Information Links
Related Conferences
Previous Issues Volume 3, Issue 1 - 2021
Improving Depression Screening Through Utilization of a Depression Screening Protocol in Primary Care
Fredricka Marsh, DNP, APRN, FNP, MSN
University of Alabama, Capstone College of Nursing, USA
Corresponding Author: Fredricka Marsh, Capstone College of Nursing, University of Alabama, USA, E-mail: [email protected]
Received Date: May 22, 2021
Published Date: September 24, 2021
Copyright: Marsh F. © (2021). This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Marsh F. (2021). Improving Depression Screening Through Utilization of a Depression Screening Protocol in Primary Care. Mathews J Nurs. 3(1):04.
ABSTRACT
The purpose of this Quality Improvement (QI) project was to implement an evidence-based protocol focused on consistent utilization of an evidence-based depression screening tool using the United States Preventive Service Task Force (USPSTF) and the Patient Health Questionnaire-9 (PHQ-9), among patients 18 to 75 years of age who receive care in a primary care setting. A retrospective chart review was conducted two weeks prior to implementation of the PHQ-9 depression screening tool, 100 randomly selected patient charts were selected by reviewing every third patient chart that met the criteria of 18 to 75 years of age. Frequencies and percentages were calculated and separated by pre- and post-implementation (before and after) implementation of the evidence-based protocol, the PHQ-9, for age, race, and gender. The findings suggest the mean of the PHQ-9 score was significantly higher in the post-implementation categories than in the pre- implementation categories in the proportion of patients 18 to 75 years of age who received the depression screening tool, PHQ-9. Therefore, utilizing a depression screening protocol will be a guide for providers to consistently assess patients for depression and promote adequate diagnosing and early interventions and treatment.
KEYWORDS: Depression; Depression Symptoms; Depression Screening; Depression Screening in Primary Care
INTRODUCTION
In the United States (U.S.), approximately 500 million Americans are living with mental health disorders [1]. Depression is a severe mental health disorder that affects individuals from all cultures, age groups, and socioeconomic backgrounds. Depression is a leading cause of disability worldwide [2]. This chronic debilitating disease has become a major clinical health concern. Primary care providers are essential in recognizing and managing depression and at least 60% of mental health diagnoses occur in the primary healthcare setting [3]. According to Akincigil and Matthews [4], 13 to 16% of adults will experience some form of mental health disorder in their lifetime. A recent study identified that less than 5% of adults in primary care are screened for depression [4]. According to the United States Preventive Service Task Force (USPSTF) [5] and despite guideline recommendations, depression symptoms continue to be underdiagnosed in primary healthcare settings [4]. According to Hedden, Copello, Tice, and Hunter [6], 43.6 million Americans, 18 years and older, suffered with an emotional mental or behavioral disorder within the previous twelve-months. It is critical for primary care settings to provide the most effective screening tools for recognizing depression as quickly as possible. Therefore, use of a depression screening protocol will provide a guide for providers’ to consistently assess for depression and improve in early identification of depression symptoms, which will promote adequate diagnosing, and early interventions and treatment.
This Doctoral Nursing Project, quality improvement (QI) evaluation project, resulted from observation of lack of utilization of a depression screening protocol that would consistently recognize depression in a vulnerable population in a primary health care clinic. This project is aimed to assess, develop, implement, and evaluate implementation of an adult depression screening protocol. Utilizing evidence-based guidelines, the USPSTF and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool will give rise to ultimately facilitate continuous utilization of proper screening for depression among adults 18 to 75 years of age at a primary care clinic located in Fort Lauderdale, Florida. Implementing a new screening protocol, could increase uniformity of screening for depression among patients. Early screening and access to treatment represents opportunities to increase access and continuity of quality care.
