Information Links
Related Conferences
Previous Issues Volume 3, Issue 1 - 2023
Energy Balance and Management in Sports and Exercise
Begüm Ögün1, Mevhibe Tamirci2, Mehrad Pournaki3, Şermin TETİK*4
1Faculty of Pharmacy, Department of Biochemistry, Marmara University, Istanbul-Turkey
2European University of Lefke, Faculty of Pharmacy, LEFKE, Northern Cyprus, TR-10 Mersin, Turkey
3,4Final International University, Faculty of Pharmacy, Kyrenia via Mersin 10 Turkey, Turkish Republic of Northern Cyprus
*Corresponding author: Şermin TETİK, Final International University, Faculty of Pharmacy, Kyrenia via Mersin 10 Turkey, Turkish Republic of Northern Cyprus, Phone: +90 392 650 6666; Email: [email protected].
Received Date: December 22, 2022
Published Date: January 09, 2023
Citation: Tetik S, et al. (2023). Energy Balance and Management in Sports and Exercise. Mathews J Sports Med. 3(1):03.
Copyrights: Tetik S, et al. © (2023).
ABSTRACT
Energy balance is the balance between energy intake and energy expenditure. The energy balance has two main components. One of these two components is energy intake and the other is energy expenditure. Macro nutrients (carbohydrates, proteins and fats) are used as energy sources. During energy intake, food intake is also under control of hormones. These ingested nutrients are used in the production or resynthesize of ATP through energy metabolism. The energy released by the breakdown of ATP is used in all metabolic processes that require energy, including muscle contraction. In addition, although vitamins and minerals are not directly involved in energy production, they have functions in some metabolic reactions. Energy is consumed in three ways. One of these is resting metabolic rate, the other is the thermic effect of food, and the other is the energy spent through physical activity. Studies have shown that the energy taken in athletes is insufficient compared to the energy expenditure. Some researchers have stated that some amino acid and herbal supplements have positive effects on athlete performance.
Keywords: Energy Balance in Athletes, Energy Metabolism, Nutrients, Hormones, Dietary Supplements.
INTRODUCTION
In this review, energy balance in sports and exercise, macro and micro nutrients, energy metabolism responsible for ATP production, hormones involved in the regulation of appetite and energy intake, and dietary supplements commonly used by athletes were examined.
Energy Balance
When the energy intake is equal to the energy output, the body's energy balance is achieved.
Figure 1. Energy balance (http://www.mix-fit.net.au/energy-homeostasis-and-energy-balance/)
The energy provided by daily intake of protein, carbohydrates and fats is spent in three different ways. 60-75% of total energy spending (TES) is at resting metabolic rate (RMR), 10-30% is energy spent for physical activity (ESPA), and 10-15% is the thermic effect of food (TEF) [1].
When energy intake exceeds energy spending, a state of positive energy balance occurs, resulting in an increase in body mass. Conversely, when energy spending exceeds energy intake, a state of negative energy balance occurs, resulting in a loss of body mass [2].
Components of energy expenditure-Resting metabolic rate
Resting metabolic rate (RMR) represents the amount of energy required to maintain physiological functions at rest [3]. RMR indicates the amount of calories your body can burn in a resting position for 24 hours without any physical activity [4]. RMR constitutes the largest part of the total daily energy expenditure and corresponds to 60-75% of the daily energy expenditure in sedentary individuals and 50% in physically active individuals or athletes [5].
Energy expanded for physical activity (EEPA)
Physical activity is the bodily movements made by skeletal muscles, and the effect of physical activity on total energy expenditure is approximately 10-30%, although it varies from person to person. EEPA has two components. The first covers activities of daily living. The other is; Apart from the daily activities, it covers the energy expenditure in the exercises done to protect or improve the health and the regular training of the athletes [6].
ENERGY METABOLISM
Energy metabolism can be broadly defined as the capacity to do work. Muscles need energy during exercise [7].
The energy generated by the breakdown of food is not used directly in doing work, that is, it cannot be converted into mechanical energy. This energy is used to make adenosine triphosphate (ATP) [8]. The ability of ATP to be stored in the organism is very limited. ATP must be resynthesized immediately for the effort to continue [7]. The energy required for the resynthesis of ATP is provided by aerobic and/or anaerobic metabolisms.
Renewal of ATP is possible with any of the three energy systems [9]. Phosphogene System (Adenosine Triphosphate (ATP) Phosphocreatine (PC) System): It is an anaerobic energy system that releases energy by the breakdown of phosphocreatine stored in the muscle. The Anaerobic Glycolysis/Lactic Acid System is the anaerobic breakdown of glucose. Lactic acid is formed as the end product. Aerobic System means the oxidation of nutrients in mitochondria to provide energy [10].
Phosphogene system
ATP and phosphocreatine (PC) are stored in muscle cells. All of them are called phosphagens due ATP and PC have phosphate compounds in their structures [11]. Short-term acute exercises are performed by the energy released by the breakdown of these stored phosphogens. Due to during high-intensity activities, ATP is used up quite quickly and the organism's aerobic system is not capable of producing ATP at such a fast pace. This energy source is used for sudden, high-intensity work lasting up to 10 seconds [12].
Lactic acid system/anaerobic glycolysis
Since anaerobic glycolysis takes place in an oxygen-free environment, this process is called anaerobic glycolysis. Since lactic acid is produced as the final product while ATP is formed in this way, the system is also called the lactic acid system [13]. The glycogen stored in the muscle is broken down into glucose and two moles of pyruvic acid molecules are formed. In the absence of oxygen, pyruvic acid, which cannot enter the citric acid cycle, turns into lactic acid [14].
Anaerobic glycolysis is very important in training and competitions. Because in heavy loads, this system synthesizes ATP 2.5 times faster than aerobic metabolism, especially in trainings and competitions involving 2-3 minutes of maximum loading, energy needs more phosphogen and anaerobic glycolysis systems [15]. For example, in physical activities of 1-3 minutes at most, running 400 meters or 800 meters, the lactic acid system is activated for ATP energy. At the same time, in some sports, in middle distance races, the lactic acid system is of great importance in the last moments of the race. As it is known, when lactic acid reaches a high concentration in the muscles and blood, it causes fatigue. The acidic environment lowers the pH and the activities of some enzymes in the mitochondria are inhibited. This slows down the degradation rate of carbohydrates [16]. Lactic acid is metabolized in the body in various ways during rest after physical activity when oxygen is sufficient. For example; Since lactic acid is a product of the breakdown of carbohydrates, it is recycled into carbohydrates (Figure 2) [17].
