Information Links
Related Conferences
Previous Issues Volume 3, Issue 1 - 2021
Facilitators and Inhibitors of Independent Disease Self-Management for Adolescents with Type 1 Diabetes
Rita E. J. Meadows, Marylyn McEwen
*Corresponding author: Rita E. J. Meadows, 20930 Dupont Blvd, Suite 101, Georgetown, Delaware 19947. Tel: 302-519-8264; Office: 302-856-3737; Fax: 302-856-7337; Email: [email protected]
Received Date: December 01, 2021
Published Date: December 17, 2021
Copyrights: Meadows REJ. © (2021).
Citation: Meadows REJ. (2021). Facilitators and Inhibitors of Independent Disease Self-Management for Adolescents with Type 1 Diabetes. Mathews J Nurs. 3(1):5.
ABSTRACT
Purpose: To describe adolescents’ perceptions of facilitators and inhibitors of behaviors required to support independent self-management of type 1 diabetes (T1DM). Methods: A qualitative descriptive method was used to describe and analyze focus group data collected from 12 adolescents with T1DM who were participating in a summer camp. Focus group interviews were conducted and data were analyzed iteratively until thematic saturation was achieved. Results: The overarching theme, “Sorry, I have diabetes...It shaped me into who I am” was supported by three domains: Self-management behavior skills required during transition from dependent to independent T1DM self-management; Facilitators of everyday participation in self-management behaviors; and Inhibitors of everyday participation in self-management behaviors. Eight apriori and inductively generated categories support the three domains. Conclusions: Current transitional diabetes education programs for adolescents with T1DM must be refined. A more comprehensive assessment that identifies the multiple factors that impact independent self-management of adolescents with T1DM must address the social determinants of health, gender, race, culture, socioeconomic status, management of co-morbidities and the triadic relationship between parents, the school community, and the health care provider(s). Further research is needed to explore and identify the facilitators and inhibitors of transition from dependent to independent self-management of the adolescent with T1DM, from the adolescents’ perspective, to inform transitional interventions.
Keywords: Type 1 Diabetes, Adolescent, Transition, Independent Self-Management, Facilitators and Inhibitors
List of abbreviations: CGM- continuous glucose monitor, T1DM- Type 1 diabetes, PI- Principal Investigator
INTRODUCTION
Type 1 diabetes (T1DM) is one of the leading chronic diseases in childhood. Global estimates of type 1 DM among children and adolescents under age 20 now exceed 1 million [2]. Nationally, the Center for Disease Control National Diabetes Statistics Report, 2020, population data for the year 2018 estimated T1DM among children and adolescents under the age of 20 was 187,000 [3]. A significant increase in the number of children and adolescents with T1DM occurred between 2002 and 2015 [3]. Additionally, between 2010 and 2050 the number of children and adolescents with T1DM is projected to triple and reach a staggering 587,477 cases [1,3]. Adolescents with T1DM are at increased risk for poor outcomes during the transition between the dependency on parents for T1DM management to independent self-management [5-14]. Guidelines for transitioning adolescents to independent self-management recommend diabetes providers and educators begin transition preparation in early adolescence and at least one year before transfer to adult healthcare [5].
The consequences of a poor transition of the adolescent with T1DM to independent self-management may include poor glycemic control, permanent adverse microvascular and macrovascular health outcomes and strained interpersonal relationships with parents, peers, and healthcare providers [5-14]. Despite a robust literature set and current transitional guidelines to assess the ability of the adolescent with T1DM to access educational, healthcare and psychosocial resources, master blood glucose monitoring and management skills, become independent with medication administration, manage hypoglycemia, and understand the relationship between nutrition and glycemic control [1,5,11,15-17], adolescents with T1DM continue to be unsuccessful with transitioning from dependent to independent self-management. Further research is needed to explore and identify the facilitators and inhibitors of transition from dependent to independent self-management of the adolescent with T1DM, from the adolescents’ perspective, to inform transitional interventions. The purpose of this study was to 1) elicit adolescents’ perceptions of behaviors required for independent self-management, and 2) add to present knowledge of the facilitators and inhibitors of independent self-management of T1DM by adolescents.