PROBLEM DESCRIPTION
It is not known if or to what extent the implementation of an evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool will affect the frequency of screening at a primary care clinic located in Fort Lauderdale, Florida. Fort Lauderdale is a city located in Broward County. It is the home of approximately 180,072 people. According to the Substance Abuse and Mental Health Services Administration [SAMHSA], National Service of Drug Use and Health [7], the prevalence of individuals suffering with mental health disorders in the Fort Lauderdale-Miami metropolitan areas are approximately 4.9 percent. Many residents residing in Fort Lauderdale suffers with mental health conditions such as anxiety and depression [9].
As stated by the World Health Organization [2], patients who suffer from depression may experience higher rates of mortality. Despite the clinical significance and growing health issues that result from depression, approximately 12 million people in the U.S. are currently experiencing depression each year [9].
Research has shown that depression is one of the most common mental health disorders in the United States [10]. Despite the increased prevalence of depression, and the recommendations from the USPSTF, rates of screening for depression in primary care are as low as 1 to 2% [11]. Although depression is a major concern, the goal of this quality improvement project is to improve depression screening through utilization of a depression screening protocol. Consistent use of a depression screening protocol is vital to improving patient health outcomes for those patients who suffer with depression symptoms.
Depression not only affects quality of life but can be a significant cause of disability and mortality [12]. In 2015, Kato E, et al. [12] showed that somatic symptoms associated with depression were often diagnosed and treated as physical illness because somatic symptoms often occur with other medical conditions. In the U.S. it has been estimated that 17.1 million adults 18 years and older have had at least one depressive episode [10]. A significant number of people suffering from depression in the U.S. continue to be underdiagnosed and under treated [12]. The long-term impact of depression, whether indirect or direct, has an enormous effect on morbidity and mortality [13]. Research suggests that depressive symptoms may interfere with all aspects of an individual’s life including their physical health, professional and personal relationships, socioeconomic status, and self-esteem [14]. The global cost for treating mental health disorders has dramatically increased since 2010, and is projected to continue to rise until the year 2030; costing the health care industry approximately $60 trillion [1]. In 2010, according to Greensberg, Fournier, Sisitsky, Pike, & Kessler [15], the economic burden of depression accounted for more than $210 billion. To decrease the high prevalence rates of morbidity and mortality of depression, use of a depression screening protocol can be crucial in early identification and treatment of mental health disorders. In a study by Hoff, Crawford, and Mersereau [16], research showed 28% of providers screened patients for anxiety or depression, 52% of providers asked the patient if they were having depression symptoms, and 29% of providers used an evidence-based depression screening tool. The consistent use of an evidence-based depression screening protocol is essential for providers to identify patients who suffer with symptoms of depression. Therefore, to provide quality care and improve depressive symptoms in patients with mental health disorders to ensure patient safety, treatment guidelines are necessary for the improving early detection of depression using an evidence-based depression screening process [17].
AVAILABLE KNOWLEDGE
In the United States (U.S.), approximately 500 million Americans are living with mental health disorders [1]. Depression is a severe mental health disorder that affects individuals from all cultures, age groups, and socioeconomic backgrounds. Depression is one of the leading causes of disability worldwide [2]. This chronic debilitating disease has become a major clinical health concern. Primary care providers are essential in recognizing and managing depression and at least 60% of mental health diagnoses occur in the primary healthcare setting [3]. Despite the increased prevalence of depression, and the recommendations from the USPSTF, rates of screening for depression in primary care are as low as 1 to 2% [10]. Approximately 15 million adults within the U.S. suffer from at least one major episode of depression that lasted longer than 2 weeks [10]. A recent study identified that less than 5% of adults in primary care are screened for depression [4]. According to the United States Preventive Service Task Force (USPSTF) [5], depression symptoms continue to be underdiagnosed in primary healthcare settings. Therefore, use of a depression screening protocol will provide a guide for providers to frequently assess for depression and improve in early identification of depression symptoms, which will promote adequate diagnosing and early interventions and treatment.
