Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2025
Gastrointestinal Complications after Ventriculoperitoneal Shunt for Pediatric Hydrocephalus: A Case Report and Literature Review
Badr Drai*, Yassine Ait M’barek, Lamia Benantar, Khalid Aniba
Ibn Tofail Neurosurgery Department, Mohamed VI University Hospital, Marrakech, Morocco
*Corresponding Author: Dr. Badr Drai, Ibn Tofail Neurosurgery Department, Mohamed VI University Hospital, Marrakech, Morocco, Phone: +212635265794, E-mail: [email protected]
Received Date: February 04, 2025
Published Date: February 19, 2025
Citation: Drai B, et al. (2025). Gastrointestinal Complications after Ventriculoperitoneal Shunt for Pediatric Hydrocephalus: A Case Report and Literature Review. Mathews J Surg. 8(1):36.
Copyrights: Drai B, et al. © (2025).
ABSTRACT
Ventriculoperitoneal shunt (VPS) surgery is a common procedure for pediatric hydrocephalus, which can lead to gastrointestinal complications such as catheter blockage, shunt infection, and distal catheter extrusion. Current problems include blockage, dysfunction, malposition, or catheter and valve infection, resulting in recurrent admissions to hospitals. Risk factors include hydrocephalus type, age, male sex, and socioeconomic status. The incidence of abdominal problems following VPS ranges between 5% and 47%, with the GI tract corresponding to the vast majority of the abdominal cavity problems. The pediatric population is more prone to these problems due to thinner bowels and more dynamic peristalsis. A case report from the Mohamed VI University Hospital Center in Marrakech evaluated the impact of VPS on the gastrointestinal tract and to determine severity of these effects even with doses less alarming than normally seem necessary. Problems in the upper GI tract involvement from the mouth cavity to stomach but lower problems belong to both small and large intestine as well as rectum and anus. VPS perforations often occur in the colon, leading to complications such as cerebral subdural abscesses, colon obstruction, abdominal distension, and bilious vomiting. Early diagnosis and treatment are crucial, as the most common pathogen found is Escherichia coli. Treatment includes surgery, antibiotic therapy, and laparoscopy. Children often develop transanal protrusion due to tube migration and bowel perforations. Despite the rarity of the condition, practitioners should be aware of potential issues in the gastrointestinal system and ensure early diagnosis and treatment.
Keywords: Hydrocephalus, VPS, Pediatric, GIT Complications.
INTRODUCTION
Among the most common procedures carried out on children at every neurosurgery institution is ventriculoperitoneal shunt (VPS) surgery. A wide range of problems, such as straightforward catheter blockage, shunt infection, and distal catheter extrusion through the oral cavity, urethra, anal canal, abdominal wall, cervical area, etc., have been documented in the literature [1-3]. Ten percent is the documented occurrence of distal catheter migration [4]. Rare side effects from ventricular catheters include subdural and extradural hematomas, pneumocephalus, and intraventricular hemorrhage [5].
Ventriculoperitoneal shunts are among the most common neurosurgical procedures performed on children. The literature documents a plethora of potential issues with these shunts, including simple catheter obstructions, infections of the shunt itself, and extrusion of the distal catheter through unlikely orifices like the mouth, urethra, anus, abdominal wall, or neck [1-3]. Migration of the distal catheter occurs in approximately 10% of cases according to records [4].
Rarely, ventricular catheters have caused subdural hematomas, pneumocephalus, or intraventricular hemorrhaging [5]. While shunts effectively treat hydrocephalus, their use introduces a lifelong risk of complications that require diligent monitoring and treatment to avoid debilitating issues. Neurosurgeons continually innovate shunt designs to minimize obstruction and migration risks while maximizing longevity, but occasional revision surgery remains inevitable for many pediatric patients. Hydrocephalus is a challenging pathology that accounts for nearly half of pediatric neurosurgical unit admission. The VPS has been developed over time to drain cerebrospinal fluid efficiently. Common complications include catheter and valve obstruction, malfunction, malposition, or infection, leading to multiple hospital admissions [6]. Risk factors include hydrocephalus type, age, male sex, and socioeconomic status. The revision rate is high, reaching 84.5% in some patient populations [7].
After VPS placement, the incidence of abdominal issues varies from 5% to 47%, with the GI tract accounting for the great majority of digestive issues. Clinicians must be aware of the potential injuries in this area [8,9]. The pediatric population is more prone to these problems due to thinner bowel walls and more dynamic peristalsis. The morphology of their intestinal musculature and the GI tract's morphology contribute to the risk of perforation.
