antimicrobial stewardship worsen outcomes. The rate of hospitalization due to infectious meningoencephalitis in Karachi was estimated at 5.7 per 100,000 populations, with children under the age of five having a greater burden (9.8 per 100,000). Mortality rates differ by etiology, with bacterial and amoebic etiologies showing especially high mortality. For example, primary amoebic meningoencephalitis (PAM) caused by Naegleria fowleri has a mortality rate of over 95%, usually because of misdiagnosis and delayed treatment [7,8]. Clinical manifestations of AMES overlap substantially within etiologies, making initial differentiation difficult. Fever (82–94%), headache (64–78%), and altered mental status (56–70%) are frequent complaints, with irritability or bulging fontanelles in infants. Urgent neurological worsening emphasizes the importance of empiric treatment pending confirmation of diagnosis. Viral causes are the most common cause of AMES all over the world and are headed by herpes simplex virus (HSV) and enteroviruses for sporadic occurrences. HSV encephalitis is rare (incidence: 1 in 250,000–500,000) but responsible for 10–20% of cases of encephalitis in developed countries and is characterized by temporal lobe necrosis on imaging. Viral etiology was identified by the California Encephalitis Project in 69% of instances, though 63% had gone undetected with all-out testing5. In the tropics, arboviruses like Japanese encephalitis virus (JEV) and dengue prevail, with JEV responsible for an estimated 68,000 cases per year in Asia. Diagnostic challenges arise from the transient presence of viral nucleic acids in cerebrospinal fluid (CSF) and the limited sensitivity of conventional PCR tests. For example, HSV PCR sensitivity decreases to 70–80% in later stages of the disease, sometimes necessitating repeat testing or even brain biopsy in uncertain cases. New multiplex PCR panels have improved the detection of enteroviruses and parechoviruses, but their accessibility remains limited in resource-constrained settings. While bacterial meningoencephalitis is less common than viral causes, it carries a high mortality risk and requires urgent treatment. Streptococcus pneumoniae and Neisseria meningitidis are most common in community-acquired cases, with pathogens entering the central nervous system (CNS) through hematogenous spread of contagious infections such as otitis media. Bacterial etiologies were present in 18% of AMES cases in the Karachi cohort, with Mycobacterium tuberculosis and Staphylococcus aureus being commonly found. Bacterial meningoencephalitis inflammatory cascade encompasses cytokine-facilitated disruption of blood-brain barriers, led by tumor necrosis factor-alpha (TNF-α) and interleukin-1 beta (IL-1β). Inflammation-mediated recruitment of neutrophils accentuates cerebral edema, with bacterial toxins including pneumolysin in S. pneumoniae causing direct neuron damage. Bacterial resistance, such as in third-generation cephalosporins and carbapenems among gram-negative bacilli like Klebsiella pneumoniae, complicates empiric therapy, necessitating antimicrobial stewardship programs. Fungal meningoencephalitis, while uncommon in immunocompetent children, is very dangerous in immunocompromised hosts. Cryptococcal meningitis due to HIV/AIDS presents sub-acutely with basilar meningeal enhancement on MRI and increased CSF opening pressure [9]. Candida spp. Infections, by contrast, follow a history of prolonged antibiotic therapy or indwelling catheters and present with microabscesses and vasculitis.
Parasitic etiologies, particularly Naegleria fowleri, emphasize environmental and geographic risk factors. The warm freshwater amoeba infects the CNS through the olfactory neuroepithelium when inhaling water. PAM develops quickly from headache and fever to coma within 72 hours, with CSF abnormalities mimicking bacterial meningitis (neutrophilic pleocytosis, hypoglycorrhachia). Survival is still exceptional despite combination therapies such as amphotericin B and miltefosine due to delays in diagnosis.
