Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2025
Embryological Development of Persistent Cloaca. Hypothesis
Michael D Levin*
Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus and Dorot. Medical Center for rehabilitation and geriatrics. Netanya. Israel
*Corresponding Author: Michael D Levin, MD, PhD, DSc, Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus & Dorot. Medical Center for rehabilitation and geriatrics, Netanya, Israel, Tel: 972-538281393, ORCID: 0000-0001-7830-1944, E-mail: [email protected]; [email protected]
Received Date: February 20, 2025
Published Date: March 04, 2025
Citation: Levin MD. (2025). Embryological Development of Persistent Cloaca. Hypothesis. Mathews J Surg. 8(1):37.
Copyrights: Levin MD. © (2025).
ABSTRACT
Introduction: While some authors suggest that anorectal malformations (ARMs) arise from abnormal development of the cloaca, only the true cloaca arises because of the cessation of the division of the cloaca stopping at the stage of development characteristic of female birds and reptiles. It is characterized by the confluence of the rectum, uterus, and bladder into a wide space, resulting in the complete absence of the urethra, vagina, and anal canal. Currently, following the articles by Hendren and Peña, persistent cloaca is the name given to the pathology that was previously called ARM with vaginal fistula. These patients have a urethra, vagina, and anal canal that supposedly merge into a common narrow channel. These patients are operated on as if they were patients with a true cloaca. Results: As a result of an analysis of literature and our own research, it has been shown that with all types of ARMs, except for the true cloaca, the pathology develops at a later embryonic period because of impaired development of the exodermal rudiment of the anal canal. By this time, normal development of the anal canal occurs up to the subcutaneous tissue. When the IAS does not encounter the ectodermal rudiment, as evidenced by the absence of the anus, it deviates forward and upward, forming a narrow, rigid fistula. This process leads to the ectopic positioning of the anus on the perineum, vestibule, urethra, or vagina. What surgeons typically remove during the pull-through procedure, under the guise of a fistula, is a functioning anal canal. A short, rigid fistula forms in the wall of the organ through which the IAS penetrates. Conclusion: Unlike a true cloaca, a persistent cloaca develops due to the penetration of the IAS through the vaginal wall before a cavity has formed within the vagina. As a result, the IAS creates a narrow long fistula that, in some cases, obstructs the emptying of the upper part of the vagina, leading to hydrocolpos. These patients typically have a normally functioning bladder and urethra, and in some cases, a functioning anal canal has been documented. Poor outcomes are the result of unnecessary and mutilating surgeries.
Keywords: Embryology Anorectal Malformations, Embryology Persistent Cloaca, Pathophysiology ARM, Diagnosis, Treatment, Hypothesis.
INTRODUCTION
Knowledge of embryology is crucial for understanding anorectal malformations (ARMs) [1]. However, there are more hypotheses in the literature than established scientific facts. The embryologist Kluth described this problem as follows: “Today, the normal and abnormal development of the hindgut is still a matter of speculation. (1) the embryonic cloaca never passes through a stage resembling any form of anorectal malformation in neonates, including the so-called 'cloacas' in female embryos, and (2) studies on abnormal embryos are essential to explain abnormal development" [2].
THE TRUE CLOACA
From an embryological point of view, "Persistent Cloaca is a rare condition that occurs only in female infants. It results from the total failure of the urorectal septum to descend and therefore occurs at an exceedingly early stage of development (10-mm stage)" [3]. This condition is an example of atavism, where development halts at a stage typical of birds and reptiles. It is characterized by the confluence of the rectum, uterus, and bladder into a wide space called a urogenital sinus, resulting in the complete absence of the urethra, vagina, and anal canal. Because of this, children with this defect cannot control urination and bowel movements. Until 1982, isolated cases of cloaca were described. Okonkwo and Crocker wrote in 1977 that “Cloacal dysgenesis is a rare anomaly. Fifty cases have been reported in the literature” [4].
INDISPUTABLE SCIENTIFIC FACTS OF ANORECTAL EMBRYOLOGICAL DEVELOPMENT
- The genitourinary septum descends and separates the cloaca into two channels: the rectum posteriorly, and the bladder and urethra (urethra and vagina in females) anteriorly [3,5].
- Immediately after cloacal separation, the internal anal sphincter (IAS) is located away from its intended site in the ectoderm (perineum). “Normally, in the post-cloacal period, the endodermal internal anal sphincter migrates in the craniocaudal direction to meet with the ectodermal portion” [6]. This refers to the unique ability of the IAS to create a channel through the tissues of the perineum and it occurs after the division of the cloaca, i.s., the post cloacal period.