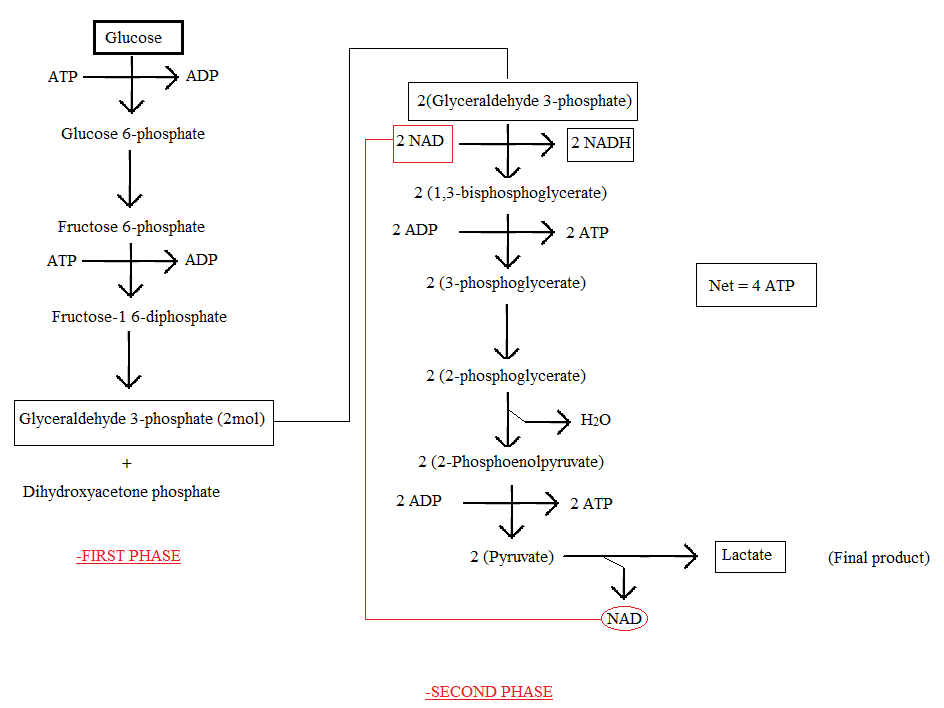
Figure 2. Lactic acid system/ Anaerobic glycolysis.
Aerobic metabolism
In the aerobic metabolism system, much more ATP is produced than in the anaerobic metabolism. Although ATP production is slower on the aerobic path, its capacity is almost unlimited.
In this system, CO2 and H2O are produced by the oxidation of carbohydrates, fats and proteins, which are essential nutrients [18]. In contrast to the anaerobic production of ATP in the cytoplasm of the cell, the oxidative production of ATP takes place within specialized cell organelles called mitochondria. Unlike anaerobic ATP production, the aerobic system is slow to operate, but its energy production capacity is much greater. For this reason, aerobic metabolism is the primary energy production method during endurance activities [19].
Examples of events where the main fuel route is the oxidative route include running 1,500 meters, marathons, half marathons, and endurance cycling or swimming 500 meters [20].
Aerobic glycolysis
The first steps in the aerobic energy pathway are the same as in anaerobic glycolysis, where one mole of glucose is converted to two moles of pyruvic acid. This step (aerobic glucose) takes place in the sarcoplasm. The main difference between the anaerobic pathway and this system is that lactic acid does not form [21,22].
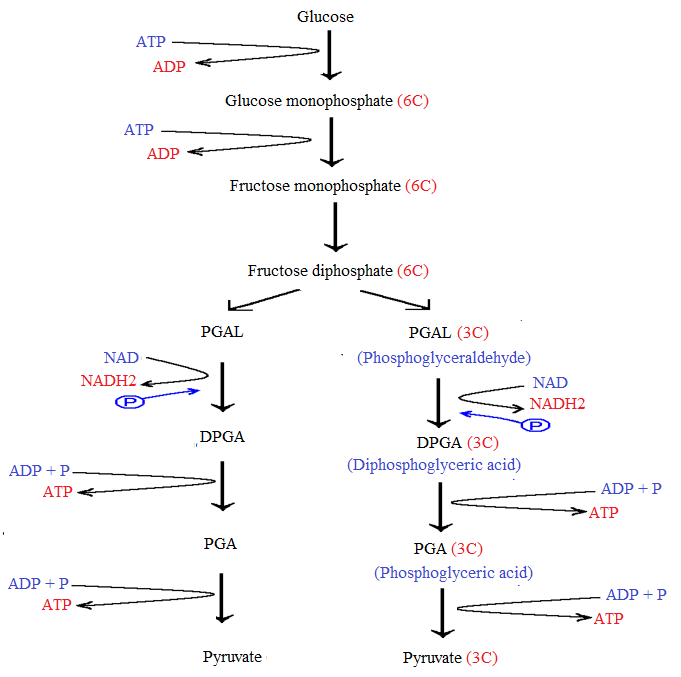
Figure 3. Aerobic glycolysis.
MACRO NUTRIENTS
Carbohydrates and proteins, one gram of which provides 4 kcal of energy, and fats, 1 gram of which provides 9 kcal of energy, are called macronutrients [23].
Carbohydrates and their role in body work
Carbohydrates are the primary and most preferred source of energy for all bodily functions. Carbohydrates are the most important component of energy metabolism in exercise [23].
All tissues use carbohydrates for their energy needs. If carbohydrates are taken in less than necessary amount, more ketones and acids are formed in the body. These molecules increase the acidity in body fluids and decrease the alkalinity of the blood. This condition is called ketosis. If the alkalinity of the blood is too low, it may cause coma [24]. Carbohydrates are used as fuel in the central nervous system and brain work [25]. Carbohydrates reduce the need for protein by preventing the use of protein for energy [24].
Carbohydrate consumption in athletes
Carbohydrates are the primary fuel in strength/power sports. Consuming carbohydrates adequately during the day not only supports glycogen stores during high-intensity training and competition, but also indirectly affects the development of muscle tissues [26].
It is recommended to increase the energy requirement of athletes with 60-65% carbohydrates and up to 70% in very intense training and endurance sports [27].
It is known that it is more appropriate to make carbohydrate consumption recommendations according to body weight rather than the percentage of energy in sports nutrition. In recommendations based on body weight, the general daily carbohydrate recommendation for athletes is 5-12 g/kg. However, it is stated that it should be 8-12 g/kg in very high intensity exercises [28].
Athletes have carbohydrate requirements that vary throughout the season based on training intensity, type of training, and timing. A summary of the requirements based on ISSN and IOC recommendations is listed in Table 1 [29].
Table 1. Summary of daily carbohydrate requirements according to ISSN and IOC recommendations [29].
|
Organization |
Physical Activity Level |
g/kg Daily |
|
ISSN |
General physical activity, 30-60 min / day, 3-4 times a week |
03-5 |
|
Medium to high intensity volume, 2-3 h/day, 5-6 times a week |
05-8 |
|
|
High volume, intense workout, 3-6 hours/day, 1-2 sessions, 5-6 times a week |
08-10 |
|
|
IOC |
low-intensity or skill-based activities |
03-5 |
|
Moderate exercise program, ~1 hour/day |
05-7 |
|
|
Endurance program, moderate to high intensity, 1-3 hours/day |
06-10 |
|
|
Strength training athletes |
04-7 |
|
|
Extreme adherence, medium to high intensity, > 4-5 hours/day |
08-12 |
High glycemic index carbohydrates taken after exercise increase insulin secretion and muscle endurance in the anabolic phase, shorten the recovery time in the muscles by taking part in protein synthesis and increase muscle density. Therefore, there is no harm in saying that carbohydrate and protein should be consumed together for faster muscle growth [30]. It is recommended to consume 6-10 g/kg/day of carbohydrates 3-4 hours before the training, and this amount corresponds to approximately 55-65% of the total energy need. The first half hour after training is the ideal time for carbohydrate consumption, and 1-1.5 g/kg carbohydrate should be consumed as soon as possible after exercise and this application should be repeated every 2 hours, especially for the first 6 hours. It should also be noted that each athlete's energy and carbohydrate needs may vary and differ from each other depending on the training intensity, age, body weight, and gender [32].