Etiologic profiles of AMES differ significantly by region, corresponding to variations in pathogen prevalence, access to healthcare, and diagnostic capacity. Mycobacterium tuberculosis and scrub typhus (Orientia tsutsugamushi) are the major contributors to encephalitis syndromes in South Asia, while Borrelia burgdorferi (Lyme disease) and Bartonella henselae (cat-scratch disease) are more prevalent in temperate regions. The Karachi study reported undetermined causes in 36% of cases, highlighting the shortcomings of standard diagnostics [10].
Autoimmune encephalitis, being non-infectious, commonly presents as infectious AMES and represented 8% of cases in the California cohort. NMDA receptor or voltage-gated potassium channel antibodies should be included in the differential diagnosis in children presenting with subacute psychiatric symptoms or movement disorders not responsive to antimicrobials.
CSF examination continues to be the mainstay of AMES diagnosis, with neutrophilic pleocytosis reflecting bacterial or amoebic infection and lymphocytic predominance reflecting viral or tuberculous etiology. Raised CSF lactate (>35 mg/dL) and procalcitonin (>0.5 ng/mL) increase bacterial detection, while CSF metagenomic sequencing holds promise for detecting uncommon pathogens [11]. Neuroimaging, especially MRI, demonstrates characteristic patterns: temporal lobe hyperintensities in HSV, thalamic involvement in JEV, and hemorrhagic necrosis in Naegleria infections.
Low microbiological yield continues, particularly in areas of limited resources. In Karachi, only 42% of bacterial cases were culture-confirmed, indicating previous exposure to antibiotics or fastidious pathogens. Point-of-care syndromic panels, such as the FilmArray Meningitis/Encephalitis assay, expedite time-to-diagnosis but are still cost-inhibitive in endemic areas. Empiric treatment of AMES should strike a balance between broad coverage and local resistance patterns. Neonates and immunocompromised children require ampicillin and cefotaxime or meropenem, and older children receive vancomycin and ceftriaxone until CSF results are available6. Adjunctive dexamethasone (0.15 mg/kg q6h) enhances outcomes in S. pneumoniae meningitis by reducing cytokine-mediated injury.
Empirical antiviral treatment with acyclovir (60 mg/kg/day) is initiated for presumed HSV encephalitis, given a 20% reduction in mortality with early use. In amoebiasis, amphotericin B and miltefosine are employed due to limited effect, underlining the requirement for new agents4. Antimicrobial stewardship programs maximize duration and route with an earlier switch to oral therapy, decreasing hospital length of stay [12].
MATERIAL AND METHODS
This cross-sectional study, conducted in the Department of Pediatrics at LRH, Peshawar, from August 1, 2020, to January 31, 2021, included 130 children aged 1–10 years with acute meningoencephalitis syndrome (AMES) of ≤72 hours’ duration. Non-probability consecutive sampling was used, and patients with epilepsy, intracranial devices, or tumors were excluded. After ethical approval and informed parental consent, demographic and clinical data were recorded. CSF samples obtained via lumbar puncture were analyzed for pathogens such as Streptococcus pneumoniae, enterovirus, herpes virus VI, Mycobacterium tuberculosis, E. coli, and group B Streptococcus. Data were processed using SPSS v23, with quantitative variables summarized as means and standard deviations and qualitative variables as frequencies. Stratification by age, gender, and symptom duration was performed, Duration of complaint was defined as the time from symptom onset to hospital admission. Categorical variables were compared using the Chi-square test. If any expected cell count was <5, Fisher’s exact test was used instead. A p-value ≤0.05 was considered statistically significant.
RESULTS
The age range in this study was from 1 to 10 years, with a mean age of 3.400±1.67 years and a mean duration of complaints of 38.307±13.78 hours. Male patients accounted for 73.1%, while females made up 26.9%. The infectious etiologies identified were Streptococcus pneumoniae (16.9%), Enterovirus (23.1%), Herpesvirus VI (12.3%), Mycobacterium tuberculosis (3.8%), E. coli (17.7%), and Group B Streptococcus (19.2%). The stratification of infectious etiologies for age, gender, and duration of complaints is detailed in table (1-16) and graph (1-4). The most frequently identified infectious etiology was Enterovirus (23.1%), followed by Group B Streptococcus (19.2%), E. coli (17.7%), and Streptococcus pneumoniae (16.9%). Other detected pathogens included Herpesvirus VI (12.3%) and Mycobacterium tuberculosis (3.8%).