The evaluation of the impact of VPS insertion on the gastrointestinal tract (GI tract) was the goal of this narrative review and our case report. The severity of those effected and determining the management strategies that have been documented in the literature. Upper GI tract perforations may affect tissues from the mouth cavity to the stomach, while lower GI tract disorders affect the small and large bowels, as well as the rectum and anus. Furthermore, more occasionally, hepatic and cholecystic disease has been described as a result of VPS placement.
CASE REPORT
In our daily practice within the neurosurgery department at the Mohamed VI University Hospital Center of Marrakech, the entire team has become accustomed to managing newborns with malformative or post-meningitic hydrocephalus, in which gastrointestinal problems are still quite uncommon. A 7-month-old boy who had a history of bacterial meningitis at the age of 2 months, complicated by hydrocephalus, had undergone a VPS following the sterilization of the CSF and the return of normal protein content. This was the first case that was encountered over a two-year period, from 2021 to 2023. The patient was brought by his family with a presentation of digestive disorders consisting of vomiting and acute diarrhea, with a fever measured at 38.9. The clinical examination found the distal end of the catheter protruding through the anus (Figure 1). The management of this complication consisted of a biological exploration, which revealed a high CRP, with leukocytosis predominantly of neutrophils. In partnership with pediatric surgeons, the DVP was removed in an emergency, and it was discovered that the appendix was the site of the digestive perforation (Figure 2). The postoperative period was uneventful. The follow-up of the patient's hydrocephalus was normal and it was done through monitoring of the cranial perimeter, neurological examination, and radiological control of ventricular dilation.
The second case was of a male infant aged 8 months, who had a history of hydrocephalus due to congenital stenosis of the Sylvian aqueduct, diagnosed at the age of 3 weeks, and treated with a VPS at the age of 2 months. His parents brought him in after observing the catheter's distal end sticking out through the anus (Figure 3). The infant's clinical checkup came back normal. The surgical management consisted of removing the VPS during which the digestive perforation involved the transverse colon, and the intestinal defect was repaired after VPS removal (Figure 4). The placement of a second valve on the contralateral side was performed due to the beginning of an intracranial hypertension syndrome after 6 weeks.
.png)
Figure 1. The distal part of the VPS coming out through the anus in a 7-month-old boy.
.png)
Figure 2. Intraoperative image of a trans-appendicular perforation by the distal end of the VPS.

Figure 3. An 8-month-old boy's distal portion of the VPS emerging through the anus.
.png)
Figure 4. Post-operative picture of the VPS's distal end following ablation.
DISCUSSION
Oral complications
A VPS distal catheter transoral migration is a rare occurrence (Figure 5); the first instance was reported in 1987 in a 10-year-old child who had post-tuberculous hydrocephalus [10]. After the shunt was replaced with a ventriculoatrial (VA) shunt, the patient passed away due to related complications. The etiology of this syndrome includes intraabdominal processes, such as stomach or jejunal perforation, which might involve the oral cavity by perforating the trachea. We present the case of an 8-month-old female patient who underwent a shunt placement for communicating hydrocephalus and was readmitted 6 months later for respiratory distress and choking. The distal shunt in the trachea was identified at the time of revision surgery; thus, it needed to be removed and a shorter one reinserted [11]. Ghritlaharey [12] reviewed 22 patients with this kind of complications in 2016, 20 of whom were child and this problem has been reported subsequently.

Figure 5. VP shunt distal end oral extrusion [13].
Gastric complications
Although they are less common than in adults, a few occurrences of stomach lesions in children have been described. First, it has been documented that children who have VPSs may experience stomach perforations anytime from a few months to several years
following placement. Four months following the treatment, an infant with a VPS showed signs of acute malnutrition and an enlarged head circumference. Six centimeters into the stomach, the shunt tip was discovered and extracted [14]. Second, another intraoperative complication was gastric perforation. Due to Dandy-Walker deformity and a history of ileostomy insertion during abdominal surgery for necrotizing enterocolitis, a young patient needed shunting for hydrocephalus. After externalizing the shunt, the patient was treated with gentamicin and ampicillin. At the four-month follow-up, no problems were found, and a week later, the VPS was swapped out for a VA shunt [15].
VPSs have been found, in asymptomatic individuals, in the stomach, suggesting the stomach's potential as a CSF draining location [16]. Alther suggested the ventriculogastric shunt in 1965 [17,18], and Jurkiewicz proposed resuscitation of these draining techniques in 2012 [19]. While some VPSs related to perforations have no significant effects under certain conditions, the technique has not been used as a substitute for CSF derivation due to risks such as ascending infection, stomach acid leakage in the peritoneum, or distal shunt dislodgement.