Fats and Fat Consumption in Athletes
Fats are nutrients that provide the energy needed by the body, just like carbohydrates. In this respect, fats are an essential resource used while performing physical activities[33]. In addition to being a source of energy, fats are necessary for the fat-soluble vitamins A, D, E, and K to dissolve and be used in metabolic processes [34]. Since fats stay in the body longer, the feeling of satiety is longer than carbohydrates and proteins [35].
Fats are used as an energy source, especially in long-term aerobic exercises. Although carbohydrates are the first energy source of the body, fats are also used as the main energy source in exercises lasting 1 hour or longer [27]. Although carbohydrates are stored in the body on a limited basis, every 0.5 kg of fat storage in the body provides an average of 3500 kcal of energy [36].
It is recommended that 20-25% of the total energy intake (ADA 2009) or 20-35% of the total energy intake should be provided from fats, close to the general population nutritional recommendations [37]. One-third of the daily fat requirement of the organism is from saturated, one-third monounsaturated and one-third polyunsaturated fats. Performance may be adversely affected by increasing fat consumption and decreasing carbohydrate consumption [38]. The use of a diet rich in fat reduces performance, decreases muscle strength and endurance [39]. When the energy provided from fat falls below 20%, problems such as deficiencies of fat-soluble vitamins, getting sick quickly, hormonal imbalance, and irregularity in blood pressure may occur in athletes. It is also stated that fat intake below 15% affects performance and blood lipids negatively. As a recommendation, the amount of energy obtained from fats should not fall below 15% and should not exceed 30% [40].
Proteins and Protein Consumption in Athletes
Protein can provide a source of carbon for energy reactions. Certain amino acids can be converted to glucose, metabolized for ATP or stored as fat [41]. Compared to carbohydrates and fats, the storage rate of proteins in the body is less. If there is a shortage of energy, the stored is used to meet this need [11]. Proteins are essential for growth, development and regeneration of various tissues and organs (skin, hair, nails and internal organs) rather than meeting their energy needs. Proteins are used in the repair of micro-tears that occur in muscle fibers during physical activities that require power and strength [42].
Protein is a nutrient that takes part in the production and repair of tissue in the body, muscle hypertrophy and the production of enzymes necessary for sports performance, and is necessary for recovery, repair and preservation of muscle mass during the training season [43]. Approximately 12-15% of the daily energy requirement of the athlete should be provided from proteins. A daily protein intake of 1.2-1.4 g/kg for endurance athletes and 1.6-1.7 g/kg for strength-training athletes is recommended [44]. More protein has been used by many athletes for years to increase muscle strength and growth, and to reduce muscle damage after intense exercise. The protein taken in excess of the requirement does not cause more muscle development in the body, and the amount taken in excess is stored in the body as fat in the adipose tissue.
MICRONUTRIENTS
Micronutrients (vitamins and minerals) have vital roles in energy metabolism, immune functions, antioxidant system, bone health, fluid-electrolyte balance, nervous system and muscle contraction in the human body. Micronutrients do not contribute to energy; however, some of them are involved in metabolic reactions in energy production [45].
Vitamin D
Vitamin D is associated with issues such as inflammation, stress fractures, muscle injuries, and upper respiratory tract infections. The intake of vitamin D through daily food consumption is insufficient, most of its need occurs in the presence of sunlight [46].Chronic musculoskeletal pain, muscle atrophy, slow muscle contraction, and increased muscle relaxation time are observed in vitamin D deficiency due to different sports [47]. Decreased vitamin D increases bone turnover, increasing the risk of bone injury. Stress fractures are common among athletes and are frequently seen in athletes. Adequate vitamin D levels reduce injuries, falls, muscle relaxation, muscle pain and weakness. Vitamin D is thought to be effective in maintaining and increasing optimal performance in athletes [48].
B group vitamins
B group vitamins are very important in the formation of adenosine triphosphate (ATP) using oxygen. In particular, thiamine (B1) is the vitamin most associated with energy intake. Since it is directly related to energy metabolism, its deficiency impairs performance, especially in endurance athletes. In addition to hemoglobin synthesis, vitamin B6 helps to break down glycogen stores during exercise and strengthens the immune system [49].
Vitamins E, A and C
Antioxidant vitamins clean the environment from free radicals. Especially in athletes, with the body's hard work, more energy is burned, which releases chemicals known as free radicals. Free radicals cause cell damage (oxidation), aging, heart diseases, cancer and diseases such as arthritis. The leading antioxidant substances that will neutralize free radicals are vitamins E, C, A and selenium from trace elements [50].
Because exercise is important for people of all ages, moderate exercise and a healthy diet can help prevent diseases including cancer, diabetes, heart disease, and cellular aging as well as muscular-skeletal disorders, obesity, and diabetes. Acute or difficult exercise can also cause muscular damage, cardiovascular maladaptation, and disruption of gut flora, as is well established. In actuality, vitamins A, B6, D, E, and K are necessary for exercise [51].