METHODOLOGY
A qualitative descriptive methodology was used to explore adolescents’ understanding of required self-management behavior skills, and their perception of the facilitators and inhibitors and resources used in everyday T1DM independent self-management behaviors. Research approval was obtained through the University of Arizona Human Subjects Protection Program. The study was conducted during a week-long summer residential camp leadership program for adolescents ages 15-17 years old diagnosed with T1DM, located in the northeastern United States. A purposeful sample provided rich data. Data saturation was achieved with 12 adolescent participants.
A recruitment flyer that included the purpose of the research study, what was being asked of participants, and the study timeline was mailed 1 month in advance of camp to the residences of each camper and their guardian. One week after the flyer was mailed, another email from the camp director regarding coordination of camper arrivals included the assent/parental permission form and the camp sign-in schedule if the camper chose to participate in the study. The principal investigator (PI) tailored the informed consent and risks and benefits appropriate for adolescent development and literacy level. Participants and their guardians were provided a copy of the consent form which included the right of participants to voluntarily withdraw from the study at any time, the central purpose of study, procedures used for data collection, the protection of confidentiality of participants, the known risks associated with participation, and the potential benefits to the participants. Parental consent and participant assent were obtained by the PI during camp check-in.
Two focus group interviews, one for male and one for female campers, were conducted in a private room appropriate for audio recording. The PI reminded participants of their right to withdraw from the study at any time without any impact on their ability to participate in camp activities at the start of each focus group. Audio recorded focus groups were conducted before camp orientation to minimize disruption of camp activities. Unfamiliar and ambiguous terminology such as the definition of facilitators, inhibitors, and independent self-management were defined and the pragmatic meanings of questions for the participants were clarified as needed. Responses to the research questions with no new data occurred after 45 minutes with the male participants and at 65 minutes with the female participants.
Figure 1: Taxonomy of data analysis
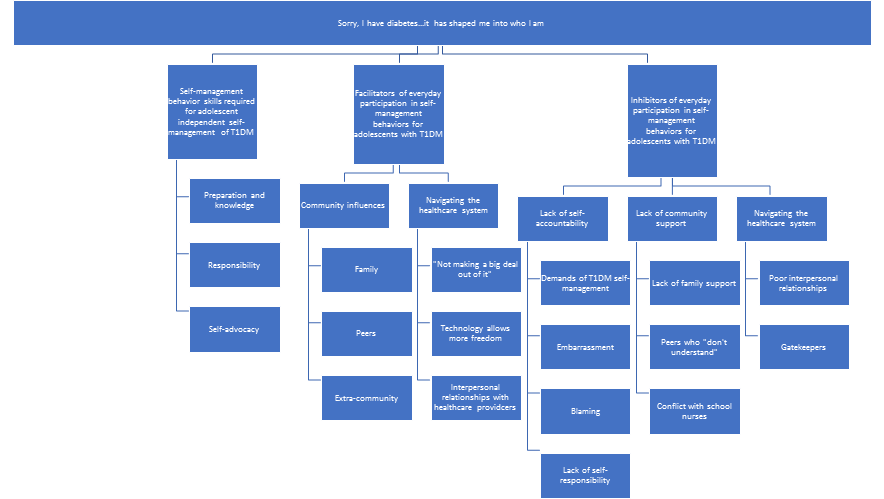
The PI recognized adolescents with T1DM as a population with unique and high-risk needs such as a possible need for healthcare intervention for blood glucose excursions during the interview process, or the adolescents’ potential divulgence of information related to co-morbid conditions often associated with T1DM. Continual assessment for these types of issues was conducted by the PI during the interviews. Participants were reminded to maintain the confidentiality of other participants outside of the focus group. Also, as a health care provider for the campers, the PI remained astute to a perceived potential power differential between herself and the adolescents. Data from the focus group audio recordings and transcriptions, handwritten field notes, and memos were uploaded, stored, and managed in Atlas.ti computer-assisted qualitative data analysis software on the PI’s encrypted, password-protected computer [18]. Qualitative content analysis was used to develop a taxonomy that represents the a priori or deductive and the inductive data analyses (Figure 1). Participant statements and/or words were used to construct the overarching theme, domains, and categories elicited the adolescents’ perceptions of behaviors required for independent self-management of T1DM, and provided new insights into facilitators and inhibitors of independent self-management of T1DM.