- The anal canal is divided into superior and inferior parts. The superior two-thirds are derived from the endoderm and are lined by simple columnar epithelial cells. The inferior one-third is derived from ectoderm and is lined by stratified squamous epithelial cells. The junction between these two types of epithelia is called the pectinate line or the dentate line [1,2,4].
- During the 10th week, the anal tubercles, a pair of ectodermal swellings around the proctodeal pit, fuse dorsally to form a horseshoe-shaped structure and anteriorly to create the perineal body [3]. This suggests that the formation of the distal ectodermal part of the IAS begins from the perineum and occurs through upward migration to meet the endodermal part of the IAS.
- According to the study of Nobles (1984), at the junction of the endodermal and exodermal rudiments, the anal membrane at first appears, which ruptures during embryos with a length of 13.5–135 cm [7]. Nievelstein et al. obtained the same data. [8].
- Nievelstein et al based on embryological observations, concluded that the abnormal communications, usually called fistulae, should be regarded as ectopic anal orifices. Anorectal malformations with the anus in normal position are best explained as late embryonic defects [8].
These undeniably reliable data lead to the conclusion that ARMs may occur during two periods of embryological development: (1). Only the true cloaca develops because of the cessation of the development of the anorectum in females, since the cloaca normally develops in female birds and reptiles for fertilization and egg release. Therefore, the cloaca has wide lumen and elastic walls. (2). All other types of ARMs occur at a later period, when the cloaca has already been divided into the urethra, vagina, and anal canal. In these cases, the pathology occurs because of a violation of the connection between the endodermal and ectodermal parts of the anal canal. Evidence of this is the absence of the anal opening in the ring of the subcutaneous portion of the external anal sphincter (EAS). Atresia/stenosis of the rectum, and ARM type H also develop in the post-cloacal embryonic period with a violation of the ectodermal part of the anal canal of another nature [9-11].
REGULARITIES OF PATHOLOGICAL ANATOMY AND PHYSIOLOGISTS OF ARMS
- All the fistulas are in the projection of the central sagittal plane. They are always displaced forward and upward from where the anus is normally located.
- In cases of visible (perineal and vestibular) fistulas, they are slightly displaced upward from the anal dimple. The degree of upward displacement increases in cases of invisible fistulas.
- In all cases of visible (perineal and vestibular) fistulas, there is a normally functioning anal canal, as evidenced by X-ray [12] and manometric studies [12,13], as well as the successful outcomes of the cutback procedure, which does not damage the anal canal [14]. These postulates are discussed in detail below.
- Radiological studies at ARMs
- ARMs with visible fistula.
On X-ray examination of patients with perineal and vestibular fistulas at rest, the anal canal is defined as the zone of constant contraction between the rectum and anus, near which a contrast marker is located. It contracts around the catheter inserted into the rectum, and as it does normally, preventing fecal leakage (Figure 1a, c). Its length corresponds to the normal length of the anal canal for the child's age. During attempts at bowel movements, the anal canal opens widely, as it should, to reduce resistance to the passage of feces (Figure 1b).
.png)
Figure 1. Lateral radiographs of the anorectum in patients with ARMs with visible fistulas. (ab). Images of the same child taken at various times. (a). A catheter was inserted through the vestibular fistula into the rectum to enter contrast substance into the intestine. At rest, the anal canal is contracted around the catheter. (b). During a follow-up examination, an attempt to defecate resulted in a wide opening of the anal canal. The distance between the marker in the anal dimple and the wall of the open anal canal is 4 mm. It is equal to the thickness of the skin and subcutaneous tissue. (c). During the administration of barium through the endotracheal tube the relaxation of the IAS occurred, allowing barium to enter the upper part of the anal canal, in front of the rectal tube. This was accompanied by a drop in rectal pressure, which was measured by a balloon connected to a pressure gauge [12]. At this moment, the posterior wall of the anal canal is pressed against the rectal tube by the contraction of the PRM, which together with external anal sphincter closes the anal canal.
Thus, in X-ray examinations of patients with visible fistulas, a functioning anal canal was always observed. It differed from a normal anal canal only by the absence of a distal section 2-4 mm in length, which is typically surrounded by the subcutaneous portion of the EAS. The anal canal is opened through a narrow, rigid fistula located in front of the anal dimple on the perineum or in the vestibule. The presence of a normally functioning anal canal is further confirmed by manometric studies. Both the basal anal pressure, and the rectoanal inhibitory reflex were consistent with a normal anal canal function [12,13].