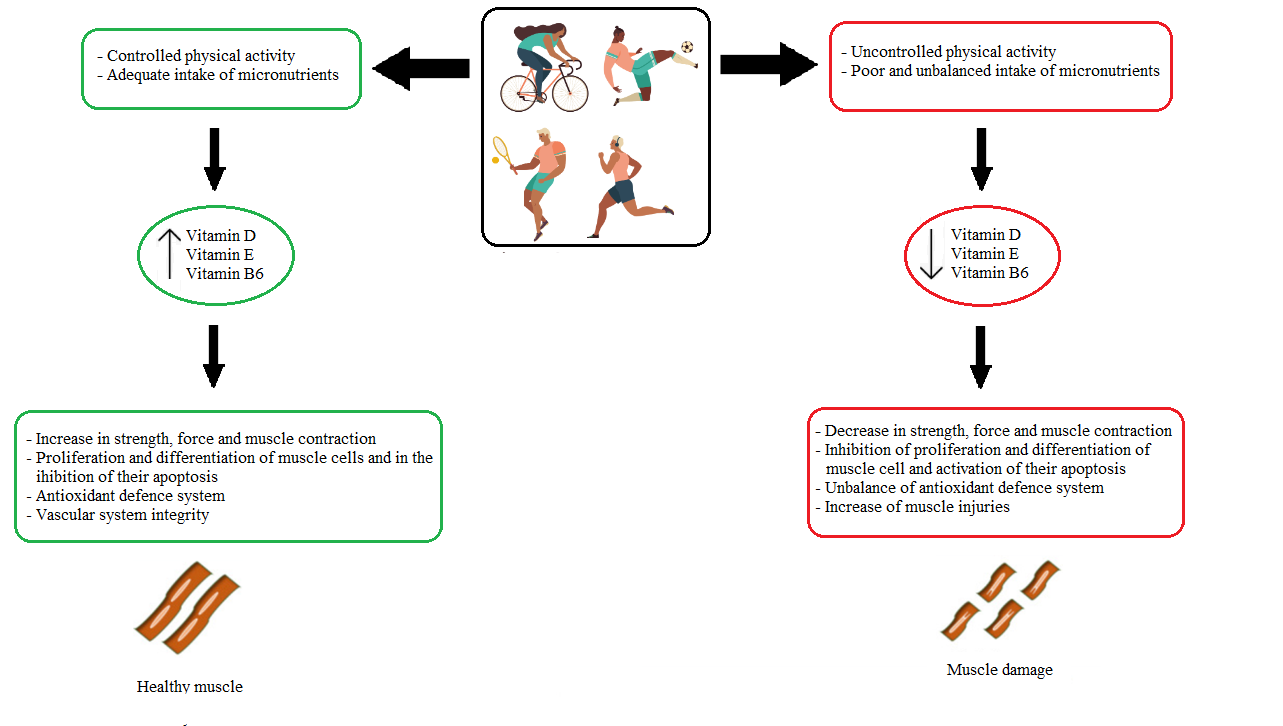
Figure 4. The role of vitamins in athlete’s muscle damage[52].
Minerals
Minerals; Establishment of acid-base balance, bone and dental health, neuromuscular functions, heart rhythm, enzyme and hormone components are involved in many different processes [53].
Iron
Iron is a mineral that plays a key role in sports performance. It has an important role in the formation of hemoglobin and myoglobin, which are responsible for oxygen transport [54]. Anemia due to the emptying of iron stores negatively affects sports performance . Iron deficiency impairs muscle function and working capacity with or without anemia [55].
Calcium
Calcium is one of the most abundant minerals in the body and is closely related to exercise performance. One of the main functions of calcium that affects exercise performance is to create bone density and the other is to take part in muscle contraction . Insufficient energy intake and insufficient calcium intake in female athletes cause decreases in bone-mineral density, increasing the risk of stress fracture and menstrual dysfunction [56].
Zinc
Zinc is a component of more than 300 enzymes, some of which are involved in functions important for physical performance, such as muscle energy production and protein synthesis [57]. It is a mineral that plays a role in energy metabolism, wound healing, cell membrane construction, antioxidant system, and is frequently lost in urine and sweat. It has been determined that the heavy training periods of the athletes cause zinc deficiency and that zinc is taken insufficiently in the diet among the athletes [53].
Magnesium
Another micronutrient that has functions on energy production, muscle contraction, protein synthesis and enzyme activation is magnesium. Magnesium is a mineral used in the production of muscle glycogen, which is an important energy source for athletes. It should not be ignored that magnesium loss will occur in athletes as a result of intense sweating [58]. Since it is effective in both aerobic and anaerobic energy metabolism, its deficiency may impair muscle functions; In particular, it is claimed that it may cause the need for more oxygen in the production of ATP in the respiratory chain. More oxygen demand negatively affects, especially in endurance branches . It has been claimed that the recommended daily intake (310-420 mg/day) is not sufficient to have an effect on performance. Its deficiency may be a cause of sudden death in sports linked to arrhythmia. Especially in endurance running, severe arrhythmia risk may occur with Mg deficiency as a result of excessive sweating. In addition, low Mg levels have been associated with an increased incidence of muscle cramps [59].
Sodium and Potassium
Sodium plays a role in the transmission of neural impulses, muscle contraction and water balance [60]. Sodium is responsible for maintaining blood volume and acid-base balance. Maintaining blood volume is important for sports performance. This situation is associated with the ability to transport nutrients to the cells, the removal of metabolic waste products from the cells, and the preservation of sweating level [27]. It plays a role in muscle contraction and glycogen storage, along with the transmission of nerve impulses such as potassium sodium [60]. Potassium is an electrolyte that helps regulate fluid balance, nerve conduction, and acid-base balance. Some research suggests that excessive increases or decreases in potassium may predispose athletes to cramps. The recommended potassium intake recommendation is 2000 mg per day [61].
Phosphorus and Selenium
Phosphorus is closely related to calcium. It constitutes approximately 22% of the total mineral content in our body. About 80% of these phosphorus, bound with calcium, provides strength and rigidity in bones. Phosphorus is necessary in metabolism to keep the cell membrane structure and blood pH constant. Phosphors play an important role in bioenergetics and are also required in the formation of ATP [62]. Selenium is a component of many enzymes, particularly glutathione peroxidase, an important cellular antioxidant enzyme. Theoretically, selenium supplementation could prevent peroxidation of erythrocyte membrane and muscle cell substrates involved in oxygen metabolism and possibly improve aerobic exercise performance [57].
PREVENTION OF DEHYDRATION IN ATHLETES
Dehydration is the loss of lliquid from the metabolism. It occurs as a result of losing 2% of body weight during competition or training [63]. Sufficient liquid consumption in athletes; It is necessary to prevent dehydration, which negatively affects strength, endurance and aerobic capacity. Sweat causes loss of body water as well as electrolytes. Na, K, Mg, Fe and Ca are the leading electrolytes excreted with sweat [64]. As a result of dehydration, successive events such as a decrease in blood volume, less blood pumping to the muscles, less transport of oxygen and nutrients to the cells, and a decrease in waste removal occur. In addition, hyponatremia may occur due to excessive sweating. As a result of these events, athlete performance is negatively affected [65]. Proper hydration during and after training is important for athletes to maintain their performance. 3–3.5 liters of liquid should be consumed 24 hours before training or competition, 400-600 milliliters 2-3 hours before, and 150 milliliters of liquid every 15 minutes during training or competition. After training or competition, depending on the exercise duration and intensity, at least 500 milliliters of fluid intake provides rehydration [66].
HORMONES THAT AFFECT APPETITE
Hormones released into the circulation through activity in the hypothalamus, brainstem and autonomic nervous system control our food intake and appetite [67]. Food intake is regulated by appetite and includes physiological needs such as eating pleasure, taste, taste and social life [68] .
Leptin, Cholecystokinin and Ghrelin
Leptin is secreted into the bloodstream as a peptide hormone consisting of 167 amino acids [69]. Leptin is synthesized by adipose tissue and released into the blood. Leptin released into the blood crosses the blood-brain barrier (BBB) and reaches the hypothalamus, binds to specific leptin receptors in various hypothalamic nuclei, reducing food intake and increasing energy use.While overeating, obesity, insulin, glucocorticoids, acute infection, proinflammatory cytokines (TNF-α, IL-1) increase leptin secretion from adipose tissue; hunger, cold, β-adrenergic agonists, testosterone and exercise reduce it [70]. Cholecystokinin is the first digestive system hormone to have a role in the regulation of appetite .CCK is produced in I cells in the doudenum and jejunum .CCK secretion increases during and after meals and suppresses hunger. CCK is secreted after a meal to reduce appetite and awakens satiety [71].