RATIONALE
In a primary care clinic in Fort Lauderdale, Florida, patients 18 years and older are not frequently assessed and screened for depression. Currently, at the clinic, there is no consistent routine for screening for depression. Providers randomly ask questions to patients they feel may have some issues with depression. A diagnosis of depression is often made based on the patient’s verbalized concerns and the physician’s clinical judgment. In addition, depression symptoms are often overlooked because patients 18 years and older may present to the clinic with other chronic conditions such as diabetes, stroke, cardiac, or thyroid disorders. According to Tait and Mitchell [18], failure of providers to recognize depression can have a harmful impact on the mental and physical health of patients. Depression is a high-risk factor for suicide, which is the second leading cause of death for adults worldwide who suffer from depression [18]. In primary healthcare settings, there continues to be no existing sustainable approach to healthcare providers’ consistent use of a depression screening protocol [19]. It is believed that introducing an evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool will increase the frequency of screening at a primary care clinic located in Fort Lauderdale, Florida. Currently, the providers are only asking questions from the Patient Health Questionnaire-2 (PHQ-2) depression questionnaire but are not asking questions from the Patient Health Questionnaire-9 (PHQ-9) depression questionnaire. The purpose of this project was to examine if the implementation of an evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool affected the frequency of screening at a primary care clinic located in Fort Lauderdale, Florida.
The long-term goal of the depression screening protocol was for healthcare providers to utilize the PHQ-9 tool 100% at annual, follow-up, and new patient visits. There were three phases of the project:
- The project sought to determine the frequency of depression screenings using the PHQ-9, prior to implementing a depression screening protocol designed to improve the number of depression screenings.
- After the frequency of depression screenings was determined, the evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool was implemented.
- Two weeks after the completion of implementing the depression screening protocol, the frequency of depression screenings using the PHQ-9 was re-assessed to determine if there was a significant difference in the frequency of depression screenings pre- and post-protocol implementation.
METHODS
Contextual Elements
Initiating improvements in the depression screening process at the primary care level can be accomplished with primary care physicians, clinical staff, and community health professionals. Making practice improvements within primary care using evidence-based treatment approaches assists in improving patient health outcomes. The solution to the current problem that exists in primary care is to adopt information from the USPSTF guidelines on “depression screening” and develop an evidence-based protocol that utilizes the Patient Health Questionnaire-9 (PHQ-9) screening tool [5].
Intervention
An evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool was developed. The depression screening project was implemented at a primary care clinic located in Fort Lauderdale, Florida. The clinic is a practice with one medical director, one physician, two nurse practitioners, and three medical assistants. The primary clinic provides primary and preventive care services, servicing approximately 60 patients daily and approximately 2,000 patients monthly. Implementation of the project consisted of five steps, which are listed as follows.
Development of Protocol
An evidenced-based depression screening protocol was developed by the researcher after review of the literature, utilizing the USPSFT guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool. A draft of the proposed depression screening protocol was emailed to Dr. Golaib, the clinical preceptor who is a nurse practitioner employed at the clinic, and discussed via telephone for feedback. A scheduled meeting was held with Dr. Golaib at the clinic to review the proposed protocol before presenting the protocol to clinical staff so that it meets the needs of the clinic.
Initiation of Project
A presentation was conducted with the clinic manager, physician, medical director, nurse practitioners, and medical assistants. This presentation included the project plan, a draft of the proposed depression screening protocol (for review and feedback), prevalence and implications of depression, review of the PHQ-9 tool and scoring guide (see Appendix B), USPSTF guideline recommendations for depression screening, treatment interventions, follow-up, referral criteria, and staff participation. In order to make sure the project’s process was effective, further discussion was held with the clinic staff regarding where depression screening would take place within the daily workflow of the clinic and how the collected depression screening data from the clinic’s EMR system would be stored. The medical director, physician, clinic manager, and nurse practitioners all agreed with the depression screening protocol (See Appendix C) and that depression screening would take place in the intake room. Collaboration of depression screening data storage was discussed with clinical staff, and it was determined that data would be stored in a locked cabinet in a locked room at the clinic, and only the clinical preceptor and the DNP student would have access to the depression screening data information. Implementation of the project began on January 9, 2020 and was completed on January 30, 2020.
