Information Links
Related Conferences
Previous Issues Volume 10, Issue 2 - 2025
Giant Lt Intrahepatic Stone Causing Severe Cholangiohepatitis, treated Surgically: Case Report
Salah Termos1,*, Yasmeen Alshahoumi1, Nour Abul1, Mohammad AM Qasem1, Ali A Alali2, Afaq Alkhalil1, Bader MS Albader1, Fahad Alabdulghani3, Yosor Alqudeimat3
1Department of Surgery, Amiri Hospital, Kuwait
2Department of Gastroenterology, Amiri Hospital, Kuwait
3Department of Radiology, Amiri Hospital, Kuwait
*Corresponding Author: Salah Termos, MD FACS, Consultant HPB Surgeon, Department of Surgery, Amiri Hospital, Kuwait, Email: [email protected]
Received Date: May 03, 2025
Published Date: May 30, 2025
Citation: Termos S, et al. (2025). Giant Lt Intrahepatic Stone Causing Severe Cholangiohepatitis, treated Surgically: Case Report. Mathews J Gastroenterol Hepatol. 10(2):32.
Copyrights: Termos S, et al. © (2025).
ABSTRACT
Background: Recurrent pyogenic cholangitis (RPC) is a chronic hepatobiliary disease characterized by the formation of intrahepatic biliary stones, leading to inflammatory strictures and progressive obstruction of the biliary tree. This pathogenesis can result in recurrent episodes of cholangitis. Although it more commonly observed in east and southeast Asia, it remains rare in Gulf region. The disease exhibits a spectrum of clinical manifestations ranging from asymptomatic to mild and severe presentation to potentially life-threatening conditions. Aim: We report the case of a giant intrahepatic stone causing RPC to highlight the importance of multidisciplinary approach in such complicated illness despite the paucity of its presentation in Arab countries. Available therapeutic options include non-surgical endoscopic approaches and surgical from drainage up to hepatectomy and biliary reconstructions. Methods & Result: We describe the case of a 45-year-old male patient who presented with a picture of obstructive jaundice associated with fever and raised liver enzymes. MRCP demonstrated a 5.5 cm left intrahepatic stone with dilated biliary radicals. ERCP succeeded to drain the common bile duct however failed to clear left hepatic duct and intrahepatic biliary system. Patient underwent left hepatectomy with uneventful outcome. Conclusion: Hepatolithiais is an uncommon liver pathology in non-Asian areas. It can cause serious complications and consequent cholangiocharcinoma. Management primarily focuses on complete stone removal and correction of associated biliary stricture. However, in selected cases hepatectomy may be warranted as a definitive therapeutic option.
Keywords: Recurrent Pyogenic Cholangitis (RPC), Cholangiohepatitis, Hepatolithiasis, Intrahepatic Stone, Endoscopy, Obstructive Jaundice.
INTRODUCTION
Hepatolithiasis is defined as the presence of stones in the bile ducts proximal to the confluence of the right and left hepatic ducts. It occurs more common in females with a disease predilection in the left hepatic lobe. This condition can occur even in the absence of the gallstones in the common bile duct or gallbladder [1]. Though the exact etiology of hepatolithiasis is not fully understood, risk factors and diagnostic approaches can contribute to better outcomes for patients presenting with RPC. Intrahepatic lithiasis is classified by composition into calcium bilirubinate and cholesterol stones. Calcium bilirubinate predominantes approximately 75% of cases [2].
RPC can range from being asymptomatic to cholangitis, abscess formation and liver cirrhosis [3,4]. Primary treatment goal for intrahepatic duct stones is complete biliary ducts clearance and stricture correction to prevent recurrent cholangitis [5]. Hepatectomy can be an effective treatment by removing affected liver tissue and eliminating the risk of malignancy [6]. Herein, we report the case of RPC in an Arab country secondary to a giant left intrahepatic bile duct managed by endoscopic common bile duct stone clearance followed by left hepatectomy.
CASE PRESENTATION
A 45-year-old male patient known to have diabetis mellitus was referred to our hepatobiliary unit for RPC secondary to hepatolithiasis. Patient reported recurrent bouts of right upper quadrant accompanied by insidious epigastric pain that had recently become continuous and was associated with fever and obstructive jaundice. Patient reported a surgical history of an open cholecystectomy at the age of 15 years and absent family history of cholangiohepatitis.