Ghrelin is a peptide hormone containing 28 amino acids produced by some endocrine cells in the gastric mucosa [72]. Ghrelin is a hormone that affects various processes related to eating, body weight and blood sugar regulation as well as stimulating the secretion of growth hormone (GH). Unlike most other metabolically effective gastrointestinal hormones, ghrelin acutely stimulates eating and also causes body weight gain with repeated administration as a result of its orexigenic effects and effects of reducing energy expenditure and preserving fat mass. Plasma ghrelin levels increase substantially during fasting and tend to decrease immediately after food intake. Therefore, ghrelin is also called "hunger hormone" [73].
Peptide YY, Adiponectin
PYY, a member of the pancreatic polypeptide family, is produced by L cells of the ileum, colon, and rectum, and its two endogenous forms (PYY1-36 and PYY3-36) are released into the circulation. PYY delays gastric emptying, inhibits pancreatic and gastric secretions, inhibits gallbladder contraction, and increases fluid and electrolyte absorption from the ileum. Plasma PYY concentrations are proportional to the energy content of meals, and higher plasma PYY concentrations occur especially after dietary fat intake [74]. While circulating PYY concentrations are low in fasting state, they increase rapidly after a meal. It is at highest level in the 2nd hour after the start of the meal and gradually decreases within 6 hours after reaching the highest value. PYY reduces appetite and increases satiety.It can inhibit eating for up to 12 hours, meaning its effect is slightly longer than other rapid regulators [75].
Adiponectin is a collagen-like plasma protein produced in adipose tissue. Although its amount is higher in subcutaneous white adipose tissue, plasma adiponectin levels decrease with the increase in visceral white adipose tissue and hypertrophic adipocytes. Circulating levels increase with weight loss and during hunger. Adiponectin provides weight loss by stimulating energy expenditure [76].
Glucocorticoids and Insulin
Glucocorticoid is an adrenal steroid hormone that plays an important role in adaptive responses to various types of stress and plays an important role in the control of the hypothalamus-pituitary-adrenal gland (HPA) neuroendocrine axis [77]. It is well known that administration of glucocorticoids stimulates appetite in some cases and, conversely, there is loss of appetite and weight loss in glucocorticoid deficiency. Primarily, adrenal cortisol defect causes anorexia. Excessive glucocorticoid secretion causes excessive gluttony [78].
Insulin is another hormone that suppresses hunger. Insulin is a polypeptide hormone secreted from beta cells in the islets of Langerhans, which are the hormonal secretion units of the pancreas . The effect of insulin on the appetite mechanism is similar to leptin. Insulin increases the release of leptin [79]. Insulin, which reaches the central nervous system through the circulatory system, has many receptors in the brain. Especially in the hypothalamus, ARC carries out its anorexigenic effects through its receptors in the nucleus [80].
HERBAL SUPPLEMENTS
Ginseng
Ginseng is one of the most popular herbal dietary supplements worldwide. Ginseng consists of many species in the Araliaceae family. Ginseng has important antioxidant properties that facilitate mitochondrial activity during exercise [81]. Given its anti-stress effects, one theory of ginseng supplementation is that it enhances sports performance by allowing athletes to train more intensely or create an anti-fatigue effect and increase endurance during competition [82].
Kava Kava (Piper Methysticum)
Kava tropical shrub plant Piper methysticum Forst F.' It is a traditional beverage used in ceremonial events in the South Pacific, prepared from the rhizome . Kava root contains kava lactones (cava pyrones). The neuropharmacological effects of Kava include analgesia, sedation, and skeletal muscle relaxation, but not central nervous system depression. It shows its effects by inducing relaxation with gamma aminobutyric (GABA) acid. Therefore, kavalactones have been theorized to reduce excessive anxiety and/or hand tremor that can impair performance in many sports such as archery and pistol shooting [82].
Ginkgo biloba
Ginkgo biloba is one of the most popular herbs grown in Asia. The active compounds of this plant are flavonoids and terpenoids. One of the tissue level effects is the stimulated release of endothelium-derived relaxant factor, which can increase muscle tissue blood flow through improved microcirculation. Such an effect may increase aerobic endurance by increasing muscle tissue oxidation [83].
St. John’s Worth (Hypericum Perforatum)
St. John's Wort (SJW) consists of dried parts of Hypericum perforatum. SJW can be theorized to reduce anxiety and hand tremor in some athletes. Unfortunately, no studies have emerged evaluating the potential ergogenic effect of kava or SJW supplementation on exercise or sports performance [84].
Capsaicin
Capsaicin (8-methyl-N-vanilyl-trans-6-nonenamide) is a chemical compound and phytochemical predominantly found in capsicum and first isolated in 1878. The United States Pharmacopoeia has classified capsaicin as a stimulant. Capsaicin can lead to stimulation of the sympathetic nervous system and sense of heat, leading to increased catecholamine concentrations and subsequent fat oxidation and energy expenditure. Because of these physiological effects, capsaicin has been investigated for its effects on weight loss [85].
AMINO ACID SUPPLEMENTS
Tryptophan
Tryptophan (TRYP) is a precursor for serotonin, a theoretical brain neurotransmitter for suppressing pain. Free tryptophan (FTRYP) enters brain cells to form serotonin. Therefore, tryptophan supplementation has been used to increase serotonin production in attempts to increase pain tolerance during intense exercise [86].
Branched chain amino acids
Although there are studies showing that branched-chain amino acids (BCAAs) increase protein synthesis, reduce protein breakdown, and prevent muscle fatigue, it has been determined that they improve physical performance and prevent nervous system fatigue by reducing tryptophan entry to the brain during exercise [87].
Aspartates
Potassium and magnesium aspartates are salts of aspartic acid, an amino acid. It has been used ergogenically, possibly by increasing fatty acid metabolism and reducing muscle glycogen use or reducing ammonia accumulation during exercise [88].
Tyrosine
Tyrosine is a precursor for catecholamine hormones and neurotransmitters, particularly epinephrine, norepinephrine, and dopamine. Oral doses of tyrosine increase circulating concentrations of adrenaline, noradrenaline, and dopamine, both in the central nervous system and in the periphery. These are heavily involved in the regulation of bodily functions during physical stress and exercise [89].
Taurine
Taurine is a non-essential sulfur-containing amino acid. The mechanism by which taurine enhances exercise performance is not fully known. It is thought that it can increase exercise performance by regulating calcium homeostasis and increasing myocardial and skeletal muscle contraction under strenuous conditions [90].
Glutamine
Glutamine is the most common amino acid in the body and has important roles in the body. Some of those; wound healing, being a source of energy, providing nitrogen transfer and regulating protein synthesis. It is known that prolonged exercise session and heavy exercise periods reduce plasma glutamine concentration and this situation is a potential cause of exercise-induced immune system disorder and glutamine supplementation is used with the claim that it will increase susceptibility to infection in athletes [91].