Pre-Retrospective Chart Review
A retrospective chart review was conducted 2 weeks prior to pre-implementation of the PHQ-9 tool to 50 randomly selected patient charts by reviewing every third patient chart that meets the criteria of 18 years and older. Information was collected on (a) age, gender, race; (b) documentation of objective or reported symptoms associated with depression, such as sadness, poor appetite or overeating, poor concentration, suicidal ideation, anxiety or insomnia; (c) current or previous history of depression diagnosis; (d) treatment or referrals; and (e) if follow-up appointments were scheduled (see Appendix A). Patient information was de-identified.
Implementation of the Depression Screening Protocol
Implementation of data begins after collection of pre-implementation data from the EMR system. Patient intake was completed in an intake room by the medical assistants. Patients who met the project criteria, 18 years and older, who presented for annual, follow-up, or new patient visits were provided a copy of the PHQ-9 tool to complete. Once PHQ-9 questionnaire was completed, medical assistants placed the PHQ-9 questionnaire in a folder to be reviewed by providers. Providers reviewed completed PHQ-9 questionnaire, discussed results with patients, documented depression screening results in the EMR system, and if needed, developed a management plan that included treatment and referral.
Post Retrospective Chart Review
Two weeks after implementation of the depression screening protocol, a retrospective chart review was conducted, and post-implementation data information was also collected using a data collection form (see Appendix A). Fifty patient charts were randomly selected by choosing every third patient chart that meets the criteria of 18 years and older. Pre- and post-data collection were compared for differences.
Study of the Interventions
A quantitative pretest-posttest quasi-experimental study was chosen for this project. The goal of this project was to evaluate if there was significant difference in the proportion of patients who received the depression screening tool, PHQ-9, between the pre-implementation (before the protocol was implemented), and post-implementation (after the protocol was implemented). In order to test this effect, both a pretest and posttest measurement of depression was required.
MEASURES
The PHQ-9 questionnaire is one of the gold-standard tools used for screening for depression. The PHQ-9 is based on the DSM-IV diagnosis criteria for major depression and has shown to be valid and reliable after being widely utilized in numerous studies related to depression. The PHQ-9 is a nine-item questionnaire designed to screen for depression in primary care and other medical settings [20]. The standard age range to begin screening to identify depression is 18 years or older. One study by Mitchell et al. [21] investigated the validity and reliability of the PHQ-9 in a meta-analysis where publications were reported on 40 case studies. The PHQ-9-was linear and the PHQ-2 was significantly high. The sensitivity and specificity for the PHQ-9-linear were 81.3% and 85.3%, for the PHQ-2 was 75.9% and 89.3%, and the PHQ-9-algorithm was 56.8% and 93.3%, identifying that the PHQ-9 was found to have excellent clinical utility.
ANALYSES
A quantitative methodology was used to address the research questions. There were two research questions under examination in this project.
- Is there a significant difference in the proportion of patients who received the depression screening tool, PHQ-9, between the pre- and post-implementation? The null hypothesis stated that there is no significant difference in the proportion of patients who received the depression screening tool, PHQ-9, between the pre- and post-implementation.
- Is there a significant difference in depression screening scores, using the PHQ-9, between the pre- and post-implementation? The null hypothesis stated that there is no significant difference in depression screening scores, using the PHQ-9, between pre- and post-implementation.
Depression screening protocol evaluation of data was conducted comparing pre-and post-implementation data that include depression screening tool use. Data analyses were conducted comparing pre- and post-implementation data information extracted from the clinic’s EMR system on patients 18 years and older. Pre- and post-implementation data were entered in the SPSS software to analyze. The Chi-square t-test was used to compare and measure. Demographic information was identified using descriptive statistics such as frequencies, percentage, and measures of central tendency to summarize the sample demographics of pre- and post-implementation data.