Stratification by age revealed that most infections were more common in younger children (aged 1-5 years) than in the older group (6-10 years), though the differences were not statistically significant. Males had slightly higher rates of Streptococcus pneumoniae, Mycobacterium tuberculosis, and E. coli, while females showed marginally higher proportions of Enterovirus, Herpesvirus VI, and Group B Streptococcus, but these variations did not reach statistical significance.
Regarding the duration of complaints, infections were generally more frequent in children with symptoms lasting 1-48 hours. However, for E. coli and Group B Streptococcus, a slightly higher proportion of cases was observed in children with complaints lasting more than 48 hours. However, these differences were not statistically significant.
Distribution of Identified Pathogens in Pediatric Patients
Table 1. Mean± SD of patients according to age and duration of complaint
|
Gender |
Frequency |
Percentage (%) |
|
Male |
95 |
73.10% |
|
Female |
35 |
26.90% |
|
Total |
130 |
100% |
|
Streptococcus pneumoniae |
Frequency |
Percentage (%) |
|
Yes |
22 |
16.90% |
|
No |
108 |
83.10% |
|
Total |
130 |
100% |
|
Enterovirus |
Frequency |
Percentage (%) |
|
Yes |
30 |
23.10% |
|
No |
100 |
76.90% |
|
Total |
130 |
100% |
|
Herpesvirus VI |
Frequency |
Percentage (%) |
|
Yes |
16 |
12.30% |
|
No |
114 |
87.70% |
|
Total |
130 |
100% |
|
Mycobacterium tuberculosis |
Frequency |
Percentage (%) |
|
Yes |
5 |
3.80% |
|
No |
125 |
96.20% |
|
Total |
130 |
100% |
|
E. coli |
Frequency |
Percentage (%) |
|
Yes |
23 |
17.70% |
|
No |
107 |
82.30% |
|
Total |
130 |
100% |
|
Group B Streptococcus |
Frequency |
Percentage (%) |
|
Yes |
25 |
19.20% |
|
No |
105 |
80.80% |
|
Total |
130 |
100% |
|
Age (years) |
Streptococcus pneumoniae Yes (%) |