Small intestine complications
Small intestine perforation is a frequent consequence of VPS in children, affecting several areas including the ileum and jejunum [20,21]. In contrast to stomach perforations, which cause the shunt to migrate into the mouth, small intestinal injuries can cause transanal and transoral protrusion [22]. The majority of patients get well with the right care, which involves a laparotomy, removal of the shunt, switching to temporary external ventricular drainage, systemic and intrathecal antibiotics, and finally replacing the shunt, involving the atrium or peritoneum [23]. One major consequence of perforations is bacterial contamination of the shunt, which causes meningitis and peritonitis. Infections with Escherichia coli, Staphylococcus epidermidis, Serratia marcescens, and Proteus mirabilis have been reported, with the last being linked to spontaneous bacterial peritonitis [24].
Intestinal obstruction, a condition resulting from VP shunting, can lead to various consequences, including volvulus and mechanical obstruction. In a case of an 11-month-old with hydrocephalus and myelomeningocele, the shunt was surgically removed due to a gas fluid level in the intestines. The bowel was found to be surrounding the shunt with 2.5 turns around it, forming a volvulus. The shunt was then placed in the subhepatic space, but it had to be removed due to Klebsiella pneumoniae contamination. The shunt became immobile, allowing the intestine to coil [25]. Mechanical obstruction might result in shunt dysfunction or severe blockage, necessitating quick medical treatment. In a case of a 3-month-old with hydrocephalus and Chiari II malformation, a distal catheter knotted around the small intestine, which produced ischemia and necrosis [26]. A small-bowel resection was performed, followed with an ileostomy and replacement with a VA derivation. Small-bowel obstruction may occur from a variety of additional VPS related conditions, including inadequate removal of the distal catheter from the abdomen, sclerosing encapsulating peritonitis, and pseudodocysts that cause some degree of obstruction. There is no established consensus on how to handle these circumstances.
Colonic complications
VPS perforations, frequently occur in the colon, with little abdominal peritonism and shunt dysfunction in certain cases. In one case, CSF from a pseudocyst contained E. coli and Streptococcus fecalis, and the contrast substance injected into the shunt revealed a gap in the ascending colon. The treatment included colon wall repair, laparotomy, removal of the distal catheter, and antibacterial drugs [27]. In a different case, Pseudomonas aeruginosa and K. pneumoniae, both of which were subsequent to the colonic damage, contaminated the shunt. Colon radiography, CT, and shuntograms have been observed in studies, and early diagnosis is crucial. The most frequent pathogen found in these circumstances is Escherichia coli [28]. Rarely, the patient has no symptoms and distal catheters poke through the anus [29].
Abdominal distension, bilious vomiting, cerebral subdural abscesses, colon blockage from volvulus, and 48 hours of no bowel movement are among the problems that might result from a colon perforation [30]. For 48 hours, a 21-month-old child with a VPS had no stool activity, bilious vomiting, and abdominal distension. Bowel derotation and colopexy were used as management of this case, and the shunt failure was attributed to severe constipation [31]. After conservative treatments to remove the involved colon, two juvenile cases of shunt dysfunction linked to abdominal distension were resolved [32]. Knuth J et al. had reported a case of a VP distal catheter that has been dislodged in the colon which was successfully removed using other techniques, such as laparoscopy [33].
Children frequently develop transanal protrusion as a result of tube migration and small or large bowel perforations [34]. Although the diagnosis is simple, but initial discomfort can be mistaken for ascariasis [35]. The vast majority of cases have been effectively handled, with no significant problems. Most instances have been identified with sterile CSF cultures [36], There were, however, some more critical situations that needed further treatment.
For instance, a 2-month-old child was treated for methicillin-resistant Staphylococcus aureus meningitis [37]. Ghritlaharey et al.'s case series revealed a patient with congenital hydrocephalus experiencing a worsening of his intracranial pressure [38]. Treatment options for this case included laparotomy, distal shunt revision, intestinal wall repair, laparoscopy, shunt removal and external ventricular drainage (Figure 6), and pediatric colonoscopy to find and removing the distal catheter [39,40].
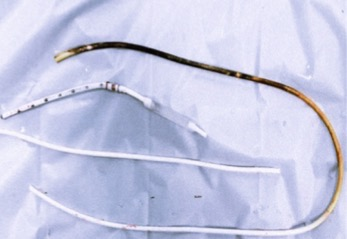
Figure 6. Fecal pigmentation of the abdominal part of the VPS, resulting of long-term intraluminal colonic content exposure [13].