ETHICAL CONSIDERATIONS
Patient records were selected for both the pre- and post-implementation phases using the nth sampling approach, where every third patient record was selected for inclusion in the project. All selected patient folders were assigned an ID number and no personally identifiable information was collected or used for this project. This ensured confidentiality of the patients. Once the data was collected, it was stored on a password-protected computer to prevent public access to data. Additionally, the data will be stored on a password-protected computer for at least three years once the project was completed.
RESULTS
Participants
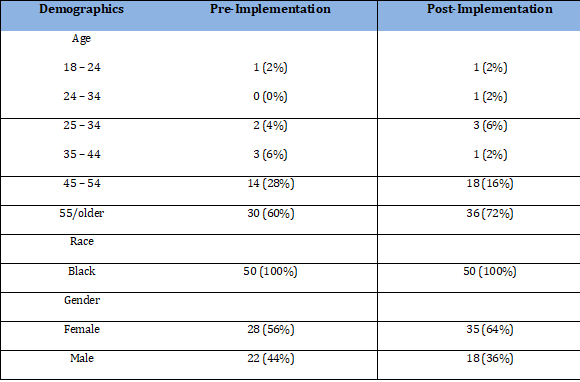
Frequencies and percentages were calculated for age, race, and gender and were separated by pre- and post-implementation of the protocol. For demographics pre-implementation, the most frequently observed category of age was 55/older (n = 30, 60%), the most frequently observed category of race was Black “B” (n = 50, 100%), the most frequently observed category of gender was female “F” (n = 28, 56%). For post-implementation demographics, the most frequently observed category of age was 55/older (n = 36, 72%), the most frequently observed category of race was Black (n = 50, 100%), and the most frequently observed category of gender was female (n = 32, 64%). Frequencies and percentages for demographics are presented in table 1.
Table 1: Frequency Table for Demographics.
RQ1: Is there a significant difference in the proportion of patients who received the depression screening tool, PHQ-9, between the pre-implementation (before the protocol was implemented), and post-implementation (after the protocol was implemented)?
The results of the Chi-square test of independence were significant based on an alpha value of 0.025, χ2(1) = 16.49, p < 0.001, suggesting that depression screening pre-implementation and post-implementation were associated with each other. There was adequate cell size, which requires all cells to have expected values greater than zero and 80% of cells to have expected values of at least five [22]. The following pre- and post-implementation data combinations had observed values that were greater than their expected values, and the following pre- and post-implementation combinations had observed values that were less than their expected values. Table 1 shows the results of the Chi-square test.
Table 2: Observed and Expected Frequencies of Depression Screening Before and After Protocol.

RQ2: Is there a significant difference in depression screening scores, using the PHQ-9, between the pre-implementation (before the protocol was implemented), and post-implementation (after the protocol was implemented)?
Using a two-tailed independent samples t-test, significant findings were calculated based on an alpha value of 0.05, t (54.00) = 4.19, p < 0.001, which indicates the null hypothesis can be rejected. This finding suggests the mean of the PHQ-9 score was significantly different between the pre-implementation and post-implementation categories of the depression screening tool, PHQ-9. In the post-implementation categories, the mean of PHQ-9 score was significantly higher than the mean of PHQ-9 score in the pre-implementation categories. The results are presented in table 3. A bar plot of the means is presented in figure 1.
Table 3: Two-Tailed Independent Samples t-Test for PHQ-9 Score.
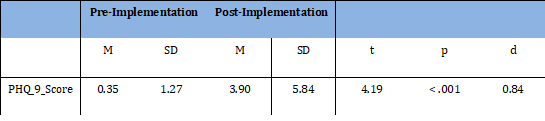
Note. N = 96. Degrees of Freedom for the t-statistic = 54.00. d represents Cohen's d.