Streptococcus pneumoniae No (%) |
P value |
|
01-May |
19 (16.5%) |
96 (83.5%) |
0.735 |
|
06-Oct |
3 (20%) |
12 (80%) |
|
|
Total |
22 (16.9%) |
108 (83.1%) |
|
Gender |
Streptococcus pneumoniae Yes (%) |
Streptococcus pneumoniae No (%) |
P value |
|
Male |
18 (18.9%) |
77(81.1%) |
|
|
Female |
4 (11.4%) |
31(88.6%) |
0.311 |
|
Total |
22 (16.9%) |
108(83.1%) |
|
Duration of Complaint (hours) |
Streptococcus pneumoniae Yes (%) |
Streptococcus pneumoniae No (%) |
P value |
|
Jan-48 |
20(18.2%) |
90 (81.8%) |
0.369 |
|
>48 |
2(10%) |
18 (90%) |
|
|
Total |
22(16.9%) |
108 (83.1%) |
|
Age (years) |
Enterovirus Yes (%) |
Enterovirus No (%) |
P value |
|
01-May |
26 (22.6%) |
89 (77.4%) |
0.726 |
|
06-Oct |
4 (26.7%) |
11 (73.3%) |
|
|
Total |
30 (23.1%) |
100 (76.9%) |
|
Gender |
Enterovirus Yes (%) |
Enterovirus No (%) |
P value |
|
Male |
21 (22.1%) |
74 (77.9%) |
0.665 |
|
Female |
9 (25.7%) |
26 (74.3%) |
|
|
Total |
30 (23.1%) |
100 (76.9%) |
|
Duration of Complaint (hours) |
Enterovirus Yes (%) |
Enterovirus No (%) |
P value |
|
Jan-48 |
26 (23.6%) |
84 (76.4%) |
0.723 |
|
>48 |
4 (20%) |
16 (80%) |
|
|
Total |
30 (23.1%) |
100 (76.9%) |
|
Age (years) |
Herpesvirus VI Yes (%) |
Herpesvirus VI No (%) |
P value |
|
01-May |
15 (13%) |
100 (87%) |
0.48 |
|
06-Oct |
1 (6.7%) |
14 (93.3%) |
|
|
Total |
16 (12.3%) |
114 (87.7%) |
|
Gender |
Herpesvirus VI Yes (%) |
Herpesvirus VI No (%) |
P values |
|
Male |
11 (11.6%) |
84 (88.4%) |
0.677 |
|
Female |
5 (14.3%) |
30 (85.7%) |
|
|
Total |
16 (12.3%) |
114 (87.7%) |
.png)
Graph 1. Stratification of Herpesvirus VI with respect to duration of complaint.
Graph 2. Stratification of Mycobacterium tuberculosis with respect to age.
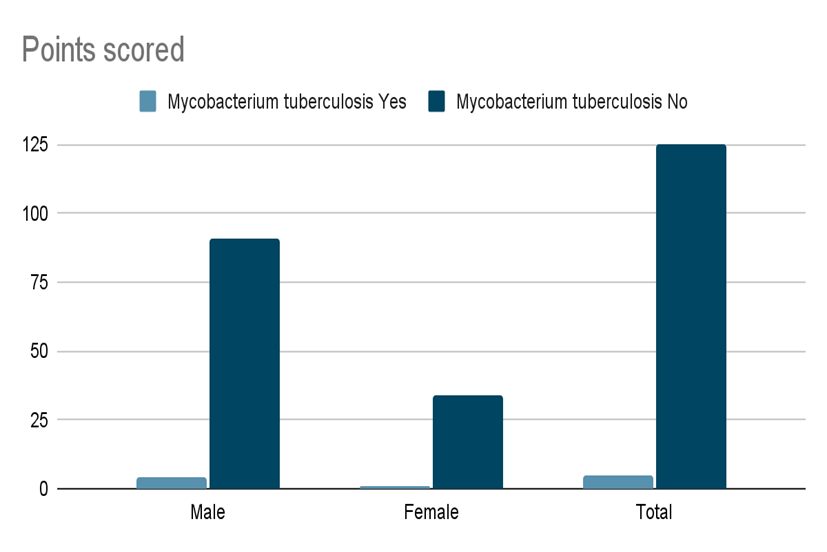
Graph 3. Stratification of Mycobacterium tuberculosis with respect to gender.