RESULTS
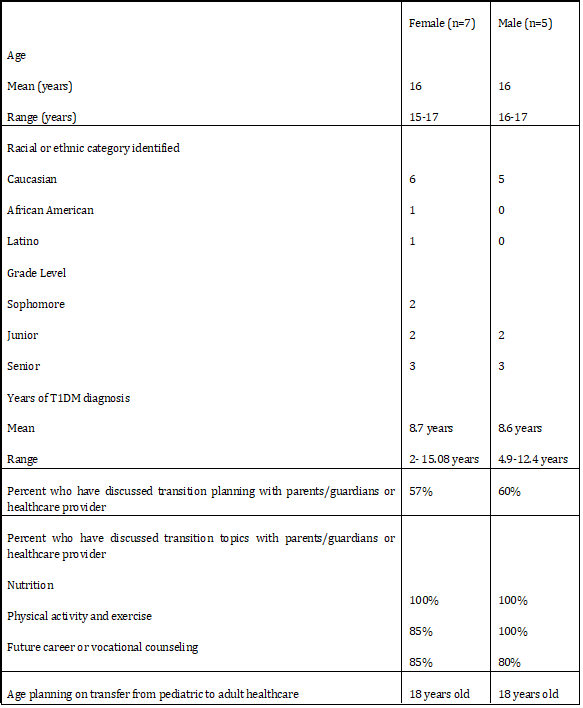
Twelve adolescents diagnosed with T1DM for at least one year participated in the study. Demographic data were collected on all participants (See table 1). Seven were female (six Caucasian and one African American/Latina) ages 15-17 years and five were Caucasian males ranging from 16-17 years of age. All except one female participant and one male participant reported previously receiving formal T1DM education in nutrition, physical activity and/or transition from pediatric to adult healthcare. All participants reported they expected to transition from pediatric to adult healthcare at 18 years of age.
Table 1: Participant demographic data
Self-management behavior skills required during transition from dependent to independent T1DM self-management
Through an iterative process, the data from two focus groups in response to semi-structured interview questions were analyzed using deductive coding for a priori categories generated by the research questions. Inductive coding was also used to identify themes and describe the adolescents’ perception of independent T1DM self-management. The data were best represented by an overarching theme, “Sorry, I have diabetes….it [T1DM and T1DM self-management] has shaped me into who I am.” (see Figure 1). Most female and male participants expressed a general acceptance of T1DM and the management requirements as part of who they were or “something you just sort of do.” Female participants expressed indifference to the painful aspects of disease management, such as needle sticks. One female participant added, “Some days, I wouldn't trade it [having T1DM] for the world because it [T1DM] shaped me into who I am.” Three domains that supported the overarching theme emerged from the data: 1) Self-management behavior skills required during transition from dependent to independent T1DM self-management; 2) Facilitators of everyday participation in T1DM self-management behaviors; and 3) Inhibitors of everyday participation in T1DM self-management behaviors.
Preparation and knowledge of T1DM informed the adolescents’ self-management behavior skills required for successful transition from dependent to independent self-management. Participants’ understanding of the etiology and management of T1DM and willingness to adapt and change based on their disease process was shared by both female and male participants. A female stated, “My basal might be one unit during the day, but at night it has to go up, because my blood sugar is going up. And, so, just noticing those sorts of trends and being able and willing to sort of adapt to those really makes a difference.” A male stated that “knowing your body” correlated with being able to correct glycemic excursions. Personal knowledge of the effects of physical activity on glycemic control enabled participants to understand and challenge disease-specific information received from their health providers and community. One female participant stated that a peer told her “That doctors don't want type 1 diabetics exercising. And I don't agree with that”. Female participants also identified the importance of self-managing co-morbid conditions such as depression, Celiac disease and sleep apnea in addition to their T1DM self-management needs.
