Information Links
Related Conferences
Previous Issues Volume 6, Issue 3 - 2023
Epidermoid Cyst of Suprasternal Region in an Adolescent: A Rare Case Report
Pankaj Goyal1,*, Kishan Kumawat2 GN Gupta3 Nidhi P Chanchlani4
1Consultant E.N.T. and Head & Neck surgeon, Apollo E.N.T. Hospital, Jodhpur, Rajasthan, India
2Apollo ENT Hospital, Jodhpur, Rajasthan, India
3,4Reliable diagnostic centre, Jaipur, Rajasthan, India
*Corresponding author: Pankaj Goyal, Consultant E.N.T. and Head & Neck surgeon, Apollo E.N.T. Hospital, Jodhpur, Rajasthan, India, ORCID: 0000-0003-4098-7308; E-mail: [email protected].
Received Date: July 11, 2023
Published Date: July 25, 2023
Citation: Goyal P, et al. (2023). Epidermoid Cyst of Suprasternal Region in an Adolescent: A Rare Case Report. Mathews J Surg. 6(3):20.
Copyrights: Goyal P, et al. © (2023).
ABSTRACT
Neck cysts are made up of a range of pathologic entities. Epidermoid cysts are benign tumours with cystic cavities bordered by simple squamous epithelium. Adolescent epidermoid cyst in the suprasternal area is an exceptionally uncommon condition. The age of the presentation and the clinical examination help to narrow the differential diagnosis, but imaging is necessary for a precise diagnosis and for pre-treatment planning. For preliminary analysis, ultrasound is frequently employed. The extent and internal composition of the mass can be better understood with the help of computed tomography (CT) scan. A supporting role for diagnosis confirmation is played by fine-needle aspiration cytology (FNAC). The best modality treatment for this kind of lesion is surgical excision.
Keywords: Epidermoid Cyst, Suprasternal Region, Ultrasonography, Computed Tomography Scan, FNAC, Surgical Excision.
INTRODUCTION
Dermoid cysts are benign entities, characterized histologically as if it is lined by squamous epithelium, it is known as epidermoid cyst, if it contains skin adnexa, it is called true dermoid and if it contains tissue of all three germ layers like muscle, teeth, bone, cartilage it is called teratoid cyst [1]. In the head and neck and oral cavity, the prevalence rates are 7% and 1.6%, respectively [2]. According to the literature, the word dermoid cyst can be used interchangeably for any of three histologically distinct entities. They appear where embryonic fusion occurs. The first published incidence of an epidermoid cyst was in Turkey [2] in 2008, and six more cases have subsequently been reported in India, making the suprasternal area a rare site of presentation [1]. We report a case of an epidermoid cyst in the suprasternal region, presented as a midline mass at neck region in an adolescent female patient. She was treated with surgical excision of neck cyst. Because epidermoid cysts are less frequent in the head-neck region, they are more likely to be misdiagnosed. The majority of diagnoses are made by imaging inform of ultrasonography and computed tomography scan, with the use of fine needle aspiration, and are then confirmed by excision biopsy. However, there are frequently situations of diagnostic difficulty, which complicate the clinical picture and therapeutic protocol due to the various forms of clinically related and identical lesions that develop in the head and neck region.