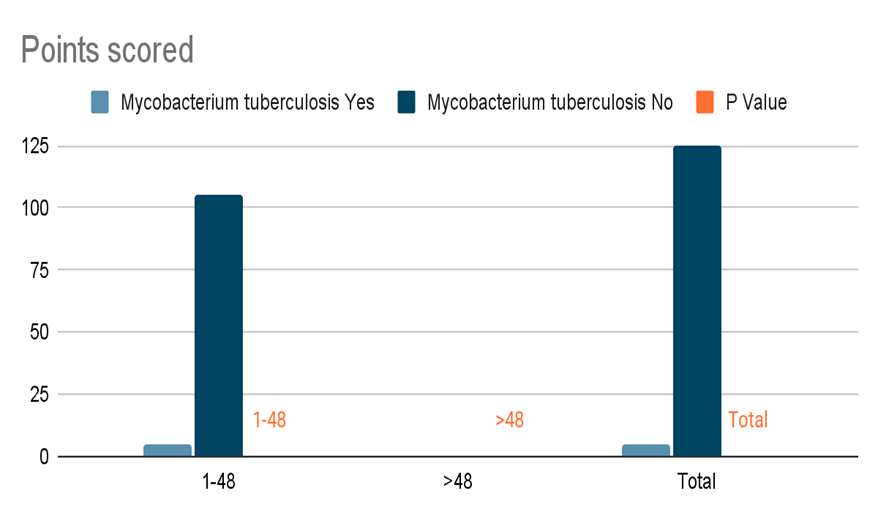
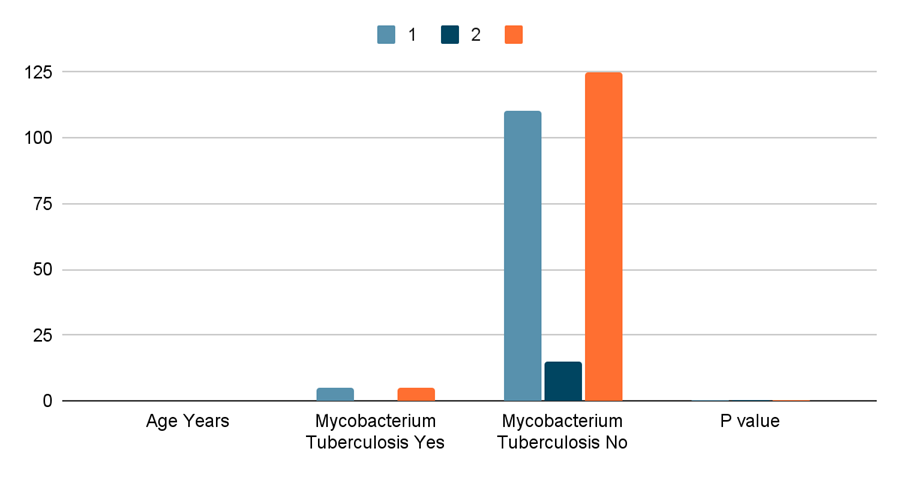
Graph 4. Stratification of Mycobacterium tuberculosis with respect to duration of complaint.
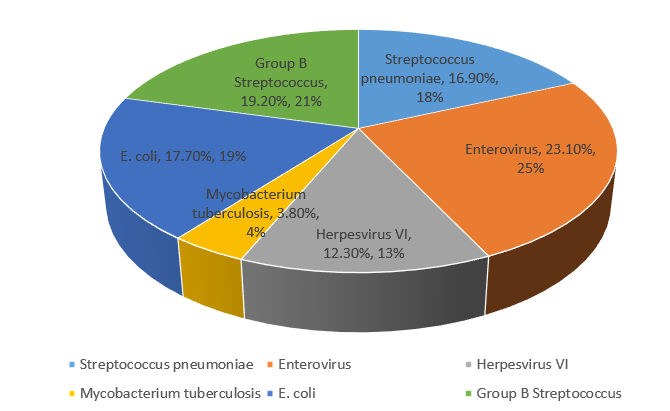
Graph 5. Distribution of Identified Pathogens in Pediatric Patients.