CONCLUSION
While being a rarely diagnosed condition, medical professionals must stay informed on potential postoperative complications involving the gastrointestinal tract following VPS implantation. Ensuring vigilant care through prompt determination and targeted treatment can meaningfully impact a patient’s outcome. Therefore, age is still an important consideration when evaluating for diagnosis since incidence varies greatly between pediatric versus adult cases. They vary in severity, and displayed symptoms similar to all types of abdominal pathology. Once these issues have been diagnosed, they often require a multidisciplinary team of specialists, led by a pediatric neurosurgeon, gastroenterologist, pediatrician, and general surgeon, to manage and device, which could include either replacement or repair.
ACKNOWLEDGMENTS
None.
CONFLICTS OF INTEREST
The authors declare there is no conflict of interest.
REFERENCES
- Paff M, Alexandru-Abrams D, Muhonen M, Loudon W. (2018). Ventriculoperitoneal VD complications: A review. Interdiscip Neurosurg. 13:66-70.
- Wu Y, Green NL, Wrensch MR, Zhao S, Gupta N. (2007). Ventriculoperitoneal shunt complications in California: 1990 to 2000. Neurosurgery 61(3):557-562.
- Vankipuram S, Jaiswal S, Jaiswal M, Bajaj A, Chandra A, Ojha BK. (2017). Spontaneous Umbilical CSF Fistula Due to Migration of the Peritoneal End of VP Shunt: A Case Report and Review of Pathogenesis. J Pediatr Neurosci. 12(3):285-287.
- Kast J, Duong D, Nowzari F, Chadduck WM, Schiff SJ. (1994). Time-related patterns of ventricular shunt failure. Childs Nerv Syst. 10(8):524-528.
- Kalia KK, Swift DM, Pang D. (1993). Multiple epidural hematomas following ventriculoperitoneal shunt. Pediatr Neurosurg. 19(2):78-80.
- George R, Leibrock L, Epstein M. (1979). Long-term analysis of cerebrospinal fluid shunt infections. A 25-year experience. J Neurosurg. 51(6):804-811.
- Stone JJ, Walker CT, Jacobson M, Phillips V, Silberstein HJ. (2013). Revision rate of pediatric ventriculoperitoneal shunts after 15 years. J Neurosurg Pediatr. 11(1):15-19.
- Esposito C, Porreca A, Gangemi M, Garipoli V, De Pasquale M. (1998). The use of laparoscopy in the diagnosis and treatment of abdominal complications of ventriculo-peritoneal shunts in children. Pediatr Surg Int. 13(5-6):352-354.
- Lortat-Jacob S, Pierre-Kahn A, Renier D, Hirsch JF, Martelli H, Pellerin D. (1984). Complications abdominales des shunts ventriculo-péritonéaux chez l'enfant. 65 observations [Abdominal complications of ventriculo-peritoneal shunts in children. 65 cases]. Chir Pediatr. 25(1):17-21.
- Griffith JA, DeFeo D. (1987). Peroral extrusion of a ventriculoperitoneal shunt catheter. Neurosurgery. 21(2):259-261.
- Fermin S, Fernández-Guerra RA, Sureda PJ. (1996). Extrusion of peritoneal catheter through the mouth. Childs Nerv Syst. 12(9):553-555.
- Ghritlaharey RK. (2016). Review of the Management of Peroral Extrusion of Ventriculoperitoneal Shunt Catheter. J Clin Diagn Res. 10(11):PE01-PE06.
- Faheem M, Jaiswal M, Prajapati HP, Kumar R, Saba Nu, Ojha BK. (2022). Unusual complications of ventriculoperitoneal shunt surgery: Tertiary care experience. J Pediatr Neurosci 17(1):30-35.
- Alonso-Vanegas M, Alvarez JL, Delgado L, Mendizabal R, Jiménez JL, Sanchez-Cabrera JM. (1994). Gastric perforation due to ventriculo-peritoneal shunt. Pediatr Neurosurg. 21(3):192-194.
- Christoph CL, Poole CA, Kochan PS. (1995). Operative gastric perforation: a rare complication of ventriculoperitoneal shunt. Pediatr Radiol. 25(Suppl 1):S173-S174.
- Cohen-Addad DI, Hewitt K, Bell D. (2018). A ventriculoperitoneal shunt incidentally found in the stomach. Radiol Case Rep. 13(6):1159-1162.
- Alther E. (1965). [The gastric valve: a new surgical technic for the treatment of infantile hydrocephalus]. Schweiz Med Wochenschr. 95:234-236.
- Duff TA, Rosenthal J, Jane JA. (1977). Evaluation and revision of ventriculo-gastric shunts by gastroscopy. Neurochirurgia (Stuttg). 20(1):28-31.