Participants discussed their willingness to take on behaviors of independent self-management, including changing insulin pump sites, medication management, setting alarm clocks for insulin reminders, preparing a backpack with needed supplies when leaving the house, and maintaining a routine. One male participant stated, “I’ll have a bag that will always have glucose tabs in it and then whenever I’m leaving, I’ll pick up that bag and throw my pump and my test kit in there. And, so, when I’m leaving, I know I have that stuff with me”. Participants revealed safety nets they had developed within their communities through self-advocacy, and they targeted specific individuals within their social networks. One female stated that her teacher facilitated T1DM education of her peers in class, “And it was really fascinating how… the questions just started piling up and they wanted to learn more, and it was really fun.” A male participant stated, “I don’t need to teach ten friends how to do this, when I can just teach the coach who will always be there”.
Facilitators of Everyday Participation in Self-Management Behaviors
Facilitators of everyday self-management behaviors included support from parents and peers, school resources, navigating the healthcare system and health care provider knowledge and skills. Overall, with parental encouragement, respect, and trust, participants felt empowered to safely and independently self-manage their T1DM. Many participants were comforted by a parental resource. One male participant stated, “During the day, I’m pretty much on my own with that, not because they won’t help, but just because I can do it myself unless I’ve done something horribly wrong with some sort of calculation...” Female participants agreed that their support networks would benefit from caregiver support resources with one stating, “I think there needs to be something [support resources] that are more accessible to parents and relatives”.
Peers were identified as another facilitator of T1DM self-management. The amount of support provided by peers without T1DM depended upon the motivation of those peers to help them, their level of understanding of the urgent and emergent signs and symptoms of T1DM complications, and the desire of the adolescents with T1DM to engage peers without T1DM in their independent self-management. A female participant who received support from peers without T1DM stated, “I know if I fall over in the middle of a restaurant or something they'll have an idea of what to do. They might not know if I'm low or high, but they know where my pump is on me. They know how to check it on my phone.” Social networking among peers with T1DM is an additional facilitator. During the interview, one female participant aided another who requested guidance in troubleshooting insulin pump settings, and offered further assistance, “If you want help later in the cabin or something”. At the end of the interview, the female participants excitedly planned to continue discussions of independent self-management in their cabin following the interview.
Male and female participants had different experiences with school resources. All the male participants viewed school nurses as positive resources in case of an emergent or urgent situation, with one male stating, “The school nurse knows and if it gets to the point where you need something badly, they will call in the nurse”. Two female participants took active roles in their health classes, educating other students on T1DM etiology and management. Some of both the male and female participants stated they appreciated the receipt of additional accommodations through individualized, disease-specific academic plans (“504 plans”) on how the school system could remove barriers to academic success for students with disabilities.
Learning how to smoothly navigate the healthcare system by “not making a big deal out of it” was identified as a facilitator of T1DM self-management. One female participant highlighted the importance of learning the skills of ordering insulin pump supplies and equated it to learning telephone communication skills, “Like my mom knows I can't even call to order a pizza half of the time. I can now.” One male participant expected obtaining their own health insurance policy before leaving the family home to be a simple process “just sort of move it from my parents’ account to mine.” Access to technology, such as a continuous glucometer (CGM) with alarms and insulin pumps facilitated independent self-management and assisted their parents in monitoring their blood glucose levels during the night. One male stated, “I can be a lot lazier with what I do [blood glucose monitoring], knowing that I have my blood sugar tested every five minutes [CGM]. So, it allows me to have a lot more freedom with what I want to do.”