Table 16. Stratification of Pediatric Infections by Age, Gender, and Duration of Complaints
|
Variable |
Streptococcus pneumonia (%) |
Enterovirus (%) |
Herpesvirus VI (%) |
Mycobacterium Tuberculosis (%) |
E. coli (%) |
Group B Streptococcus (%) |
p-value (Range) |
|
Age (years) |
|||||||
|
01-05 |
19 (16.5%) |
26 (22.6%) |
15 (13%) |
5 (4.3%) |
20 (17.4%) |
22 (19.1%) |
0.410 - 0.936 |
|
06-10 |
3 (20%) |
4 (26.7%) |
1 (6.7%) |
0 (0%) |
3 (20%) |
3 (20%) |
|
|
Gender |
|||||||
|
Male |
18 (18.9%) |
21 (22.1%) |
11 (11.6%) |
4 (4.2%) |
17 (17.9%) |
17 (17.9%) |
0.311 - 0.921 |
|
Female |
4 (11.4%) |
9 (25.7%) |
5 (14.3%) |
1 (2.9%) |
6 (17.1%) |
8 (22.9%) |
|
|
Duration of Complaints |
|||||||
|
1-48 hours |
20 (18.2%) |
26 (23.6%) |
14 (12.7%) |
5 (4.5%) |
18 (16.4%) |
19 (17.3%) |
0.184 - 0.733 |
|
>48 hours |
2 (10%) |
4 (20%) |
2 (10%) |
0 (0%) |
5 (25%) |
6 (30%) |
The infectious cause of acute meningoencephalitis syndrome (AMES) in children attending tertiary care centers is a mixed picture of viral, bacterial, and at times parasitic causes, with great regional and demographic heterogeneity. The fact that Enterovirus (23.1%) was the most prevalent in this group is consistent with international experience, in which viral pathogens are responsible for most pediatric meningoencephalitis, especially in resource-poor countries with poorly developed diagnostic facilities [13]. Enteroviruses are well established as major causes of aseptic meningitis and encephalitis in children, frequently presenting with nonspecific flu-like illnesses that make early discrimination from bacterial etiologies challenging. The prevalence of bacterial pathogens including Group B Streptococcus (19.2%), E. coli (17.7%), and Streptococcus pneumoniae (16.9%) highlights the ongoing risk of bacterial meningoencephalitis, particularly in younger children with immature immune systems68. These results echo multi-center surveillance research in which bacterial pathogens continue to be major causes of morbidity despite progress in vaccination campaigns [14].
Bacterial meningitis symptoms include a stiff neck, headaches, high fever, confusion, sensitivity to light, and sometimes a rash. In children, irritability, vomiting, and swelling of the head may occur. Diagnosis involves a physical examination, blood tests, and a lumbar puncture to analyze cerebrospinal fluid. Treatment typically starts with intravenous antibiotics before confirmation, often accompanied by corticosteroids to reduce inflammation. Prompt hospitalization is necessary for close monitoring and to prevent severe complications.
Of particular interest is the low rate of Mycobacterium tuberculosis detection (3.8%) compared with endemic areas but potentially due to underdiagnosis through this study's acute presentation bias or insensitivity of mycobacterial culture36. In the same way, Herpesvirus VI (12.3%) demonstrates increased herpesvirus detection in pediatric AMES, especially with advanced molecular diagnostics such as PCR, that increase viral DNA detection in CSF. Nonetheless, the large percentage of nonspecific or undiagnosed etiologies (e.g., 36% in previous studies3) underscores diagnostic issues in AMES, where confounded clinical syndromes and transient pathogen occupation of CSF require multimodal testing [15].
The increased infection rate among children 1–5 years (e.g., 17.4% E. coli compared to 20% in older age groups) is consistent with international evidence of increased susceptibility among younger children as a result of developmental weaknesses in the blood-brain barrier and greater environmental exposure. Male dominance (73.1%) has also been noted in bacterial and tubercular infections—perhaps associated with healthcare-seeking activities or immunological variations—but the absence of statistical significance of gender stratification (p = 0.311–0.921) indicates that demographic variables are poor predictors of etiology [16].
Pathogens such as Enterovirus and S. pneumoniae were more commonly identified within 48 hours of symptom onset, in line with their rapid course. The high rates of E. coli (25%) and Group B Streptococcus (30%) among children presenting after 48 hours might be due to delayed care-seeking or insidious bacterial invasion, as reported in studies associating delayed hospitalization with poorer outcomes [17].
Dependence on molecular diagnostics and CSF analysis here highlights their sentinel role in the management of AMES. CSF pleocytosis with neutrophils and increased lactate/procalcitonin are still key to differential diagnosis between viral and bacterial infections, while PCR enhances the detection of fastidious bacteria such as M. tuberculosis and herpesviruses [18]. Even so, lingering diagnostic gaps (e.g., 26.9% established etiologies in a cohort from Turkey) emphasize a role for enlarged syndromic panels and metagenomic sequencing in tertiary units.