Ornithine, lysine and arginine
Ornithine, lysine and arginine have been used in attempts to increase human growth hormone (HGH) production, the theory being to increase lean muscle mass and strength [86]. It can be theorized that arginine supplementation is ergogenic because it is a substrate for nitric oxide (NO) synthesis, a potent endogenous vasodilator that may benefit blood flow and endurance capacity. Arginine expands blood vessels and provides more oxygen and nutrients needed by the muscle, while helping to remove metabolic byproducts such as carbon dioxide and lactic acid [86].
CONCLUSION
In order to achieve energy balance, energy intake must be equal to energy expenditure. Energy intake is provided from protein, carbohydrates and fats. Carbohydrates taken are stored in the body as glycogen. Inadequate consumption of carbohydrates by athletes, as they support glycogen stores and are effective on blood sugar levels, delays rest and regeneration in the muscles. When there is a decrease in glycogen stores, endurance and sports performance are also negatively affected. Fats are used as an energy source in long-term aerobic exercises. The use of fats as an energy source affects performance positively by preventing the emptying of glycogen stores. However, performance may be adversely affected due to the decrease in carbohydrate consumption by increasing fat consumption. Protein consumption after exercise or competition contributes to the repair of muscle tissue. With adequate protein consumption, recovery occurs quickly. In addition, adequate protein consumption of the athlete is important for maintaining positive nitrogen balance and stimulating muscle protein synthesis.
Although vitamins and minerals (micronutrients) cannot be used directly in energy production, some of them are involved in metabolic reactions in energy production. The decrease of micronutrients below a certain level harms sports performance.
Liquid consumption is also important for athlete performance. As a result of dehydration, events such as a decrease in blood volume, less blood pumping to the muscles, less transport of oxygen and nutrients to the cells, and reduced waste removal occur. As a result of these events, athlete performance is adversely affected.
Anaerobic glycolysis is very important in training and competitions. Because this system synthesizes ATP faster than aerobic metabolism in heavy loads. Although ATP production is slower on the aerobic path, its capacity is almost unlimited. Food intake is regulated by appetite. Some hormones in our body are effective in regulating appetite. Cholecystokinin, peptide YY, insulin, leptin hormones play a role in suppressing appetite. High levels of glucocorticoids stimulate appetite, while low levels cause appetite and weight loss. Adiponectin increases energy expenditure. Unlike other hormones, the plasma levels of the hormone ghrelin, known as the hunger hormone, increase in the fasting state and stimulate hunger and nutrition.
Dietary supplements and amino acids are used to improve sports performance. Tryptophan supplementation is used to increase tolerance to pain during intense exercise by increasing serotonin production. Branched-chain amino acids increase protein synthesis and reduce degradation, prevent muscle fatigue and are used as a fuel source for long-term exercises. Aspartates are thought to delay fatigue by removing ammonia from the blood. Because arginine is an endogenous vasodilator, it expands blood vessels and provides more oxygen and nutrients needed by the muscle. Tyrosine increases circulating adrenaline, noradrenaline and dopamine concentrations in both the central nervous system and the periphery. Tyrosine has been suggested to be ergogenic, as some have suggested that inadequate production of these hormones or transmitters may compromise optimal physical performance. It is thought that taurine can improve exercise performance by regulating calcium homeostasis and increasing myocardial and skeletal muscle contraction in strenuous conditions. Ornithine, lysine, and arginine have been used in attempts to increase human growth hormone production.
AUTHOR DISCLOSURE
The authors declare to have no commercial associations and no competing financial interest.
ACKNOWLEDGEMENTS
This work was not supported by grant.
REFERENCES
- Bosy-Westphal A, Hägele FA, Müller MJ. (2021). What Is the Impact of Energy Expenditure on Energy Intake? Nutrients. 13(10):3508.
- Hill JO, Wyatt HR, Peters JC. (2012). Energy balance and obesity. Circulation. 126(1):126-132.
- Tortu E, Deliceoğlu G, Kocahan T, Hasanoğlu A. (2017). Comparison of Resting Metabolic Rates Measured by Indirect Calorimetry with Some Estimation Formulas. Journal of Sport Sciences. 28(2):103-114.
- Uygur E. (2010). Investigation of aerobic exercise capacity, resting metabolic rate, respiratory functions and body composition in individuals with different body mass indexes. Turkey: (Master's thesis, University of Afyon Kocatepe, Health Sciences Institute).
- Johns DJ, Hartmann-boyce J, Jebb SA, Aveyard P, Behavioural Weight Management Review Group. (2014). Diet or exercise interventions vs combined behavioral weight management programs: A systematic review and meta-analysis of direct comparisons. J Acad Nutr Dietet. 114(10):1557-1568.
- Moghetti P, Bacchi E, Brangani C, Donà S, Negri C. (2016). Metabolic Effects of Exercise. Front Horm Res. 47:44-57.
- İpekoğlu G. (2013). Changes in Fat Oxidation Rate During Intermittent and Continuous Aerobic Exercise. Published Master's Thesis.
- Westerterp KR. (2000). Control of energy expenditure in humans. [Updated 2016 Nov 11]. Endotext [Internet]. South Dartmouth (MA): MDText. com, Inc.
- Tortum AC. (2017). The effect of core stabilization exercises applied to female volleyball players on balance and anaerobic performance (Doctoral dissertation, University of Ankara Yıldırım Beyazıt, Health Sciences Institute, Turkey).
- Pontzer H, Durazo-Arvizu R, Dugas LR, Plange-Rhule J, Bovet P, Forrester TE, et al. (2016). Constrained Total Energy Expenditure and Metabolic Adaptation to Physical Activity in Adult Humans. Curr Biol. 26(3):410-417.
- Beis I, Newsholme EA. (1975). The contents of adenine nucleotides, phosphagens and some glycolytic intermediates in resting muscles from vertebrates and invertebrates. Biochem J. 152(1):23-32.
- Dunn J, Grider MH. (2021). Physiology, adenosine triphosphate. In StatPearls [Internet]. USA: StatPearls Publishing.
- Barclay CJ. (2011). Energetics of contraction. Comprehensive Physiology. 5(2):961-995.
- Kurt Y. (2015). Comparison of balance measurements in elite freestyle wrestlers by weight.
- Melkonian EA, Schury MP. (2019). Biochemistry, anaerobic glycolysis. USA: StatPearls Publishing.
- Peek CB, Levine DC, Cedernaes J, Taguchi A, Kobayashi Y, Tsai SJ, et al. (2017). Circadian Clock Interaction with HIF1α Mediates Oxygenic Metabolism and Anaerobic Glycolysis in Skeletal Muscle. Cell Metab. 25(1):86-92.
- Péronnet F, Aguilaniu B. (2014). Physiological significance and interpretation of plasma lactate concentration and pH in clinical exercise testing. Rev Mal Respir. 31(6):525-551.
- Chen Y, Fry BC, Layton AT. (2017). Modeling glucose metabolism and lactate production in the kidney. Math Biosci. 289:116-129.