Most participants agreed their health care providers facilitated their fundamental learning of independent self-management skills. One male correlated his maturity with learning independent self-management stating, “Just as you mature and get older and understand more the kind of impact that it [T1DM] has”. Another male participant explained that the bulk of his knowledge formation began with diabetes education, and then they “practice behaviors of independent self-management between [health care] visits.” Healthcare provider knowledge and skill were important facilitators of independent self-management, especially with helping them change insulin settings based on health changes, with males citing teaching “glycemic index”, "noticing trends", and "keeping it [blood glucose] steady." Participants appreciated providers that communicated directly with them versus their parents and expressed confidence in their abilities to troubleshoot T1DM self-management.
Inhibitors of Everyday Participation in T1DM Self-Management Behaviors
Inhibitors of T1DM self-management behaviors included the daily demand of self-management, prioritization of T1DM self-management over other daily activities such as sleep, blaming diabetes as an excuse to not assume responsibility, parental behaviors, lack of family support, peer pressure, poor interpersonal skills with school nurse and health care providers, and barriers to engaging in independent behaviors such as ordering supplies. Independent T1DM self-management was described by females as “hard”, “agitating,” and “can frustrate you”. The female participants sometimes became exasperated by T1DM self-management, as one stated, “You just need a week off of diabetes”.
Prioritizing other activities over glycemic control inhibited independent self-management of T1DM. Female participants agreed that discomfort with or embarrassment by publicly performing the skills of self-management interferes with independent self-management, “If you're in a dress, you don't want to raise your dress and grab your pump or raise it and take a shot.” Many of the female participants agreed that during the summer months they failed to maintain the same schedule they had during the school year and did not prioritize self-management behaviors. Female participants stated that the summer change of schedule impacted their “sleep schedule”, “eating [habits]”, and the frequency of blood glucose monitoring. Some of the female participants admitted to using T1DM as a scapegoat that inhibited engagement in independent self-management behaviors. “It'll [a negative event] have nothing to do with it [effects of T1DM] and I'll be like, ’Sorry, I have diabetes”. Another female participant scoffed, stating, “It's kind of like instinct where I just blame it, and then they're [the community] like, ‘Okay’." A diagnosis of diabetes gave them “an excuse” to absolve them of responsibilities, “I have the right. I'm diabetic.”
Female participants identified familial inhibitors of independent self-management as overbearing or accusatory parental behaviors. One female described her parents as "down your throat all the time". Another female stated that her parent will “throw it [poor self-management behaviors] in your face” and another added that parental pressure, “just makes you feel worse about yourself. You just don't want to [self-manage T1DM].” One female stated that “Some things that your parents say actually hurt”, which results in decreased self-esteem, decreased self-confidence and giving up, “then I just don't want to do it at all.” Females cited decreased parental involvement in T1DM self-management over time, fear of parental anger, parental fear of T1DM diagnosis, parental distrust, and punishment for not engaging in independent self-management behaviors, and lack of psychosocial support as inhibitors of independent self-management. One female stated, “One day you just have like one high [blood glucose level] or and [her parent] like, ‘Oh, I'm taking every privilege [of independent self-management] you had.’" Another female stated, “It [family involvement] is different from everybody's home lives. It's just me and my dad and my sister… she's eight with Down's syndrome, so a lot of attention goes to her. I've learned how to do everything on my own.” One female stated “She'll [her mother] be like, ‘I'm not trusting you; you're not doing this without me watching you. I have to give you your shots. I can't trust you for anything,’ when you feel like you're starting to get a rhythm”. Some female participants perceived their mothers as interfering with their ability to self-advocate, independently problem solve, and build and maintain support networks-particularly relationships with their healthcare providers and school nurses. One female stated, “But then if a school nurse is trying to tell you what to do [manage blood glucose], then they're [her mother is] like, ‘You can't tell her [school nurse]’.” Female participants also regarded not being “blessed” with financial resources as an inhibitor of independent T1DM self-management.