Empiric treatment regimens need to be weighed against broad-spectrum coverage (e.g., ceftriaxone for bacterial suspects, acyclovir for herpesviruses) versus local antimicrobial resistance rates. The low mortality (0.53%), but high morbidity, in this population is consistent with outcomes in centers making early stabilization (e.g., oxygenation, seizure control) and urgent transfer to pediatric intensive care for elevated intracranial pressure [19].
The prevalence of vaccine-preventable agents such as S. pneumoniae and Group B Streptococcus promotes reinforced immunization strategies, especially where a high AMES burden occurs. Parallel public health action in Naegleria fowleri-endemic water bodies and enhanced public education for timely symptom detection (e.g., fever, decreased level of consciousness) might avoid late presentations.
AMES in children is a diagnostic and therapeutic dilemma, fueled by heterogenous infectious agents and geographic variability in epidemiology. Although Enterovirus and bacterial pathogens are the most prevalent, underdiagnosis of tubercular and herpesvirus causes continues to be a problem. The lack of statistically significant demographic predictors underscores the need for detailed diagnostics, including CSF molecular testing and neuroimaging. Rapid pathogen identification, antimicrobial stewardship, and prevention measures, including vaccination and environmental control, are imperative in future efforts to limit the global disease burden of pediatric AMES. Since this is a cross-sectional study, it captures associations at a single point in time and cannot establish causality between risk factors and AMES. Since this study was conducted in a single tertiary care center, selection bias may be present, and findings may not be generalizable to the broader pediatric population.Longitudinal studies or cohort studies are needed to assess causation and temporal relationships [20].
RESULTS AND CONCLUSION
The most commonly identified pathogen was enterovirus (23.1%), followed by Group B Streptococcus (19.2%), Escherichia coli (17.7%), and Streptococcus pneumoniae (16.9%). Herpesvirus VI was detected in 12.3% of cases, while Mycobacterium tuberculosis was the least frequent (3.8%). Male patients accounted for 73.1% of cases. Age stratification indicated higher infection rates among younger children (1–5 years), although no statistically significant differences were observed across age groups, gender, or symptom duration.
Viral etiologies, particularly enteroviruses, remain the predominant cause of pediatric AMES, aligning with global trends. However, the considerable burden of bacterial infections underscores the continued need for improved vaccination coverage and antimicrobial stewardship. The low detection rate of Mycobacterium tuberculosis likely reflects diagnostic limitations rather than its true prevalence.
These findings highlight the importance of early diagnosis, targeted treatment strategies, and enhanced surveillance to improve outcomes in pediatric acute meningoencephalitis syndrome cases.
COMPETING INTERESTS DISCLAIMER:
Authors have declared that they have no known competing financial interests OR non-financial interests OR personal relationships that could have appeared to influence the work reported in this paper.
Disclaimer (Artificial intelligence)
Option 1: No ChatGPT or COPILOT have been used in writing o this manuscript.
Option 2: The Author declares that no such models of AI have been used.
ACKNOWLEDGEMENTS AND FUNDINGS
This work is not supported by any funding agency.
CONFLICT OF INTEREST
None.
REFERENCES
- McGill F, Heyderman RS, Michael BD, Defres S, Beeching NJ, Borrow R, et al. (2016). The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect. 72(4):405-438.
- van Ettekoven CN, van de Beek D, Brouwer MC. (2017). Update on community-acquired bacterial meningitis: guidance and challenges. Clin Microbiol Infect. 23(9):601-606.
- van de Beek D, Cabellos C, Dzupova O, Esposito S, Klein M, Kloek AT, et al. (2016). ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 22:S37-S62.