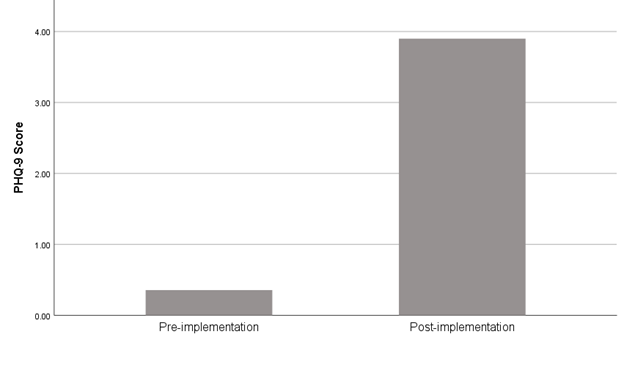
Figure 1: The Means of PHQ-9 Score by Pre- and Post-Implementation.
A two-tailed Mann-Whitney two-sample rank-sum test was conducted to examine whether there were significant differences in pre-data collection and post-data collection using the PHQ-9 tool. The result of the two-tailed Mann-Whitney U-test was significant based on an alpha value of 0.05, U = 1567, z = -4.14, p < 0.001. The mean rank for the group pre-implementation was 38.18, and the mean rank for group post-implementation was 56.84. These findings suggest that the distribution of PHQ-9 score for the pre-implementation group was significantly different from the distribution of PHQ-9 score for the post-implementation group. Pre-implementation median (Mdn = 38.18) was significantly lower than post-implementation median (Mdn = 56.84). Table 4 presents the results of the two-tailed Mann-Whitney U test.
Table 4: Two-Tailed Mann-Whitney Test for PHQ-9 Score.

DISCUSSION
Depression is a condition that is a major health concern within the United States that can have a huge effect on the patient and their family’s mental and physical wellbeing. Depression is a leading cause of disability worldwide [2]. Primary care providers are essential in recognizing and managing depression and at least 60% of mental health diagnoses occur in the primary healthcare setting [3]. So, having and effective and consistent depression screening protocol is vital to identifying and combating depression.
The purpose of this project was to examine if the implementation of an evidence-based depression screening protocol utilizing the USPSTF guidelines and the Patient Health Questionnaire-9 (PHQ-9) depression screening tool would affect the frequency of screening at a primary care clinic located in Fort Lauderdale, Florida. There were two research questions that were explored in this project. The first research question asked if there was a significant difference in the proportion of patients who received the depression screening tool, PHQ-9, between the pre-implementation (before the protocol was implemented), and post-implementation (after the protocol was implemented). Results indicated that there was a significant increase in proportion of patients who received the PHQ-9 depression screening tool after the protocol was implemented. The second research question asked if there was a significant difference in depression screening scores, using the PHQ-9, between the pre-implementation (before the protocol was implemented), and post-implementation (after the protocol was implemented). The results indicated that there was a significant increase in PHQ-9 depression screen scores after the protocol was implemented.
A recent study identified that less than 5% of adults in primary care are screened for depression [4]. Therefore, it was expected that there would be an increase in depression screening after the depression screening protocol was implemented. This is because having a protocol for conducting depression screening assists the healthcare professional in remembering to implement the depression screening, thereby increasing the consistency of the screening. The result of the study supported what was expected, as there was an increase in the application of the PHQ-9 depression screening tool.
According to the United States Preventive Service Task Force [5] and despite guideline recommendations, depression symptoms continue to be underdiagnosed in primary healthcare settings [4]. For example, lower scores on depression screening tools like the PHQ-9 indicate fewer depression symptoms. It was expected that there would be an increase in depression screening scores on the PHQ-9 after the depression screening protocol was implemented. Not only should the implementation of the depression screening protocol increase the consistency of depression screening, it should also improve the accurate implementation of the PHQ-9 depression tool. The results supported what was expected, as there was a significant increase in depression screening scores on the PHQ-9 after implementing the depression protocol. This indicated that the healthcare professionals were utilizing the tool more effectively, allowing fewer depression symptoms to go undiagnosed.