CASE REPORT
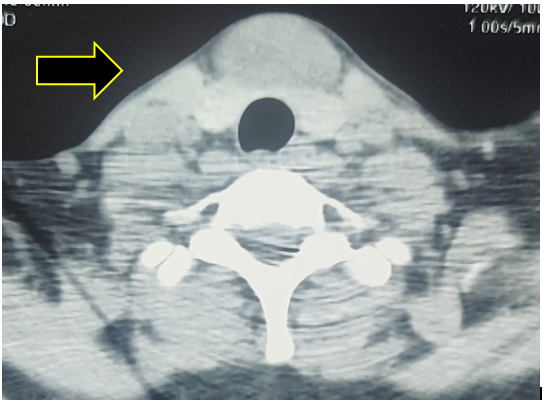
A twenty-one-year-old female patient presented to our Apollo ENT Hospital in Jodhpur, Rajasthan, with midline neck swelling from childhood. The swelling increases gradually. She denied any previous history of respiratory problems, voice changes, or swallowing difficulties. There were no signs of hyper- or hypothyroidism. Her menstrual cycle was regular. There was no history of trauma at the neck. During the clinical examination, the neck's suprasternal area showed a 3.5 x 3 cm swelling. (Figure 1) The swelling was soft and cystic. It was not tender. Over the swelling, there was no erythema, scars, or dilated veins. No movement of the neck mass could be produced by swallowing or protrusion of the tongue. There was no further neck swelling or lymphadenopathy found. The systemic assessment was uneventful. Routine laboratory tests, including a complete blood count, liver function, and renal function, all came back normal. On computed tomography (CT) scan, there was 3.2 x 2.5cm x2.0cm well defined soft tissue lesion noted just below thyroid isthmus, not involving any great vessel in the neck and it was not involving the retrosternal region. It was very well defined and had fluid contents displaying wall enhancement on contrast imaging (Figure 2A & 2B). The lesion did not include any major vessels in the neck or the retrosternal area. The patient was advised to undergo fine needle aspiration cytology (FNAC), which revealed an epidermoid cyst. After obtaining the patient's informed agreement, she was scheduled for surgical excision under general anaesthesia. A transverse incision was made 2 cm above the suprasternal notch and dissected around the mass capsule (Figure 3). Hyperextension of the neck and upward retraction of the mass were used to get access to the lower margin. It was excised completely with intact cyst wall (Figure 4). The surgical wound was closed in layers. The patient was moved to recovery after a successful extubation. Histopathological analysis revealed a cyst in the dermis that was surrounded by stratified squamous epithelium and keratinization. The cyst wall was devoid of any adnexal features, such as hair follicles or eccrine glands. Granular cell layer is present in the epithelium. Lamellar eosinophilic flakes make up the keratin. There were no cells found. This look resembled an epidermoid cyst (Figure 5A & 5B). During six month follow up, patient was doing well without any recurrence.

Figure 1. Clinical picture of midline neck cyst at suprasternal region.
A
B
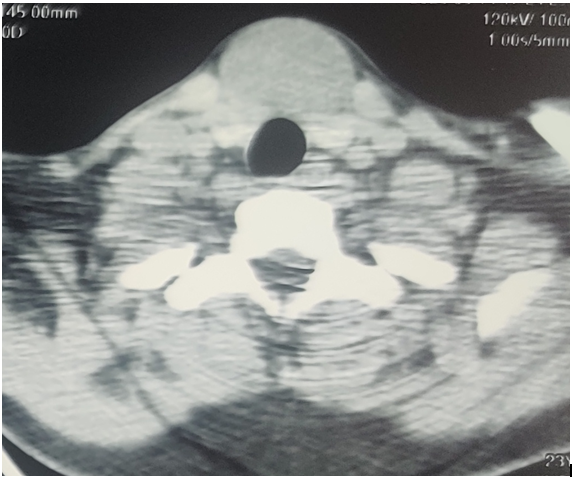
Figure 2 (A & B). CT scan of the neck revealed a cystic mass in the suprasternal area and measured 32 mm x 25 mm x 20 mm. It was very well defined and had fluid contents displaying wall enhancement on contrast imaging.