- Tatlıci A. (2017). Effect of acute dietary nitrate supplementation on anaerobic power in elite boxers. Selcuk University Institute of Health Sciences, Master Thesis, 2017, Konya (Supervisor: Assoc. Prof. Dr. Oktay Çakmakçı).
- Péronnet F, Aguilaniu B. (2014). Signification physiologique et interprétation clinique de la lactatémie et du pH au cours de l’EFX incrémentale. Rev Mal Respir. 31(6):525-551.
- Naifeh J, Dimri M, Varacallo M. (2021). Biochemistry, aerobic glycolysis. In StatPearls [Internet]. USA: StatPearls Publishing.
- Schurr A, Payne RS. (2007). Lactate, not pyruvate, is neuronal aerobic glycolysis end product: an in vitro electrophysiological study. Neuroscience. 147(3): 613-619.
- Dashty M. (2013). A quick look at biochemistry: carbohydrate metabolism. Clin Biochem. 46(15): 1339-1352.
- Yakupova EI, Bocharnikov AD, Plotnikov EY. (2022). Effects of Ketogenic Diet on Muscle Metabolism in Health and Disease. Nutrients. 14(18):3842.
- Westerblad H, Bruton JD, Katz, A. (2010). Skeletal muscle: energy metabolism, fiber types, fatigue and adaptability. Exp Cell Res. 316(18):3093-3099.
- Sahlin K, Tonkonogi M, Söderlund K. (1998). Energy supply and muscle fatigue in humans. Acta Physiol Scand. 162(3):261-266.
- Çetiner Okşin B. (2019). Energy Balance and Food Consumption Trends in Female Basketball Players.
- Evans M, Cogan KE, Egan B. (2017). Metabolism of ketone bodies during exercise and training: physiological basis for exogenous supplementation. J Physiol. 595(9):2857-2871.
- Bytomski JR. (2018). Fueling for performance. Sports Health. 10(1):47-53.
- Boison D. (2017). New insights into the mechanisms of the ketogenic diet. Curr Opin Neurol.. 30(2):187-192.
- Akyol H. (2018). Examining the nutritional habits and knowledge level of support product use of elite skiers (Master's thesis, University of Ağrı İbrahim Çeçen, Social Sciences Institute, Turkey).
- Bora Z. (2015). Determination of nutritional status and nutritional support product usage of sports instructors working in the gym doing bodybuilding sports. (Master's thesis,University of Başkent, Social Sciences Institute, Turkey).
- Yang Z, Mi J, Wang Y, Xue L, Liu J, Fan M, et al. (2021). Effects of low-carbohydrate diet and ketogenic diet on glucose and lipid metabolism in type 2 diabetic mice. Nutrition. 89:111230.
- Kurt A. (2018). Investigation of the nutritional habits and nutrition awareness levels of female students in the 14-17 age group who do and do not actively do sports. (Master's thesis, University of İstanbul Gelişim, Social Sciences Institute, Turkey).
- Muscella A, Stefàno E, Lunetti P, Capobianco L, Marsigliante S. (2020). The regulation of fat metabolism during aerobic exercise. Biomolecules. 10(12):1699.
- Peric R, Meucci M, Bourdon PC, Nikolovski Z. (2017). Does the aerobic threshold correlate with the maximal fat oxidation rate in short stage treadmill tests? J Sports Med Phys Fitness. 58(10):1412-1417.
- O’Hearn K, Tingelstad HC, Blondin D, Tang V, Filion LG, Haman F. (2016). Heat exposure increases circulating fatty acids but not lipid oxidation at rest and during exercise. J Therm Biol. 55:39-46.
- Demirci Ü. (2012). Determination of body composition, use of nutritional support, nutritional habits in people who exercise for health purposes (Master's thesis, Social Sciences Institute).
- Purdom T, Kravitz L, Dokladny K, Mermier C. (2018). Understanding the factors that effect maximal fat oxidation. J Int Soc Sports Nutr. 15(1):3.
- Lundsgaard AM, Fritzen AM, Kiens B. (2018). Molecular regulation of fatty acid oxidation in skeletal muscle during aerobic exercise. Trends Endocrinol Metab. 29(1):18-30.
- Eskici G. (2015). Nutrition in team sports. Journal of Human Sciences. 12(2):244-265.
- Carbone JW, Pasiakos SM. (2019). Dietary protein and muscle mass: translating science to application and health benefit. Nutrients. 11(5):1136.
- Thomas DT, Erdman KA, Burke LM. (2016). Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: nutrition and athletic performance. J Acad Nutr Diet. 116(3):501-528.
- Morton RW, Murphy KT, McKellar SR, Schoenfeld BJ, Henselmans M, Helms E, et al. (2018). A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br J Sports Med. 52(6):376-384.
- Celep GS, Kaynar P, Rastmanesh R. (2017). Biochemical functions of micronutrients. Adv Obes Weight Manag Control. 6(2):43-45.
- Hamilton B. (2011). Vitamin D and athletic performance: the potential role of muscle. Asian J Sports Med. 2(4):211.
- de la Puente Yagüe M, Collado Yurrita L, Ciudad Cabañas MJ, Cuadrado Cenzual MA. (2020). Role of vitamin d in athletes and their performance: Current concepts and new trends. Nutrients. 12(2):579.
- Volpe SL. (2014). Vitamin D and Exercise Performance. ACSM's Health & Fitness Journal. 18(3):28-30.
- Manore MM. (2000). Effect of physical activity on thiamine, riboflavin, and vitamin B-6 requirements. Am J Clin Nutr. 72(2):598S-606S.
- Brancaccio M, Mennitti C, Cesaro A, Fimiani F, Vano M, Gargiulo B, et al. (2022). The Biological Role of Vitamins in Athletes’ Muscle, Heart and Microbiota. Int J Environ Res Public Health. 19(3):1249.
- Kerksick CM, Wilborn CD, Roberts MD, Smith-Ryan A, Kleiner SM, Jäger R, et al. (2018). ISSN exercise & sports nutrition review update: research & recommendations. J Int Soc Sports Nutr. 15(1):38.
- Lavie CJ, DiNicolantonio JJ, Milani RV, O’Keefe JH. (2013). Vitamin D and cardiovascular health. Circulation. 128(22):2404-2406.
- McClung JP, Gaffney-Stomberg E, Lee JJ. (2014). Female athletes: a population at risk of vitamin and mineral deficiencies affecting health and performance. J Trace Elem Med Biol. 28(4):388-392.
- Rubeor A, Goojha C, Manning J, White J. (2018). Does iron supplementation improve performance in iron-deficient nonanemic athletes? Sports Health. 10(5):400-405.
- Marzban M, Nabipour I, Farhadi A, Ostovar A, Larijani B, Darabi AH, et al. (2021). Association between anemia, physical performance and cognitive function in Iranian elderly people: evidence from Bushehr Elderly Health (BEH) program. BMC Geriatr. 21(1):1-17.
- Sale C, Elliott-Sale KJ. (2019). Nutrition and athlete bone health. Sports Medicine. 49(2):139-151.