- Jurkiewicz J. (2012). Ventriculogastric shunt. J Neurosurg Pediatr. 9(2):216-217.
- Odebode TO. (2007). Jejunal perforation and peroral extrusion of a peritoneal shunt catheter. Br J Neurosurg. 21(2):235-236.
- Lee CH, Tseng SH, Chen Y. (2015). Ileal perforation and transanal protrusion of the peritoneal tube in a boy with a ventriculoperitoneal shunt and literature review. Formos J Surg. 48:209-213.
- Grosfeld JL, Cooney DR, Smith J, Campbell RL. (1974). Intra-abdominal complications following ventriculoperitoneal shunt procedures. Pediatrics. 54(6):791-796.
- Sathyanarayana S, Wylen EL, Baskaya MK, Nanda A. (2000). Spontaneous bowel perforation after ventriculoperitoneal shunt surgery: case report and a review of 45 cases. Surg Neurol. 54(5):388-396.
- Tumialán LM, Lin F, Gupta SK. (2006). Spontaneous bacterial peritonitis causing Serratia marcescens and Proteus mirabilis ventriculoperitoneal shunt infection. Case report. J Neurosurg. 105(2):320-324.
- Bal RK, Singh P, Harjai MM. (1999). Intestinal volvulus--a rare complication of ventriculoperitoneal shunt. Pediatr Surg Int. 15(8):577-578.
- Tan LA, Kasliwal MK, Moftakhar R, Munoz LF. (2014). Ventriculoperitoneal shunt with a rare twist: small-bowel ischemia and necrosis secondary to knotting of peritoneal catheter. J Neurosurg Pediatr. 14(3):234-237.
- Peirce KR, Loeser JD. (1975). Perforation of the intestine by a Raimondi peritoneal catheter. Case report. J Neurosurg. 43(1):112-113.
- Sells CJ, Loeser JD. (1973). Peritonitis following perforation of the bowel: a rare complication of a ventriculoperitoneal shunt. J Pediatr. 83(5):823-824.
- Adeloye A. (1997). Protrusion of ventriculo peritoneal shunt through the anus: report of two cases. East Afr Med J. 74(5):337-339.
- Sharma BS, Kak VK. (1988). Multiple subdural abscesses following colonic perforation--a rare complication of a ventriculoperitoneal shunt. Pediatr Radiol. 18(5):407-408.
- Hsueh CC, Jaw TS, Lin JY, Chan HM. (2007). Splenic flexure colonic volvulus: a pediatric case report. Kaohsiung J Med Sci. 23(4):207-210.
- Martínez-Lage JF, Martos-Tello JM, Ros-de-San Pedro J, Almagro MJ. (2008). Severe constipation: an under-appreciated cause of VP shunt malfunction: a case-based update. Childs Nerv Syst. 24(4):431-435.
- Knuth J, Detzner M, Heiss MM, Weber F, Bulian DR. (2013). Laparoscopy for a ventriculoperitoneal shunt tube dislocated into the colon. JSLS. 17(4):675-678.
- Chen HS. (2000). Rectal penetration by a disconnected ventriculoperitoneal shunt tube: an unusual complication. Chang Gung Med J. 23(3):180-184.
- Gupta SK, Jaiswal AK, Kumar S. (2005). Ventriculoperitoneal shunt catheter masquerading as ascariasis. J Clin Neurosci. 12(8):966-967.
- Glatstein M, Constantini S, Scolnik D, Shimoni N, Roth J. (2011). Ventriculoperitoneal shunt catheter protrusion through the anus: case report of an uncommon complication and literature review. Childs Nerv Syst. 27(11):2011-2014.
- Marino M, Phillips C. (2019). Methicillin-Resistant Staphylococcus aureus Meningitis from Transanal Migration of a Ventriculoperitoneal Shunt. J Emerg Med. 57(3):e81-e84.
- Ghritlaharey RK, Budhwani KS, Shrivastava DK, Gupta G, Kushwaha AS, Chanchlani R, et al. (2007). Trans-anal protrusion of ventriculo-peritoneal shunt catheter with silent bowel perforation: report of ten cases in children. Pediatr Surg Int. 23(6):575-580.
- Vuyyuru S, Ravuri SR, Tandra VR, Panigrahi MK. (2009). Anal extrusion of a ventriculo peritoneal shunt tube: Endoscopic removal. J Pediatr Neurosci. 4(2):124-126.
- Lawther S, Patel R, Gabra H. (2013). Laparoscopic management of silent colonic perforation with trans-anal protrusion of ventriculo-peritoneal shunt catheter. J Pediatr Surg Case Rep. 1(5):106-107.