Physical examination noted high-grade fever, evident obstructive jaundice, right upper quadrant tenderness and a Kocher incision scar. Blood analysis revealed a white blood cell count of 13.4×109/L, alkaline phosphatase (ALP) of 430U/L, gamma-glutamyl transferase (GGT) of 340 U/L, total bilirubin of 38.5 µmol/L, and alanine aminotransferase (ALT) of 95U/L. Tumor marker Ca19.9 was elevated.
Ultrasonography showed a suspicious left hepatic duct stone with a dilated common bile duct and left biliary radicals. A contrast enhanced computed tomography scan of the abdomen and pelvis demonstrated an atrophic left lobe with multiple hypodense liver lesions suggestive of stones, particularly in segments II and III, with the largest measuring approximately 4 cm, likely representing a liver abscess with a cluster sign due to recurrent pyogenic cholangitis (Figure 1). MRCP confirmed evidence of a dilated left intrahepatic bile duct with multiple stones, associated with edema of the left liver lobe, findings consistent of oriental cholangiohepatitis. The common bile duct was dilated with multiple small stones (Figure 2). Patient underwent ERCP using Spyglass that failed to opacify the Left IHBR by to complete obstruction of the LHD due to giant stone. CBD clearance was performed with plastic stent insertion (Figure 3).
.png)
Figure 1. Axial and Coronal portal venous phase CECT showing a large stone in a peripheral segment II duct (star), which is dilating and causing obstruction of the duct and dilatation of the segmental duct distal to the stone (arrow).
.png)
Figure 2. MRI liver image showing stones, dilatation and edema (Cluster Sign), in a segment II bile duct (star).
.png)
Figure 3. MRCP MIP image showing the large stones (star) in the peripheral duct of segment II; there is also narrowing / stricture of the common hepatic duct (arrow).
After multidisciplinary meeting, a decision was taken to proceed surgical intervention. Diagnostic laparoscopy revealed numerous adhesions in the portahepatis, liver and adjacent structures. Adhesiolysis was performed and access was attained to all the important elements. Inflow and outflow were controlled. Pringle’s maneuver was used for parenchymal dissection along the demarcation zone. Difficulty was encountered at the LHD junction due to a giant stone at the LHD extending to the confluence that necessitated the addition of a hand assisted port to complete the procedure through a small midline incision. Left hepatectomy was performed under ultrasound guidance showing diseased bile ducts with intrahepatic stones (Figure 4). Doppler ultrasound confirmed patent flow in the right hepatic artery and portal vein. Large intrahepatic stone measured 5.5 cm in size was extracted from the specimen (Figure 5). Histopathology revealed acutely and chronically inflamed liver tissue, fibrosis and hepatolithiasis, with no evidence of malignancy. Repeat ERCP was done and stent was removed after 8 weeks (Figure 6). Patient was maintained on ursodeoxycholic acid and low fat diet. 6 months follow up noted normal liver enzymes and CA 19.9. The imaging study was unremarkable (Figure 7).
.png)
Figure 4. ERCP revealing large stone obstructing the LHD (star), Deployment of biliary stent (arrow).
.png)
Figure 5. Left Hepatectomy demonstrating atrophic segments with diseased ducts filled with stones.

Figure 6. Large left intrahepatic stone.
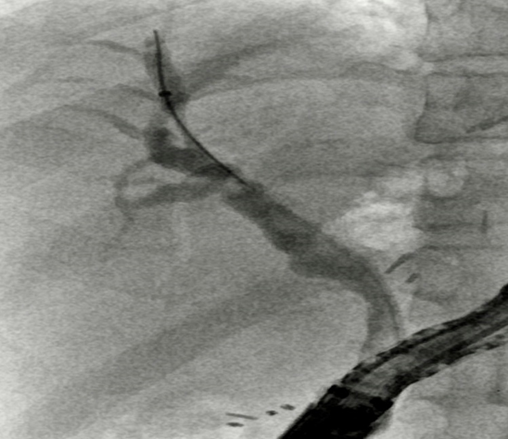
Figure 7. Repeat ERCP and stent removal.
DISCUSSION
Recurrent pyogenic cholangitis, also known as Hong Kong disease or oriental hepatitis. It presents a complex clinical challenge due to longstanding repeated inflammation of the biliary tree. Historically prevalent in East and Southeast Asia and other regions endemic to trematodes infections, the reported rates of RPC in these areas range from 30% to 50% [7,8]. However, the global migration phenomenon has contributed to the rise of RPC cases worldwide, this shift highlights the importance of considering RPC as a potential diagnosis, regardless of geographic location [9].