A
B
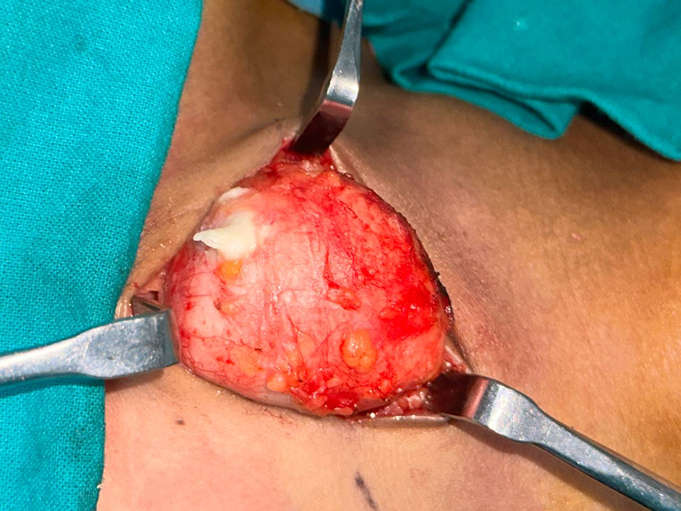
Figure 3 (A & B). Intra operative view of the cyst and surgical dissection around it.

Figure 4. Main specimen–Intact epidermoid cyst after complete excision
A
B
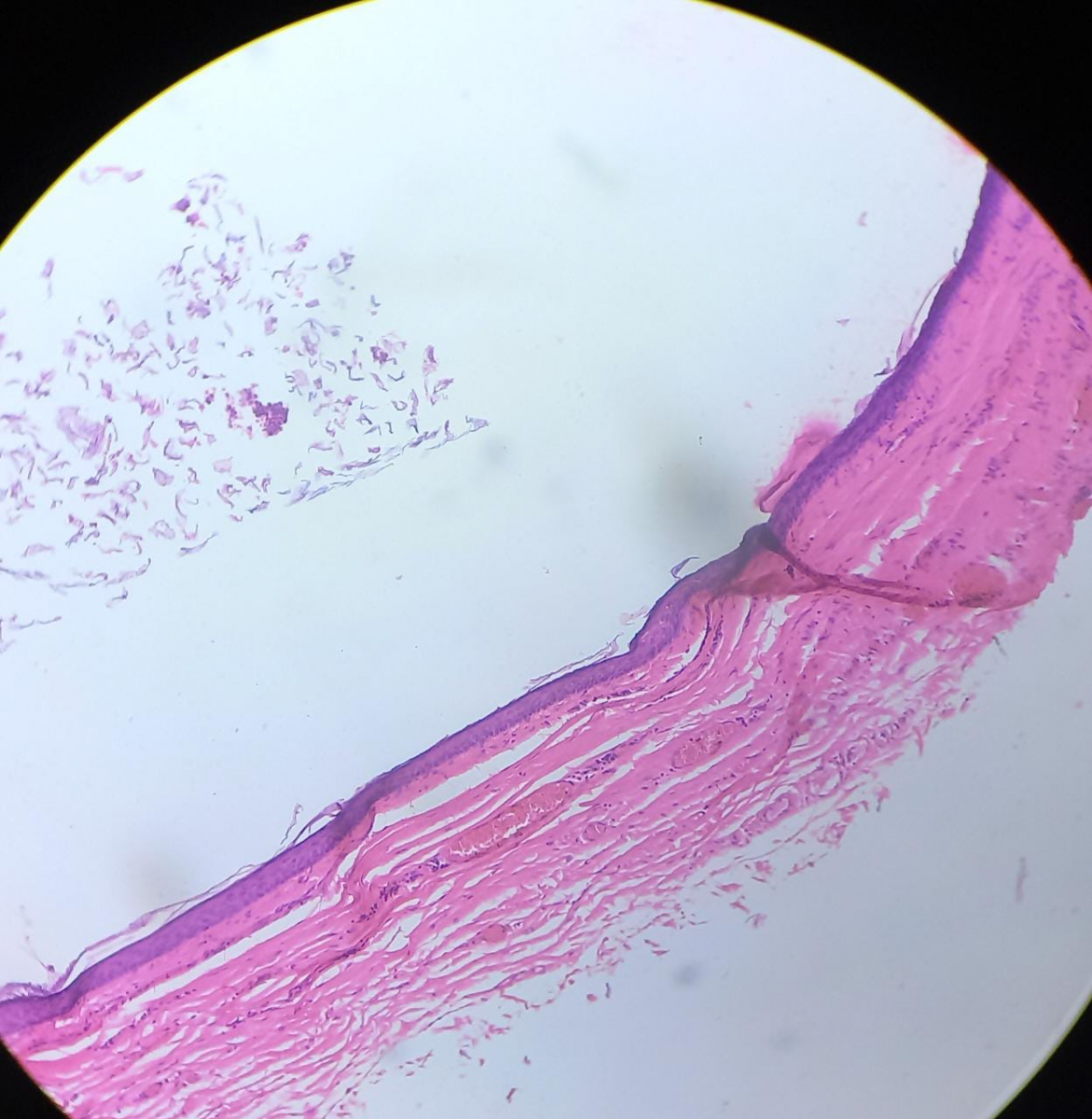
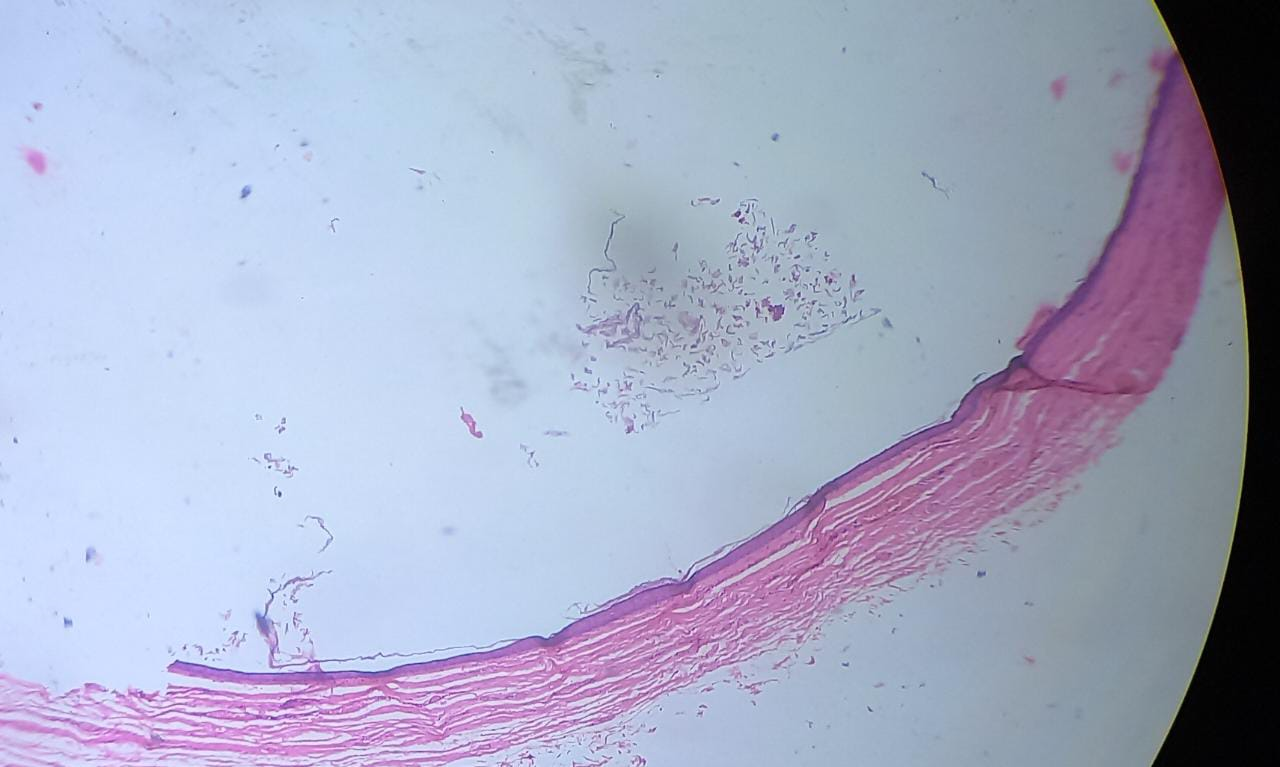
Figure 5A. Microscopic view of the epidermoid cyst. Cyst wall lined by keratinizing stratified squamous epithelium and contains keratin flakes (Hematoxylin and Eosin stain, magnification 100×); (B) microscopic view of the epidermoid cyst. Cyst wall lined by keratinizing stratified squamous epithelium (Hematoxylin and Eosin stain, magnification 400×).