LIMITATIONS
There were several limitations associated with this project. First, the lack of ethical diversity, the clinic was located in and served an African American community. Given the ethnic homogeneity of the sample, the results of the effectiveness of implementing a depression protocol inside a health clinic may not be projectable to the general population that is more ethnically diverse. Second, most of the respondents in the project were elderly. This may adversely affect the projectability of the PHQ-9 results to the general population, which may suggest that elderly African Americans people are more depressed than the general population. Third, the pre and post-randomized sample size was small as well as the small number of healthcare providers who implemented the protocol. Finally, this was a high-volume local health clinic that saw approximately 2,000 patients per month. However, it is not known if the results would be the same for lower volume clinics, where there are fewer opportunities to perform the depression protocol.
CONCLUSIONS
Depression is a condition that is being recognized as a major health concern within the United States. According to WHO [2], depression is one of the leading causes of disability, and significantly impacts the economic well-being of the healthcare system. Depression is a mental illness linked to significant economic burden through direct and indirect costs and is associated with increased mortality due to suicide and impaired ability to manage other health issues [5]. Many patients suffering with mental disorders do not immediately seek care or talk with their provider, making it extremely important to comply with the USPSTF recommendations for screening for this disorder [23]. Primary care providers are essential in recognizing and managing depression and at least 60% of mental health diagnoses occur in the primary healthcare setting [3]. A significant primary step for refining the care of patients with depression in primary care, according to Smithson [13] is to develop, implement, and sustain a high-quality screening process. Accurate identification of depression may reduce depression symptoms and decreases clinical morbidity [3]. The benefit to screening for depression in adults 18 years and older is to ensure accurate diagnosis, effective treatment, and appropriate follow-up after screening. In addition, the economic burden of depression is substantial for individuals, as well as society and may include emotional suffering, reduced quality of personal relationships, possible adverse effects from treatment, numerous mental health and medical visits, time away from work, and lost wages. In addition, costs to society may include loss of life, and reduced productivity due to possible absenteeism from work. In primary care, proper training for providers and clinical staff can promote “adequate systems being in place” to ensure that patients are adequately screened, appropriately diagnosed, and provided proper treatment or referral. There continues to be gaps in practice relating to depression screening. These gaps may be related to assessing for depression using a protocol in primary care settings with more diverse populations and making sure that all depression questions, the PHQ-2, and PHQ-9 are discussed with the patient. Finally, additional research is essential to assess barriers to establishing adequate screening systems in primary care and how these barriers can be addressed.
REFERENCES
- Balanescu P, Botezat-Antonescu I, Dima C, Oana SC, Sorel E. (2016). Depression screening in primary care and correlations with comorbidities in Romania. International Medical Journal. 23(2):128-31.
- World Health Organization [Internet]. Geneva: WHO; 2020 [cited 09/01/2021]. Depression (fact sheet); [about 3 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
- Park TL, Zarate AC. (2019). Depression in the primary care setting. N Engl J Med. 380(6);559-68. doi:10.1056/NEJMcp1712493.
- Akincigil A, Matthews EB. (2017). National rates and patterns of depression screening in primary care: results from 2012 and 2013. Psychiat Serv. 68(7):660-6. doi:10.1176/appi.ps.201600096.
- United States Preventive Services Task Force [Internet]. USPSTF; 2016 [cited 08/17/2119]. Screening for Depression in Adults: US Preventive Services Task Force Re-commendation Statement. JAMA. 315(4):380-387. doi:10.1001/jama.2015.18392.
- Hedden SL, Copello EAP, Tice P, Hunter D [Internet]. Rockville, MD: Substance Abuse and Mental Health Services Administration, Department of Health & Human Services; 2015. Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health; [64 p]. Available from: https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf.