The lack of standardized nomenclature, combined with diverse clinical presentations, and evolving endemic patterns, complicates the accurate diagnosis of RPC. Etiology is usually due to various contributing factors, including cholestasis and stones, bacterial infection, liver fluke infestations, anatomic defect of biliary tract and metabolic abnormalities [10]. A study in China on genetic mutations and hepatolithiasis identified a connection between Pst-I polymorphism of the mucin 4 gene and primary hepatolithiasis [11].
Complications of RPC can range from acute issues such as ascending cholangitis to long-term problems like stone recurrence, liver atrophy, biliary cirrhosis and even carcinogenesis [12-14]. Among these, the most concerning complication is the development of cholangiocarcinoma, reported incidence of 4% to 11%. Lifelong monitoring is essential even after stone removal. Therefore, further research exploring the relationship between hepatolithiasis and cholangiocarcinoma is crucial, including identifying risk factors, growth factors, and treatment methods to predict malignant transformation [15].
A study in China suggested that hepatoma-derived growth factor (HDGF) may serve as an early indicator for hepatolithiasis-associated intrahepatic cholangiocarcinoma, while markers such as VEGF and MUC5B were identified as potential indicators for disease progression and prognosis [16]. Postoperative formation of Segmental atrophy, biliary strictures and residual stones are additional risk factors for hepatolithiasis-associated cholangiocarcinoma [17]. Smoking, family history of cancer and a duration of symptoms longer than 10 years may also increase the risk of developing intrahepatic cholangiocarcinoma [18].
Treatment of hepatolithiasis involves a range of approaches, often requiring a multidisciplinary team that includes gastroenterologists, interventional radiologists, and hepatobilliary surgeons. Less invasive methods include percutaneous transhepatic one-step biliary fistulation (PTOBF) with cholangioscopic lithotripsy, traditional percutaneous transhepatic cholangioscopy (PTCSL) and endoscopic retrograde cholangiopancreatography (ERCP). Studies comparing 3D-PTOBF lithotripsy to conventional 2D-PTOBF approach show that the former results in superior outcomes, with shorter hospital stays and shorter operation times [19]. The removal of impacted stones remains the primary goal of endoscopic intervention, while emerging methods like lithotripsy and bile duct exploratory lithotomy continue to improve care, especially when surgery is not feasible.
Despite the absence of standardized approaches and lack of expertise due to the paucity of patient numbers in the Gulf region we elected to proceed with endoscopic CBD clearance using Spyglass technique followed by Lt hepatectomy. Surgical intervention is generally favored for optimal outcomes, with emphasis on restoring the biliary tract system and addressing any residual stones. There is little to no significant difference between laparoscopic hepatectomy and open hepatectomy. However, when comparing resection with T-tube drainage versus resection and bile duct-intestinal anastomosis, recurrence rates were 50% and 22% respectively, and re-operation rates were 28% and 8.3% respectively [20].
Oriental hepatitis in Arab patients is uncommon. ERCP with or without lithotripsy usually is the first line treatment. However, the exceptional size of the intrahepatic stone 5.5cm had directed our plan toward combined endoscopy followed by hepatectomy.
CONCLUSION
Hepatolithiasis is a serious medical condition that lead to recurrent pyogenic cholangitis. Presence of larger stones causing complete hepatic ducts obstruction can pose substantial challenges especially in non-endemic countries. MRCP is the gold standard for diagnosis and planning. We recommend multi-disciplinary approach to establish appropriate management. Surgical resection in certain cases remains the superior treatment option in terms of lower recurrence rates, eradication of residual stones or strictures or any possible malignant transformation.
ACKNOWLEDGEMENT
We thank our hepatobiliary unit for their continuous care and support.
CONFLICT OF INTERESTS
Authors declare that there is no conflict of interest.
SOURCES OF FUNDING
This case report received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
ETHICS APPROVAL
Our institution does not require ethical approval for reporting individual cases or case series.
CONSENT
A verbal and a written consent were taken from the patient directly prior to publishing information or images.
REFERENCES
- Tsunoda T, Imazu H, Mori T, Okano K, Sugiyama M, Yasui K, et al. (1989). Hepatolithiasis in Japan: present status. HPB Surg. 1(1):1-10.
- Freise J, Mena J, Wen KW, Stoller M, Ho S, Corvera C. (2020). A rare presentation of hepatolithiasis in an adolescent patient: a case report. Int J Surg Case Rep. 72:343-345.