In the modern literature, starting with the publication of Peña [15], the distal part of the intestine is called the rectal pouch or fistula, which is removed during all pull-through operations, including posterior sagittal anorectoplasty (PSARP). The theoretical basis for this misconception is the absence or marked reduction of nerve ganglia in the distal part of the intestine, compared to the rectum in healthy individuals. These authors called the anal canal a rectal sac and compared the anal canal with the rectum [16,17]. However, the anal canal, unlike other parts of the intestinal tube, does not have an intermuscular plexus [18]. Uemura et al. again after Duhamel, Alamowich, Gubler and Roujeau (1966) proved that: - “Epithelial and ganglionic distribution was similar in the distal rectal end of ARMs and in a normal anal canal” [19].
All the above scientific studies of patients with visible fistulas indicate that the distal part of the intestine, erroneously called the rectal pouch or fistula, is a normally functioning anal canal. The rigid and narrow channel between the anal canal and the anteriorly displaced opening is in the subcutaneous tissue and skin and has a length from 2 mm in newborns to 4 mm in infants. These data confirm the embryological studies of Nievelstein et al, that the abnormal communications, usually called fistulae, should be regarded as ectopic anal orifices [8].
- ARM with long anopenile fistula.
Craniocaudal penetration of IAS along the natural path causes the formation of a normal anal canal. However, the displacement of IAS beyond the limits of this path leads to the formation of a narrow rigid fistula. This channel can be very short if IAS penetrates through the subcutaneous tissue and skin inside the subcutaneous portion of the EAS, which leads to a congenital stenosis of the anus [20]. But this fistula can be long when IAS is created by a long narrow rigid canal in the subcutaneous tissue until it penetrates outward. This is how fistula exiting on the penile skin (Figure 2 a,b) [21] or rectopenile fistula (Figure 2c) [22].
.png)
Figure 2(a). Sfoungaris et al presented the case of a male neonate with imperforate anus and a fistula exiting on the penile skin. "Colostogram and urethrography. Course of recto-penoscrotal fistula (arrows) and urethra (arrowheads). R: rectum, B: urinary bladder [21]. (b, c) Yang et al described rectopenile fistula [22].
I drew the pubococcygeal line (red). In both cases, an open anal canal is visible below the pubococcygeal line. In Figure 2a, the anal canal is mistakenly labeled as the rectum. A long, narrow fistula extends under the skin from the already formed anal canal to the root of the scrotum. These typical cases demonstrate that when the IAS penetrates tissues beyond its natural path, it creates a narrow, rigid fistula, the length of which depends on the distance between the anal canal and the point of entry into any cavity or outward. This suggests that the IAS first reaches the subcutaneous tissue opposite the anal fossa. After forming a normal anal canal, if it does not encounter the ectodermal rudiment coming towards it, it turns forward and continues until it penetrates a cavity.
The findings described above are consistent with a recent statement by pediatric surgeons from the ARM-Net Consortium: “According to present knowledge, the ‘fistula’ in ARM represents an ectopic anal canal and should be preserved as far as possible to improve the chance for fecal continence” [23]. As this definition indicates, the authors do not limit the ectopia of the anal canal to visible fistula alone, which is confirmed by both manometric and radiological studies [24].
- ARMs Without Visible Fistula
ARMs without visible fistulas (whether without a fistula, with urethral or vaginal fistulas) differ from ARMs with visible fistulas only by higher ectopia of the anus. Stephens (1953) proposed the concept of a pubococcygeal line from the lower part of the pubic bone to the distal coccygeal vertebra. He showed that this line corresponds to the location of the puborectalis muscle (PRM) separating the rectum and anal canal [25]. Since then, it was believed that if the intestine was visible below the PRM line, then in this case there was an anal canal, and the defect was classified as a low type, and if it was at or above this line, this indicated the absence of an anal canal. Over time, all cases with visible fistulas were classified as low type, and efforts were made to preserve the anal canal. Cases with invisible fistulas were classified as high types and pull-through surgery was used for treatment. However, such a division into high and low types turned out to be insufficiently precise. For example, Ohama et al. demonstrated that the functional IAS, which exists at the rectal end even in high and intermediate anorectal malformations, should be preserved during reconstruction due to its critical role in maintaining anal continence [26]. When it became clear how the anal canal functions and we began to use provocation of high rectal pressure to open it during radiographic examination, it turned out that high types also have an anal canal (Figure 3) [27, 28]. What now is meant by a high type of ARM? Since all ARMs have an anal canal, they all belong to low types. We call ARMs high or low based on the degree of ectopy of the anus.