- Substance Abuse and Mental Health Services Administration [Internet]. Rockville, MD: SAMHSA; 2018. Mental and substance use disorders; [about 1 screen]. Available from: https://www.samhsa.gov/disorders.
- Raspolich J [Internet]. Fort Lauderdale: Vista Pines Health; 2021. Mental Health Treatment in Fort Lauderdale; [about 3 screens]. Available from: https://vistapineshealth.com/florida/fort-lauderdale/.
- Tracy N [Internet]. Healthy Place; 2019. Depression in Women: Understanding Female Depression; [about 6 screens]. Available from: https://www.healthyplace.com/depression/women/depression-in-women-understanding-female-depression.
- National Institute of Mental Health [Internet]. (2019). Arlington, VA: NAMI; 2019 [cited 09/17/2018]. Major depression; [about 7 screens]. Available from: https://www.nimh.nih.gov/health/statistics/major-depression.shtml.
- Melville NA [Internet]. Medscape; 2017 [cited 02/08/2018]. Depression screening in primary care still rare; [about 1 screen]. Available from: https://www.medscape.com/viewarticle/876075.
- Kato E, Borsky AE, Zuvekas SH, Soni A, Ngo-Metzger Q. (2018). Missed opportunities for depression screening and treatment in the United States. J Am Board Fam Med. 31(3):389-97. doi.org/10.3122/jabfm.2018.03.170406.
- Smithson S, Pignone M. (2017). Screening adults for depression in primary care. Med Clin N Am. 101(4):87–821. doi:10.1016/j.mcna.2017.03.010.
- Sivertsen H, Guro HB, Knut E, Geir S, Anne-Dofie H. (2015). Depression and quality of life in older persons: A Review. Dement Geriatr Cogn Disord. 40(5-6):311-39. doi:10.1159/000437299.
- Greensberg PE, Fournier A, Sisitskky T, Pike CT, Kesssler RC. (2015). The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J Clin Psychiatry. 76(2):155-162. doi:10.4088/JCP.14m09298.
- Hoff HS, Crawford NM, Mersereau JE. (2018). Screening for psychological conditions in infertile women: Provider perspectives. J Women’s Health. 27(4):503-509. doi:10.1089/jwh.2017.6332.
- Tu PC, Kuan YH, Li CT, Su TP. (2017). Structural correlates of trait impulsivity in patients with bipolar disorder and healthy controls: a surface-based morphometry study. Psychol Med. 47(7):1292–1299.
- Tait L, Mitchell M. (2014). Educational intervention for general practitioners to identify and mange depression as a suicide risk factor in young people: A systemic review and eta-analysis protocol. Syst Rev. 3(145). doi.org/10.1186/2046-4053-3-145.
- Flynn HA, Spino C, Guille C, Deligiannidis KM, Maki P, et al. (2018). A collaborative, network-based approach to advance women's depression research in the United States: Preliminary findings. J Women's Health. 27(1):51-7. doi:10.1089/jwh.2016.6261.
- Moriarty AS, Gilbody S, McMillan D, Manea L. (2015). Screening and case finding for major depressive disorder using the Patient Health Questionnaire (PHQ-9): A meta-analysis. Gen Hosp Psychiatry. 37:567-76. doi:10.1016/j.genhosppsych.2015.06.012.
- Mitchell AJ, Yadegarfar M, Gill J, Stubbs B. (2018). Case finding and screening clinical utility of the Patient Health Questionnaire (PHQ-9 and PHQ-2) for depression in primary care: A diagnostic meta-analysis of 40 studies. Br J Psychiatry. 2(2):127-38. doi:10.1192/bjpo.bp.115.001685a.
- Rana R. (2015). Chi-square test its applicability in hypothesis testing. J Pract Cardiovasc Sci. 1(1):69-71. doi:10.4103/2395-5414.157577.
- Centers for Disease Control and Prevention. (2018). Surveillance for certain health behaviors and conditions among states and selected local areas: Behavioral risk factor surveillance system, United States, 2015. MMWR. 67(9):1-90.