- Adhikari L, Achhami E, Bhattarai N, Kandel A, Shrestha AB. (2022). Diagnosis and management of hepatolithiasis in an adult patient: a case report. Ann Med Surg (Lond). 82:104788.
- Lee BS, Kim TH, Kim KH, Kim TN, Kim SH, Kim KH, et al. (2018). Clinical features and outcomes of hepatolithiasis: a single-center experience. Korean J Gastroenterol. 71(5):247-254.
- Lee TY, Cheon YK, Noh SH, Moon JH, Lee JS, Shim CS. (2015). The role of percutaneous transhepatic cholangioscopy in the management of hepatolithiasis: long-term results. Korean J Intern Med. 30(1):59-65.
- Liu CL, Lo CM, Fan ST. (2006). Hepatic resection for hepatolithiasis: a comparative study of left lobectomy and left lateral segmentectomy. J Am Coll Surg. 203(2):245-249.
- Motta RV, Saffioti F, Mavroeidis VK. (2024). Hepatolithiasis: Epidemiology, presentation, classification and management of a complex disease. World J Gastroenterol. 30(13):1836-1850.
- Jeyarajah DR. (2004). Recurrent pyogenic cholangitis. Curr Treat Options Gastroenterol. 7(2):91-98.
- Kim KH, Kim TN, Kim KH, Kim SH, Kim KH, et al. (2018). Clinical features and outcomes of hepatolithiasis: a single-center experience. Korean J Gastroenterol. 71(5):247–54.
- Termos S, Alali M, Alkabbani M, AlDuwaisan A, Alsaleh A, Alyatama K, et al. (2017). Gallbladder Mucus Plug Mimicking Ascaris Worm: An Ambiguous Cause of Biliary Colic. Case Rep Surg. 2017:7167934.
- Zhang Y, Li Z, Wang Y, et al. (2022). Significance of expressions of HDGF, VEGF and mucin 5B in hepatolithiasis associated with intrahepatic cholangiocarcinoma. Chin J Hepatobiliary Surg. 28(12):97-102.
- Termos S, Al Duwaisan A, Alali M, Faour H, AlHomoud H, Alsaleh A. (2017). Gallbladder-associated symptomatic hepatic choristoma: Should you resect? Int J Surg Case Rep. 41:243-246.
- Chen W, Huang Z, Zhang L, et al. (2022). Risk factors of intrahepatic cholangiocarcinoma in patients with hepatolithiasis: a case-control study. J Gastroenterol. 57(5):372-380.
- Wang Y, Li Z, Wang Z, et al. (2023). Percutaneous transhepatic choledochoscopy in the management of hepatolithiasis: a narrative review. World J Gastroenterol. 29(13):1836-1849.
- Hussain J, Alrashed AM, Alkhadher T, Wood S, Behbehani AD, Termos S. (2018). Gall stone ileus: Unfamiliar cause of bowel obstruction. Case report and literature review. Int J Surg Case Rep. 49:44-50.
- Termos S, Mohammad I, Khaled A, Khadija A, Munerah A, et al. (2024). Heterotopic hepatic tissue on gallbladder: A rare incidental finding. J Clin Med Images Case Rep. 4(5):1742.
- Huang Z, Chen W, Zhang L, et al. (2022). Predictive factors for subsequent intrahepatic cholangiocarcinoma associated with hepatolithiasis: Japanese National Cohort Study for 18 years. J Gastroenterol. 57(5):372-380.
- Feng X, Li J, Zhang J, Zhang L, Zhang Y, Wang Y, et al. (2020). The ultrasonic navigation technique in percutaneous transhepatic one-step biliary fistulation with rigid cholangioscopic lithotripsy for complicated hepatolithiasis. Chin J Hepatobiliary Surg. 26(12):103-107.
- Termos S, Alrashidi M, Alrushaidan S, Alqudeimat Y, AlBader MSB, Almojil K, et al. (2024). Strawberry Gallbladder: A Distinctive Type of Cholesterolosis Case Report and Literature Review, Ann Med Clin Cas Rept. 1(2):1.
- Zhang J, Li J, Zhang L, Zhang Y, Wang Y, et al. (2021). Three-dimensional visualization technology in one-stage establishment of a percutaneous transhepatic biliary tract in treatment of complex hepatolithiasis. Chin J Hepatobiliary Surg. 27(12):509-512.