.png)
Figure 3. Radiologic studies in males with ARM without visible fistulas. (a). On the radiograph of a newborn 30 hours after birth, the gas reaches the caudal part of the ischium (red dot), b). In the same patient, during abdominal compression, the gas penetrated the anal canal and approached the contrast marker glued to the anal dimple. (c, d) Augmented-pressure distal colostograms: (c-X-ray) and (d-MRI). In both cases, under the high pressure, the anal canal (caudal P-C line – red) opened, and its caudal wall approached the anal dimple. (e). Scheme of anal ectopy variants at high pressure in the rectum. The anal canal is wide open: red indicates the normal position of the anus (congenital anal stenosis); yellow - perineal fistula; green - bulbar fistula; blue - prostatic fistula. (f). Scheme at rest, the anal canal is in a contracted state.
Although the site of IAS penetration in urethral fistulas is significantly higher than in cases with visible fistulas, by the time of displacement, the anal canal is already formed, and its blind ending is located 2-4 mm from the anal dimple. A fistula is the short channel in the wall of the organ through which the IAS penetrates the organ. Its length is equal to the thickness of that wall of the organ through which it penetrates. Since ARMs with urethral fistulas, as well as those without fistula, have a normally formed anal canal, they should be considered low types. Kraus et al. confirm these observations. They claim: - «It is extremely important in this regard to understand that the lowest part of the rectum is usually collapsed due to the muscle tone of the funnel-like striated muscle mechanism that surrounds the rectum in 90% of cases…” [29]. However, it is well known from anatomy that there are no muscles around the rectum. The muscles that compress the intestine and prevent the leakage of intestinal contents are located around the anal canal. Since the authors do not cite any specific studies, the 90% figure should be interpreted with caution. From the above data, it follows that the IAS is involved in the formation of the anal canal until it reaches the subcutaneous tissue. It can penetrate outward through the ring of the subcutaneous portion of the EAS. Any such penetration is almost always accompanied by the formation of stenosis at the penetration site, leading to congenital anal stenosis. More often, the IAS moves anteriorly and upward, each time leaving behind a functioning anal canal.
In females without visible fistulas, the only thing that is in the way of the ectopy of the anus is the vagina, so from an embryological point of view, only ectopia of the anus in the vagina is possible, which, as shown in the diagram proposed by Stephens, can be lower or higher [25,30] (Figure 4).
.png)
Figure 4. ARM without visible fistulas in females. (a). Scheme of ectopy of the anus in girls: 1 - vestibular, 2 - low vaginal, 3 - high vaginal. (b). In a female with a low vaginal fistula, the rectum is not dilated. The contrast agent introduced through the colostomy passes through the anal canal (caudal of pubococcygeal line) and comes out of the vagina in a wide stream. The moment of contraction of the anal canal is recorded. (c). In a female with high vaginal fistula, the contrast agent introduced through the colostomy passes through the anal canal to the high part of the vagina. The upper part of the anal canal is widely open to the level of the fistula (arrow), and the lower part is in a closed state since the pressure in the rectum is not high enough.
EMBRYOLOGY OF ARMS WITH FISTULAS, WITHOUT FISTULAS AND CONGENITAL STENOSIS OF THE ANUS FROM THE POINT OF VIEW OF PATHOLOGICAL ANATOMY AND PHYSIOLOGY
Literature review and our own research indicate that the above types of ARMs develop in the post-cloacal period because of impaired development of the ectodermal rudiment of the anal canal. The upper part of the anal canal develops normally because of the cranio-caudal movement of the IAS. Having reached the subcutaneous tissue and not encountering the ectodermal rudiment on its way, the IAS continues to create a canal, moving forward and upward until it penetrates the outside or into some cavity. Beyond its natural path, it creates a narrow and rigid fistula. If it penetrates through the subcutaneous tissue and skin inside the subcutaneous portion of the EAS, stenosis of the anus (not the anal canal) occurs, ranging in length from 2 mm in a newborn to 4 mm in an infant. In other cases, ectopia of the anus occurs to varying degrees, but the distance from the caudal wall of the anal canal to the imperforate anal pit remains within the same limits. Thus, in all cases, regardless of the degree of ectopia, there is a normally functioning anal canal. If the anal canal is in a contracted state, it is impossible to see it. It opens only when the pressure in the rectum is high. During surgery under anesthesia, the pressure in the rectum decreases, which leads to a contraction of the anal canal. Those surgeons who do not know about the existence of the anal canal and find a narrow channel, think that it is a fistula, and resect it, and in its place, they lower the rectum, which has a completely different function [12].