Female participants noted discomfort with instances when they could not relate to peers with T1DM. According to a female participant, peers with T1DM who “haven't reached all the stages in your life [who] look down on you”, inhibited independent self-management behaviors by making them feel incompetent. Female participants resented being thrust into adult-led “diabetes support groups” composed of other adolescents with T1DM with whom they were not familiar.
Males and females highlighted insensitivity by peers and employers without T1DM as inhibitors of independent self-management. A female participant described it as a form of “peer pressure” and clarified, “I can't [go out with friends because] my blood sugar's high and I don't feel good. And they're like, ‘Just come anyway’.” A male stated, “We’ll go out to eat ice cream and they’ll just order this big ol’ Sundae, you know, without care. I got to bolus, like, 15 minutes before we eat, before we even get there.” One female participant stated, “jobs where you're like, I need to sit down and take a break, and they’re like, No!”
Female participants, not male, experienced the school nurse as inhibiting their T1DM self-management. Several of the female participants described school nurses failing to consider their individual nuances for independent T1DM self-management. These participants found ways to circumvent the nurses’ diabetes management rules. “It's like, call my mom on the phone and you can talk to her. I'm going back to class because you're making me miss two periods for nothing.”
Navigating the healthcare system was identified as an inhibitor, largely due to poor interpersonal relationships with healthcare providers and difficulty accessing the healthcare system due to their age. Some female participants complained that their providers focused on their parents during visits which resulted in feeling that they were not being listened to and being unfairly judged by their provider. One participant withdraws from her endocrinologist during visits and, “pout. I sit there and just don't talk.”
Several female participants identified ordering supplies from durable medical supply companies as an inhibitor. "You call them, they tell you they won't talk to you because you're a minor when you're the patient just trying to order yourself something …” Although most participants were not immediately concerned with their personal access to medications, insurance, or food, many participants shared stories of and concerns for individuals with T1DM that had difficulties obtaining insulin and health insurance and maintaining access to proper nutrition. One female noted, "Your blood sugar shouldn’t be dependent upon your access to food."
DISCUSSION
This study, based on the perspective of the adolescent with T1DM, extends the paucity of extant literature related to transitioning from dependent to independent self-management, informs our understanding of their transition facilitators and barriers, and provides targets for educational and supportive programs that facilitate independent T1DM self-management. Current research is insufficient in identifying the relationships and interdependence between the adolescent, parent, and providers [5], the reasons adolescents with T1DM are unable to stay on track with the responsibilities of self-management [11], and the support needs of adolescents with T1DM within their communities. Current literature is predominantly from the perspective of the parent or healthcare providers [6,11,20,21,22]. This study is one of few to describe from the adolescents’ perspective, the behaviors required to achieve independent T1DM self-management and the factors that facilitate and/or inhibit this process.
Current literature identifies differences in parental and adolescent perceptions of transition success, and parental difficulties in the gradual shift in roles from primary caregiver to supportive resource network [17,21,22,24]. In support of current research, this study found the adolescents’ perspective of successful role transition was dependent upon mutual trust, as well as the adolescent’s comfort in using parents as safety nets. However, male participants in this study were found more likely to accept and receive family support to troubleshoot with independent self-management behaviors while female participants resisted parental involvement and assistance as they got older.
One study described maintaining a routine to integrate independent self-management behaviors into everyday life as “Normalizing”, while another study referred to increased experience with disease management as learning to “live normally” [11,21,24]. In this study, “normalizing” was demonstrated through participant behaviors such as maintaining a routine, changing insulin pump sites on time, setting alarm clocks to remember to take insulin, and preparing and carrying their backpack with needed supplies. However, some female participants had difficulty integrating behaviors of independent self-management into their personal value systems due to lack of self-accountability, lack of personal responsibility for the demands of T1DM management, embarrassment over the diagnosis of T1DM, or finding blame for poor health outcomes beyond themselves.