DISCUSSION
In the Otorhinolaryngology Clinic, cystic masses in the head and neck region are frequently seen, and epidermoid cysts in the form of cutaneous lesions are thought to most frequently affect the face, scalp, neck, and trunk. [3]. However, dermoid and epidermoid cysts in the head and neck are less common in the deeper tissue planes, contributing roughly 1.6–6.9% of all instances in the body, as substantiated by a thorough examination of both new and older literature [4]. The head and neck region accounts for just 7% of all epidermoid and dermoid cysts [5,6], 1.6% in the oral cavity, and constitutes only 0.01% of all the oral cysts [6-8].
In children, a neck tumour or cyst is fairly prevalent. However, suprasternal epidermoid cysts are quite uncommon. Epidermoid cysts appear early in life, with the majority of lesions appearing during infancy. In our case, it appears during adolescence, which is an extremely rare occurrence.
Despite having a similar presentation or histology, epidermoid and dermoid cysts can be congenital or acquired [9]. Congenital cysts are dysembryonic lesions that develop from entrapped ectoderm during the fusion of the first and second branchial arches [9]. Acquired cysts caused by traumatic or iatrogenic epithelial cell inclusion or blockage of a sebaceous gland duct.
Dermoid cysts of the head and neck are assumed to be congenital inclusion cysts [9].
The majority of subcutaneous epidermoid cysts are relatively tiny and can often be identified clinically without imaging. Rarely do they enlarge to the point where more investigations are necessary. It is possible for large or medium epidermoid cysts to develop in unexpected locations adjacent to certain organs, simulating tumours coming from that tissue as in our instance [10].
Epidermoid cysts have a gradual, steady growth pattern and do not cause symptoms unless they get bigger. The cyst's rapid growth may be an indicator of an underlying infection or malignancy [11]. Although uncommon, epidermoid cysts and squamous cell cancer have been linked in ten cases [12].
Bowen's disease, Paget's disease, and squamous cell carcinoma have all been isolated cases of premalignant and malignant disorders that were detected in the walls of epidermoid cysts, despite the fact that these conditions are rare in this type of cyst [2]. The clinical diagnosis must be supported by imaging in order to determine the lesion's anatomical extent and to guide any necessary treatment.
High-resolution ultrasound (US) is the best initial imaging test for neck masses because it typically detects the cystic character of the mass and locates it in relation to the surrounding structures. Its diagnostic value has greatly improved as a result of advancements in three-dimensional technology, colour, and power Doppler applications. The advantages of computed tomography (CT) include its ability to validate the results of ultrasound (US), assess the size of the lesion, and demonstrate calcification or fat within the lesion. These are typically seen as well-defined anechoic masses with posterior enhancement in the midline of the neck on a CT scan [13].
The diagnosis of cystic neck masses also involves magnetic resonance imaging (MRI). T2 weighted MRI is especially useful for separating cystic from solid components. In some circumstances, fine-needle aspiration cytology (FNAC) may be necessary to confirm the diagnosis. The differential diagnosis of a midline anterior neck mass includes thyroglossal duct cyst, dermoid cyst, cystic hygroma, thyroid mass, and ectopic thymic mass [14]. The preferred course of treatment for epidermoid cysts is complete removal by surgery [15]. Even asymptomatic cysts should be removed since they may change in size, leak, or become inflammatory [16]. The goal of early excision is to avoid subsequent infection.