MODERN IDEAS ABOUT THE SO-CALLED "PERSISTENT CLOACA"
An ARM, которая now называется persistent cloaca, before Hendren’s classification was known as ARM with recto-vaginal fistula because feces were expelled from an opening in the perineum in the absence of an anus. The reason for highlighting this anomaly was the existence of two similar types of anomalies. In rare cases, the vagina had a wide lumen (see Figure 4). Sometimes a narrow, rigid channel was observed, and in some cases, a closed cavity formed in the upper part of the vagina, leading to the accumulation of a large amount of fluid (hydrocolpos). Hendren termed this second type of anomaly persistent cloaca [31]. Although the anatomical and physiological descriptions of this defect lack a scientific basis, these children are treated as though they suffer from a true cloaca [32].
Hendren did not conduct any studies to assess the function of the urinary system and lacked a clear understanding of the pathological anatomy of the defect. For example, he believed that hydrocolpos resulted from vaginal distension by urine. He wrote: “Intermittent catheterization of the bladder and/or urine-filled vagina can often provide adequate decompression” [19]. Peña adopted the idea of persistent cloaca. However, neither he nor his colleagues conducted studies on the state of the urinary system. In 1997, Peña proposed the total urogenital mobilization (TUM) operation to repair cloaca. During the presentation of his article, Hendren asked, “Do you think the external urethral sphincter is of any importance in these patients? And if it is, do you think this mobilization risks any injury to the external sphincter?" Peña responded, "My experience in managing cloaca is that girls who suffer from urinary incontinence do so not because of a lack of urinary sphincter but rather due to the lack of bladder contractility" [23]. Of the numerous articles by Alberto Peña, I have not found a single scientific study. All his innovations are the result of his "experience". Even though experience is not scientific evidence, he and his followers do not recognize scientific data that contradicts Peña's experience. Below is an analysis of the situation with "persistent cloaca".
- The description of the anatomy and physiology of the “persistent cloaca” contradicts known patterns of embryology
Currently, following Hendren and Peña, it is believed that the urethra, vagina, and rectum are connected during the embryonic period into a single canal called the cloaca [33]. However, the presence of the urethra and vagina indicates that patients have successfully passed the cloacal stage and therefore have a urethra, vagina, and must also have an anal canal. In the post-cloacal period three separate canals form within the perineal tissues, with their walls adjacent to each other. There is no evidence to suggest that these three channels can fuse into a single channel, especially not in one specific location. This assumption contradicts common sense. Furthermore, in a study by Runck et al., the molecular pathologies underlying cloacal malformations were examined. Their findings using Shh knockout mice showed that “...the epithelium from the common channel has matured and does not exhibit the same characteristics as cloacal epithelium before septation...” [34]. This means that the epithelial samples taken by pediatric surgeons from the so-called "common canal" were more mature than what would be expected in an undivided cloaca. From an embryological perspective, therefore, the "persistent cloaca" has no relation to the cloaca. By calling the anal canal the rectum (rectal pouch or fistula), these authors, as shown above, justify its extirpation during PSARP.
- The generally accepted description of radiological studies of the persistent cloaca does not correspond to the true anatomy
Radiological diagnostics are used to determine the confluence site of the urethra, vagina, and rectum. The surgical treatment method depends on the fusion level [35,36]. Figure 5 shows samples of MRI studies.
.png)
Figure 5. Radiographic anatomy of persistent cloaca. (a) MRI study from the article by Wood et al. [35], with the caption "Short common channel cloaca with adequate urethra." The authors suggest that, in the angle between the yellow and green lines, the urethra merges with the vagina to form a common channel. In the copy of the same image (b) I have shown the presence of two channels: between the yellow lines, you can see the continuation of the urethra up to the perineum, and next to it, the blue lines indicate the narrow vaginal canal. Between them, a dark dividing line can be observed, representing the fusion of the walls of the urethra and vagina. The upper part of the vagina (V) is dilated (hydrocolpos). The red arrow points to a rectum above the anal canal. The white arrow indicates at the site of the anal ectopy into the vagina. The contracted short anal canal is visible between the red and white arrows. The site of IAS penetration into the vagina divides the vagina into an upper, widened part and a lower, narrow part. However, the urethra is of normal length and extends to the perineum. (c, d, e) From the article by AbouZeid with the caption "MRI stratification of cloaca based on the level of the urogenital confluence (white arrow)" [36]. I have indicated the urethra with yellow lines. (c) The urethra and narrow vagina run parallel up to the perineum, where the clitoris is located. There is no fusion of the urethra and vagina. (d) The white arrow does not indicate the site of confluence but rather the site of vaginal obstruction, above which hydrocolpos is observed. (e) The white arrow shows the site of vaginal obstruction, above which hydrocolpos is observed. The yellow line shows a long and normally positioned urethra. Gas is visible in the rectum, which is also present in the upper part of the anal canal (a) (arrow).