This study supported current knowledge of adolescents’ use of peers as resources to facilitate independent self-management of T1DM [6,9,11,21,24,25]. This study also found that the quality of support from peers without T1DM that facilitated independent self-management was dependent on peer understanding of the demands of T1DM in the adolescents’ lives, and signs and symptoms of hypo- and hyperglycemia, as well as peers’ willingness to help the participant achieve success in independent self-management. Peers without T1DM pressured some participants to disregard T1DM self-management behaviors because it interfered with their social activities. In female participants, this led to feelings of guilt and embarrassment, while male participants felt isolated. Current literature shows that a commiserate understanding of the demands of T1DM underlies the value of support from peers with T1DM [21,23]. However, female participants in this study clarified that the desire to engage peers with T1DM in a support group environment was also dependent on their similarities in developmental level and their ability to develop a bond of friendship.
In support of current literature, this study identified overbearing parents and family members as inhibitors of independent T1DM self-management [5,9,11,21,22], but overall, female participants were found to have more turbulent relationships with their parents and family members than male participants. Current literature also stresses the importance of the school nurse to establish an equal partnership with the adolescent during the transition process of the adolescent with T1DM to independent self-management [11,14,24]. In this study female participants often found themselves in the middle of a tug of war between their parents and school nurses, which resulted in decreased adolescent confidence in independent self-management tasks.
Current literature shows positive perceptions of healthcare, increased responsibility for healthcare needs, communication about the healthcare transition, and higher levels of health literacy are associated with a successful transition to independent self-management [7]. In this study, adolescents found healthcare provider access limited by provider turnovers and shortages, and for one female participant, telemedicine which reduced focus on provider-adolescent communication. This study also found that insurance companies, pharmacies and durable medical supply companies would limit communication with female participants due to their ages, thereby inhibiting independent self-management.
CONCLUSION
Based on the study findings, the authors recommend refining current transitional diabetes education programs for adolescents with T1DM. Specifically, the recommendation is to incorporate a more comprehensive assessment to identify the far-reaching impact on independent self-management of adolescents with T1DM that includes: the social determinants of health, gender, race, culture, socioeconomic status, management of co-morbidities and the triadic relationship between parents and the school nurse.
Longitudinal studies are needed to evaluate the long-term effectiveness of transitional programs that incorporate the facilitators and inhibitors of independent self-management found in this study [5,9,19]. Further research is needed to develop and evaluate diabetes education programs for adolescents with T1DM that 1) increase accessibility to and facilitate bonding between peers with T1DM in alternative settings, such as in the camp setting 2) compare the impact of different environments through which the adolescent can self-advocate and educate their community on T1DM, and 3) incorporate the use of technology in the community and healthcare system in which the adolescent interacts.
REFERENCES
- Chapter 12. Children and Adolescents: Standards of Medical Care in Diabetes—2018. Diabetes Care. 2017; 41(Supplement 1).
- Lin X, Xu Y, Pan X, Xu J, Ding Y, (2020). Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 10:14790. Available from https://www.nature.com/articles/s41598-020-71908-9
- Centers for Disease Control and Prevention. National Diabetes Statistics Report 2020: Estimates of Diabetes and Its Burden in the United States. Available from https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed July 8, 2020
- Dabelea D, Mayer-Davis EJ, Saydah S, Imperatore G, Linder B, et al. (2014). Prevalence of Type 1 and Type 2 Diabetes Among Children and Adolescents From 2001 to 2009. JAMA. 311(17):1778–1786.
- Castensøe-Seidenfaden P, Teilmann G, Kensing F, Hommel E, Olsen BS, et al. (2017). Isolated thoughts and feelings and unsolved concerns: adolescents’ and parents’ perspectives on living with type 1 diabetes - a qualitative study using visual storytelling. J Clin Nurs. 26(19-20):3018-3030. Available from https://onlinelibrary.wiley.com/doi/10.1111/jocn.13649
- Bomba F, Herrmann-Garitz C, Schmidt J, Schmidt S, Thyen U. (2016). An assessment of the experiences and needs of adolescents with chronic conditions in transitional care: a qualitative study to develop a patient education programme. Health Soc Care Community. 25(2):652-666.