- Guest NS, VanDusseldorp TA, Nelson MT, Grgic J, Schoenfeld BJ, Jenkins NDM, et al. (2021). International society of sports nutrition position stand: caffeine and exercise performance. J Int Soc Sports Nutr. 18(1):1.
- Zhang Y, Xun P, Wang R, Mao L, He K. (2017). Can magnesium enhance exercise performance? Nutrients. 9(9):946.
- Moretti A. (2021). What is the role of magnesium for skeletal muscle cramps? A Cochrane Review summary with commentary. J Musculoskelet Neuronal Interact. 21(1):1-3.
- Munson EH, Orange ST, Bray JW, Thurlow S, Marshall P, Vince RV. (2020). Sodium Ingestion Improves Groundstroke Performance in Nationally-Ranked Tennis Players: A Randomized, Placebo-Controlled Crossover Trial. Front Nutr. 7:549413.
- Toktaş N, Demirörs R. (2020). Teniste Beslenme. Beslenme ve Diyet Dergisi. 48(2):100-108.
- Gürsoy R, Dane Ş. Nutrition and nutritional ergogenics II: Vitamins and minerals/Noutrions and noutrionals ergogenics. Journal of Physical Education and Sport Sciences. 4(1).
- Kenefick RW, Cheuvront SN. (2012). Hydration for recreational sport and physical activity. Nutrition reviews. 70(suppl_2):S137-S142.
- Baker LB, Wolfe AS. (2020). Physiological mechanisms determining eccrine sweat composition. Eur J Appl Physiol. 120(4):719-752.
- Chapman RF, Stickford JL, Levine BD. (2010). Altitude training considerations for the winter sport athlete. Exp Physiol. 95(3):411-421.
- Maughan RJ, Shirreffs SM. (2010). Development of hydration strategies to optimize performance for athletes in high‐intensity sports and in sports with repeated intense efforts. Scand J Med Sci Sports. 20(Suppl 2):59-69.
- Tetik, Ş. Nutritional Biochemistry. İstanbul: Nobel Publication Distribution.
- Kristeller JL. (2015). Mindfulness, eating disorders, and food intake regulation. In: Ostafin BD, Robinson MD & Meier BP, (Eds). Handbook of mindfulness and self-regulation. Germany: Springer Science + Business Media. p. 199-215.
- Dando R, Roper SD. (2011). Controlling what we eat: How circulating peptide hormones influence taste and appetite. The Biochemist. 33(6):14-17.
- Hocking S, Samocha-Bonet D, Milner KL, Greenfield JR, Chisholm DJ. (2013). Adiposity and insulin resistance in humans: the role of the different tissue and cellular lipid depots. Endocrine reviews. 34(4):463-500.
- Steinert RE, Feinle-Bisset C, Asarian L, Horowitz M, Beglinger C, Geary N. (2017). Ghrelin, CCK, GLP-1, and PYY (3–36): secretory controls and physiological roles in eating and glycemia in health, obesity, and after RYGB. Physiological reviews. 97(1):411-463.
- Sakata I, Sakai T. (2010). Ghrelin cells in the gastrointestinal tract. Int J Pept. 2010:945056.
- Cheng MHY, Bushnell D, Cannon DT, Kern M. (2009). Appetite regulation via exercise prior or subsequent to high-fat meal consumption. Appetite. 52(1):193-198.
- Meguid MM, Glade MJ, Middleton FA. (2008). Weight regain after Roux-en-Y: a significant 20% complication related to PYY. Nutrition. 24(9):832-842.
- Erdmann J, Topsch R, Lippl F, Gussmann P, Schusdziarra V. (2004). Postprandial response of plasma ghrelin levels to various test meals in relation to food intake, plasma insulin, and glucose. J Clin Endocrinol Metab. 89(6):3048-3054.
- Kubota N, Yano W, Kubota T, Yamauchi T, Itoh S, Kumagai H, et al. (2007). Adiponectin stimulates AMP-activated protein kinase in the hypothalamus and increases food intake. Cell Metab. 6(1):55-68.
- Giordano R, Pellegrino M, Picu A, Bonelli L, Balbo M, Berardelli R, et al. (2006). Neuroregulation of the hypothalamus-pituitary-adrenal (HPA) axis in humans: effects of GABA-, mineralocorticoid-, and GH-Secretagogue-receptor modulation. The Scientific World Journal. 6:1-11.
- Raff H, Sharma ST, Nieman LK. (2014). Physiological basis for the etiology, diagnosis, and treatment of adrenal disorders: Cushing’s syndrome, adrenal insufficiency, and congenital adrenal hyperplasia. Compr Physiol. 4(2):739-769.
- Melanson KJ, Zukley L, Lowndes J, Nguyen V, Angelopoulos TJ, Rippe JM. (2007). Effects of high-fructose corn syrup and sucrose consumption on circulating glucose, insulin, leptin, and ghrelin and on appetite in normal-weight women. Nutrition. 23(2):103-112.
- Yousefvand S, Hamidi F. (2021). The role of ventromedial hypothalamus receptors in the central regulation of food intake. International Journal of Peptide Research and Therapeutics. 27(1):689-702.
- Sng KS, Li G, Zhou LY, Song YJ, Chen XQ, Wang YJ, et al. (2022). Ginseng extract and ginsenosides improve neurological function and promote antioxidant effects in rats with spinal cord injury: A meta-analysis and systematic review. J Ginseng Res. 46(1):11-22.
- Zhong L, Zhao L, Yang F, Yang W, Sun Y, Hu Q. (2017). Evaluation of anti-fatigue property of the extruded product of cereal grains mixed with Cordyceps militaris on mice. J Int Soc Sports Nutr. 14(1):15.
- Mahadevan S, Park Y. (2008). Multifaceted therapeutic benefits of Ginkgo biloba L.: chemistry, efficacy, safety, and uses. J Food Sci. 73(1):R14-R19.
- Yavuz HU, Özkum D. (2014). Herbs potentially enhancing sports performance. Current Topics in Nutraceutical Research. 12.
- Antonio AS, Wiedemann LSM, Junior VV. (2018). The genus Capsicum: a phytochemical review of bioactive secondary metabolites. RSC advances. 8(45):25767-25784.
- Williams M. (2005). Dietary supplements and sports performance: amino acids. J Int Soc Sports Nutr. 2(2):63-67.
- Wolfe RR. (2017). Branched-chain amino acids and muscle protein synthesis in humans: myth or reality? J Int Soc Sports Nutr.. 14(1):30.
- Trudeau F. (2008). Aspartate as an ergogenic supplement. Sports Med. 38(1):9-16.
- Salamanca N, Giráldez I, Morales E, de La Rosa I, Herrera M. (2020). Phenylalanine and tyrosine as feed additives for reducing stress and enhancing welfare in gilthead seabream and meagre. Animals (Basel). 11(1):45.
- Kp AD, Martin A. (2022). Recent insights into the molecular regulators and mechanisms of taurine to modulate lipid metabolism: a review. Crit Rev Food Sci Nutr. p. 1-13.
- Posey EA, Bazer FW, Wu G. (2021). Amino acids and their metabolites for improving human exercising performance. Adv Exp Med Biol. 1332:151-166.