The interpretation of these cases by the authors of the articles was influenced by the erroneous concept of the possibility of already formed canals merging into one common channel. Because of this misconception, the authors overlooked the actual anatomical features, mistaking the site of vaginal obstruction for the site of merging. Consequently, obvious signs of a normal urethral position were ignored. In case (e), the presence of gas in the anal canal was not mentioned.
- Comparison of the results of different treatment methods for "Persistent Cloaca".
In a retrospective review by Rosen et al. of all girls with ARM treated by Peña from 1980 to 2000, only 6 out of 617 patients were found to have a true rectovaginal fistula, an incidence of 1%. In numerous cases where a vaginal fistula was diagnosed at other institutions, the authors considered it a misdiagnosis, asserting that it was a persistent cloaca [37]. To evaluate the value of a novel approach to treating children with so-called "persistent cloaca" it is important to compare the treatment results before and after the diagnosis was changed.
As shown in the systematic review by Versteegh et al., after treating a “persistent cloaca” as if it were a true cloaca, voluntary bowel movements were reported in 57% of patients, soiling in 71%, and constipation in 51%. Spontaneous voiding was reported in 46%. Additionally, 42% of patients used intermittent catheterization, and 22% had a urinary diversion [38]. First, in the treatment of vaginal fistulas before categorizing them as "persistent cloaca", there were no issues with urinary diversion. Comparisons of outcomes before and after changes in diagnosis from vaginal fistula to persistent cloaca are not described in the literature. Secondly, Kittur and Vora conducted a follow-up study involving one adolescent and eight adult female patients born with cloaca, who had undergone rectal pull-through surgery in infancy, leaving the urogenital region untouched. After full growth, the common channel was used as a vagina with introitoplasty and dilatation, or with additional surgical intervention. All patients retained an intact urogenital complex, and none experienced recurrent urinary tract infections until adolescence. All patients are now beyond adolescence, and five have married. Three reported regular sexual intercourse, and one has conceived. Of the three patients who are not married, introitoplasty was performed to allow for free menstrual flow. Only one of the nine patients reported urinary and fecal incontinence. The authors argue that there is a strong case against subjecting cloaca patients to TUM, as it has significant potential to cause urinary incontinence. Furthermore, the common channel can be used as a vagina in conjunction with introitoplasty and dilatation [39]. AbouZeid, based on the analysis of long-term results, concluded that in some cases of cloaca, it might be better from both functional and cosmetic perspectives to perform only introitoplasty while leaving the common urogenital sinus uncorrected [36].
Based on the literature review and our own research, the following was established:
- The expanded concept of the so-called “persistent cloaca” has nothing to do with the true cloaca. This pathology develops in the post-cloacal period, when the urethra, vagina and anal canal have already emerged. The only hole in the crotch is displaced forward from the usual location of the anal dimple.
- There is no evidence that these patients have congenital pathology of the urinary and anorectal functions. Preservation of the urinary system without intervention leads to significantly better functional results than scientifically unsubstantiated correction.
- It is reliably known that the vagina is narrow and has rigid walls. Sometimes there is obstruction of the vaginal lumen, because of which fluid accumulates in the upper part of the vagina.
I propose a hypothesis of the embryonic development of the so-called “persistent cloaca”, which is free from the above-described contradictions.
THE HYPOTHESIS OF EMBRYONIC DEVELOPMENT OF “PERSISTENT CLOACA”
The pathology develops in the post-cloacal period, when the cranio-caudal advancement of the IAS reaches the subcutaneous tissue, but without encountering the ectodermal rudiment of the anal canal on its way, it begins to shift forward and upward. The IAS penetrates the vagina and can create two types of vaginal fistulas. (a). If a cavity has already formed in the vagina by this time, a typical ARM with a short narrow fistula is formed, the length of which is equal to the thickness of the vaginal wall. In such cases, the vagina has a wide cavity and elastic walls (see Figure 4). Depending on the place of penetration, the fistula can be located lower or higher. (b). If at the time of penetration of the IAS into the vagina the cavity has not yet formed, then the advancement of the IAS creates a narrow and rigid canal, the same as in boys with rectopenile fistula (see Figure 2). In both cases, by the time the IAS penetrates the vagina, the urethra and anal canal are already normally formed. Figure 6 shows the anatomical diagrams of the “persistent cloaca” anatomy [33,25].