CONCLUSION
A suprasternal epidermoid cyst is an exceptionally uncommon lesion in adolescent. It could therefore be misdiagnosed as malignancy. Due to the odd and deceptive clinical presentations, there is a greater likelihood of a diagnostic conundrum. Imaging is becoming increasingly important in surgical planning. It had aided us in determining the anatomy and type of the lesion. Successful removal of this type of cyst, which prevents recurrences, requires careful surgical dissection.
COMPLIANCE WITH ETHICAL STANDARDS
The procedure performed in this case report was in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
FUNDING
This study is not funded by any resources.
CONFLICT OF INTEREST
The author (s) declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this paper.
ETHICAL APPROVAL
For the purpose of publishing this case report, the patient's written informed consent was obtained.
REFERENCES
- Dutta M, Saha J, Biswas G, Chattopadhyay S, Sen I, Sinha R. (2013). Epidermoid cysts in head and neck: our experiences, with review of literature. Indian J Otolaryngol Head Neck Surg. 65(Suppl 1):14-21.
- Ciftci I, Sert A, Odabas D, Kocaoglu C, Kayacetin S. (2008). A rare suprasternal cystic neck mass in a pediatric patient: epidermoid cyst. Otolaryngol Head Neck Surg. 139(5):733-734.
- Handa U, Kumar S, Mohan H. (2002).Aspiration cytology of epidermoid cyst of terminal phalanx. Diagn Cytopathol. 26(4):266-267.
- Jham BC, Duraes GV, Jham AC, Santos CR. (2007). Epidermoid cyst of the floor of the mouth: a case report. J Can Dent Assoc. 73(6):525-528.
- Koca H, Seckin T, Sipahi A, Kaznac A. (2007). Epidermoid cyst in the floor of the mouth: report of a case. Quintessence Int. 38(6):473-477.
- Ozan F, Polat HB, Ay S, Goze F. (2007). Epidermoid cyst of the buccal mucosa: a case report. J Contemp Dent Pract. 8(3):90-96.
- Pancholi A, Raniga S, Vohra PA, Vaidya V. (2006). Midline submental epidermoid cyst: a rare case. Internet J Otorhinolaryngol. 4(2):1-5.
- Kandogan T, Koc M, Vardar E, Selek E, Sezgin O. (2007). Sublingual epidermoid cyst: a case report. J Med Case Rep. 1:87.
- Boo SH, Heo M, Han C. (2009). Multiple dermoid cysts of the external auditory canal. Int J Pediatr Otorhinolaryngol Extra. 4(4):158-161.
- Suzaki C, Maeda M, Matsumine A, Matsubara T, Taki W, Maier SE, et al. (2007). Apparent diffusion coefficient of subcutaneous epi-dermal cysts in the head and neck: comparison with intracranial epidermoid cysts. Acta Radiol. 14(9):1020-1028.
- Cameron D, Hilsinger R. (2003). Squamous cell carcinoma in an epidermal inclusion cyst: case report. Otolaryngol Head Neck Surg. 129(1):141-143.
- Morgan MB, Stevens GL, Somach S, Tamenbum M. (2001). Carcinoma arising in epidermoid cyst: a case series and aetiological investigation of human papilloma virus. Br J Dermatol. 145(3):505-506.
- Som P. (1987). Cystic lesions of the neck. Postgrad Radiol. 7:211‑236.
- Loney DA, Bauman NM. (1998). Ectopic cervical thymic masses in infants: a case report and review of the literature. Int J Pediatr Otorhinolaryngol. 43(1):77-84.
- Suliman M. (2005). Excision of epidermoid (sebaceous) cyst: description of the operative technique. Plast Reconstr Surg. 116(7):2042-2043.
- Han HH, Ju RK, Seo BF, Moon SH, Oh DY, Ahn ST, et al. (2014). Dermoid Cyst Excision under Müller Muscle in a Patient with Blepharoptosis. Arch Plast Surg. 41(5):607-609.