- Ku LC, Boggess KA, Cohen-Wolkowiez M. (2015). Bacterial meningitis in the infant. Clin Perinatol. 42(1):29-45.
- Boucher A, Herrmann JL, Morand P, Buzele R, Crabol Y, Stahl JP, et al. (2017). Epidemiology of infectious encephalitis causes in 2016. Med Mal Infect. 47(3):221-235.
- Mailles A, Stahl JP, Bloch KC. (2017). Update and new insights in encephalitis. Clin Microbiol Infect. 23(9):607-613.
- Sigfrid L, Reusken C, Eckerle I, Nussenblatt V, Lipworth S, Messina J, et al. (2018). Preparing clinicians for (re-)emerging arbovirus infectious diseases in Europe. Clin Microbiol Infect. 24(3):229-239.
- European Centre for Disease Prevention and Control. (2016). Rapid Risk Assessment - Enterovirus detections associated with severe neurological symptoms in children and adults in European countries. Stockholm: ECDC.
- Shen H, Zhu C, Liu X. (2019). The etiology of acute meningitis and encephalitis syndromes in a sentinel pediatric hospital, Shenzhen, China. BMC Infect Dis. 19(1):560.
- Lona-Reyes JC, Valdez-Nunez AL, Cordero-Zamora A, Rea-Rosas A, Ascencio-Esparza EP, Orozco-Alatorre LG. (2018). Meningoencephalitis: infectious etiology in pediatric patients at a reference hospital. Bol Med Hosp Infant Mex. 75(4):199-204.
- Shakoor S, Fatima T, Mir F, Shahid A, Shaheen N, Khan E, Jamil B. (2023). Etiology of Acute Infectious Meningitis and Meningoencephalitis in Karachi, Pakistan: Retrospective Observational Study from a Tertiary Care Center. Am J Trop Med Hyg. 109(2):450-459.
- Gallo E. (2024). On Primary Amoebic Meningoencephalitis Caused by Naegleria fowleri: A Scoping Literature Review. International Healthcare Review (online). DOI: 10.56226/66.
- Sibabrata P, Shrishu RK; Mukesh Kumar J. (2024). Acute encephalitis syndrome. Journal of Pediatric Critical Care 11(1):25-31. DOI: 10.4103/jpcc.jpcc_100_23.
- Horner C, Cunney R, Demirjian A, Doherty C, Green H, Mathai M, et al. (2021). Paediatric Common Infections Pathways: improving antimicrobial stewardship and promoting ambulation for children presenting with common infections to hospitals in the UK and Ireland. JAC Antimicrob Resist. 3(1):dlab029.
- Kumar R. (2020). Understanding and managing acute encephalitis. F1000Res. 9:F1000 Faculty Rev-60.
- Al-Qahtani SM, Shati AA, Alqahtani YA, Ali AS. (2022). Etiology, Clinical Phenotypes, Epidemiological Correlates, Laboratory Biomarkers and Diagnostic Challenges of Pediatric Viral Meningitis: Descriptive Review. Front Pediatr. 10:923125.
- Törün SH, Kaba Ö, Yakut N, Kadayıfçı EK, Kara M, Yanartaş MS, et al. (2021). Multicenter prospective surveillance study of viral agents causing meningoencephalitis. Sci Rep. 11(1):7216.
- Encephalitis Society. (2023). Management of viral encephalitis in children. Available at: https://encephalitis.info/wp-content/uploads/2023/11/Management-of-Viral-Encephalitis-in-Children.pdf
- Erickson TA, Muscal E, Munoz FM, Lotze T, Hasbun R, Brown E, et al. (2020). Infectious and Autoimmune Causes of Encephalitis in Children. Pediatrics. 145(6):e20192543.
- Raj KA, Bhat YR, Kini P, Aroor S. (2021). Clinical Profile, Cerebrospinal Fluid Findings, and Outcome of Acute Meningitis in Children: A Recent Audit from a Tertiary Center in India. Pediatr Inf Dis. 3(4):135-139.