.png)
Figure 6. (а). The diagram of the “persistent cloaca” from the article by Levitt and Peña [33]. Caudal to the pubococcygeal line I have drawn (in red) are the urethra, vagina, and anal canal, which the authors call the rectum. As shown above, the urethra does not merge with the vagina but is located next to it. The upper part of the vagina above the ectopia of the anus is dilated (hydrocolpos). (b-c) On the diagram of fistula locations in girls, proposed by Stephens (1-vestibular; 2-vaginal low; 3-vaginal high), I have drawn a channel in red, which is created by the IAS in the vagina in cases where an internal cavity has not yet developed. The blue oval shows the location of the hydrocolpos above the site of the IAS ectopy, where the release of fluid from the upper part of the vagina is blocked. (b). Low vaginal ectopy. (c). High vaginal ectopy with narrow and rigid vagina.
DIAGNOSIS AND TREATMENT
The purpose of diagnostics in newborns is to detect the anal canal. Fluoroscopy should be performed 30-48 hours after birth with the patient in a horizontal position on her side. By this time, enough gas and meconium should accumulate in the rectum to create a threshold pressure in the rectum for opening the anal canal. This is manifested by gas penetration into the anal canal and its distal wall approaching the marker glued to the anal pit (see Figure 3). In such cases, three options are possible. (1). If the fistula is poorly passable or blocked by meconium, then during abdominal compression between the operator's palms, gas penetrates the anal canal and does not disappear, despite compression. This situation allows perforation of the perineum and insertion of a tube into the anal canal, which will lead to complete preservation of the anal canal [40]. (2). If the fistula functions and gas enter the anal canal during abdominal compression but quickly passes through the fistula to the outside, this allows confirmation of the presence of the anal canal but does not allow to do perforation of the perineum. In this case, a colostomy must be performed. (3) If the fistula is easily patent, then it is not possible to create pressure in the rectum to open the anal canal, so a colostomy must be performed. Definitive anorectal correction is advisable to perform at about one year of age using the anal canal visualization method described by Pakarinen and Rintala [41] (Figure 7a,b). After the endoscope passes the entire anal canal and stops 2-4 mm opposite the anal fossa, it is possible to perforate the tissue with an exit in the ring of the subcutaneous part of the EAS (Figure 7c) and then pass a 1 cm diameter tracheostomy tube into the rectum. A balloon inflated in the rectum will hold the tube in the rectum for 2 weeks, ensuring evacuation of the rectum. By this time, the diastasis that has developed between the IAS and the skin will close without the development of scar tissue. Thus, the anatomy and function of the anal canal are completely preserved [42,43].
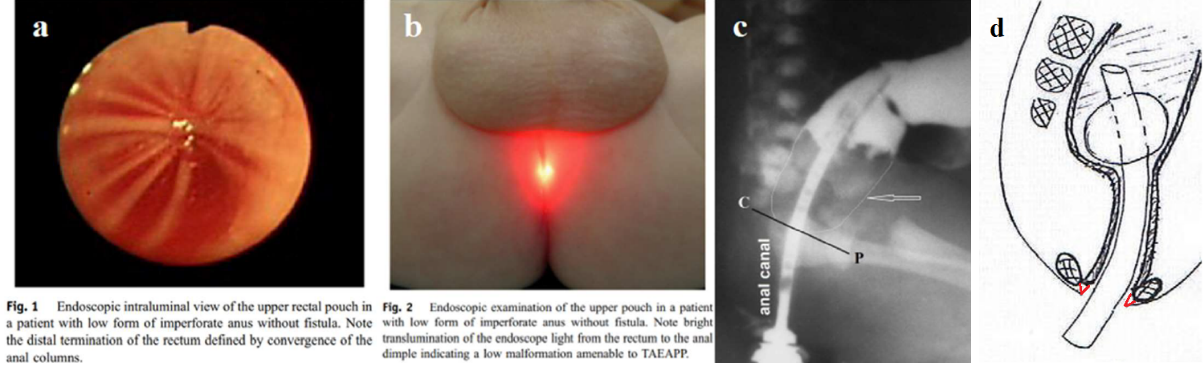
Figure 7. Method of preserving the anal canal by perforating the perineum from the anal canal using an endoscope. (a, b). From the article by Pakarinen and Rintala [41], the caudal part of the anal canal is visible, where the anal columns converge. Bright translumination of endoscope light indicates that the endoscope is near the anal pit. (c). After perforating the perineum, a catheter is inserted into the rectum, through which a contrast agent is injected. In the rectum, above the pubococcygeal line, there is meconium (arrow). (d). A tracheostomy tube is inserted into the rectum through the guidewire. After 2 weeks, the diastasis between the IAS and the skin (red) closes.