- Beal SJ, Riddle IK, Kichler JC, Duncan A, Houchen A, et al. (2016). The Associations of Chronic Condition Type and Individual Characteristics With Transition Readiness. Academic Pediatrics. 16(7):660-667.
- Campbell F, Aldiss S, Biggs K. (2016). Transition of Care for Adolescents from Child to Adult Health Services. Cochrane Database Syst Rev. 2016:147-169.
- Ersig AL, Tsalikian E, Coffey J, Williams JK. (2016). Stressors in Teens with Type 1 Diabetes and Their Parents: Immediate and Long-Term Implications for Transition to Self-Management. J Pediatr Nurs. 31(4):390-396.
- Hagger V, Hendrieckx C, Sturt J, Skinner TC, Speight J. (2016). Diabetes Distress Among Adolescents with Type 1 Diabetes: a Systematic Review. Curr Diab Rep. 16(1):9.
- Babler E, Strickland CJ. (2015). Moving the Journey Towards Independence: Adolescents Transitioning to Successful Diabetes Self-Management. J Pediatr Nurs. 30(5):648-660.
- Chu PY, Maslow GR, Isenburg MV, Chung R J. (2015). Systematic Review of the Impact of Transition Interventions for Adolescents With Chronic Illness on Transfer From Pediatric to Adult Healthcare. J Pediatr Nurs. 30(5):e19-27.
- Egan EA, Corrigan J, Shurpin K. (2015). Building the Bridge From Pediatric to Adult Diabetes Care. Diabetes Educ. 41(4):432-443.
- White M, O'Connell MA, Cameron FJ. (2015). Transition to adult endocrine services: What is achievable? The diabetes perspective. Best Pract Res Clin Endocrinol Metab. 29(3):497-504.
- Radovick S, Misra M. (2018). Pediatric Endocrinology a Practical Clinical Guide. Cham: Springer.
- Little JM, Odiaga JA, Minutti CZ. (2017). Implementation of a Diabetes Transition of Care Program. J Pediatr Health Care. 31(2):215-221.
- Sheehan AM, While AE, Coyne I. (2015). The experiences and impact of transition from child to adult healthcare services for young people with Type 1 diabetes: a systematic review. Diabet Med. 32(4):440-458.
- ATLAS.ti Qualitative Data Analysis. What is ATLAS.ti. 2000-2020. Available from https://atlasti.com/product/ Accessed August 3, 2020.
- Farrell K, Fernandez R, Salamonson Y, Griffiths R, Holmes-Walker D. (2018). Health outcomes for youth with type 1 diabetes at 18 months and 30 months post transition from pediatric to adult care. Diabetes Res Clin Pract. 139:163-169.
- Hansen K, Jensen AL. (2017). Partnership in transition: Experiences of adolescents with type 1 diabetes. Int Diabetes Nurs. 14(2-3):52-29.
- Babler E, Strickland CJ. (2016). Helping Adolescents with Type 1 Diabetes "Figure It Out." J Pediatr Nurs. 31(2):123-131
- Polfuss M, Babler E, Bush L, Sawi K. (2015). Family perspectives of components of a diabetes transition program. J Pediatr Nurs. 30:748-756.
- Fernandes S, O'Sullivan-Oliveira J, Landzberg M, Khairy P, Melvin P, et al. (2014). Transition and transfer of adolescents and young adults with pediatric-onset chronic disease: The patient and parent perspective. J Pediatr Rehab Med. 7(1):43-51.
- Borges B, Neto J, Falcão L, da Silva A, de Freitas R. (2016). Type 1 Diabetes Mellitus in adolescents: From diagnosis to the daily contact with the illness. J Nurs. 10(7):2328-2335.
- Joly E. (2015). Transition to adulthood for young people with medical complexity: An integrative literature review. J Pediatr Nurs. 30(5):e91-103.