After this operation, continence, defecation, and the function of the urinary system do not differ from the norm since the muscles and innervation of the perineum are not damaged. All interventions that are proposed to correct the supposedly true cloaca destroy what naturally functions normally. In the presence of hydrocolpos, timely drainage of the upper part of the vagina is necessary. Questions about dilatation of a narrow vagina or introitoplasty, as well as the time of their implementation, should be decided and carried out by gynecologists.
CONCLUSION
All ARMs, except for the true cloaca, arise in the post-cloacal period because of impaired development of the ectodermal portion of the anal canal. By this time, the IAS, shifting in the cranio-caudal direction, forms the anal canal. Not having encountered the ectodermal rudiment on its way, the IAS continues to look for an exit, moving forward and upward. In this way, it creates an ectopia on the perineum, vestibule, urethra, and vagina. The hypothesis of the development of two types of ectopy of the anus in the vagina is substantiated. If at the time of penetration of the anus in the vagina there is already a cavity, then a typical ectopy of the vagina with wide cavity and elastic walls occurs. These patients usually have a normal bladder, urethra, and a functioning anal canal. If penetration of the anus into the vagina occurred before the occurrence of cavity in it, then the IAS creates a narrow and rigid channel in the vagina, reaching the perineum near the opening of the urethra. By this time, the urethra and anal canal are already normally formed. This pathology is mistakenly called persistent cloaca and patients are operated on as if they had a true cloaca, i.e., the urethra, vagina and anal canal were absent. Poor outcomes are the result of unnecessary surgeries. In accordance with this hypothesis, diagnostic and treatment methods are proposed.
HIGHLIGHTS
- Most ARMs arise because of disruption of the formation of the ectodermal portion of the anal canal.
- By this time, they already have a functioning anal canal.
- The internal anal sphincter, which forms the anal canal, not having encountered the ectodermal rudiment on its way, shifts forward and upward and penetrates outward or into some organ, forming an ectopia of the anus (perineal, vestibular, urethral, vaginal).
- The so-called persistent cloaca, unlike the true cloaca, is formed because of ectopia of the anus in the vagina, when a cavity has not yet appeared in it, resulting in the formation of a long fistula.
These patients have a normally functioning bladder, urethra and anal canal, which must be preserved during correction to achieve the best functional result.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The author declares that there is no Conflicts of Interest.
REFERENCES
- Alamo L, Meyrat BJ, Meuwly JY, Meuli RA, Gudinchet F. (2013). Anorectal Malformations: Finding the Pathway out of the Labyrinth. Radiographics. 33(2):491-512.
- Kluth D. (2010). Embryology of anorectal malformations. Semin Pediatr Surg. 19(3):201-218.
- Anatomy and Embryology of the Colon, Rectum, and Anus José Marcio Neves Jorge and Angelita Habr-Gama. In book: The ASCRS Textbook of Colon and Rectal Surgery. pp.1-22.
- Okonkwo JE, Crocker KM. (1977). Cloacal dysgenesis. Obstet Gynecol. 50(1):97-101.
- Gupta A, Bischoff A, Peña A, et al. (2014). The great divide: septation and malformation of the cloaca, and its implications for surgeons. Pediatr Surg Int. 30(11):1089-1095.
- Zhang SW, Bai YZ, Zhang D, Zhang T, Zhang SC, Wang DJ, Wang WL. (2010). Embryonic development of the internal anal sphincter in rats with anorectal malformations. J Pediatr Surg. 45(11):2195-202.
- Nobles VP. (1985). The development of the human anal canal. Journal of Anatomy, 1984, 138, 575. Quote from the book "Coloproctology and the pelvic floor" by M.M. Henry and M. Swash. Batterworths.
- Nievelstein RA, van der Werff JF, Verbeek FJ, Valk J, Vermeij-Keers C. (1998). Normal and abnormal embryonic development of the anorectum in human embryos. Teratology. 57(2):70-78.
- Levin MD. (2024). Embryological Development of Anorectal Malformations: A Hypothesis. Qeios, CC-BY 4.0. Preprint. https://doi.org/10.32388/HIMVOF
- Levin MD, Averin VI, Degtyarev YuG. (2023). Diagnosis and Treatment of the Rectal Atresia. Novosti Khirurgii. 31(6):468-477.
- Levin MD, Mendelson G. (2024). Late diagnosis of congenital anal canal stenosis. Case report and literature analysis. Gastroenterol Hepatol Open Access. 15(4):126-129.
- Levin MD. (2013). [The pathological physiology of the anorectal defects, from the new concept to the new treatment]. Eksp Klin Gastroenterol. (11):38-48.
- Ruttenstock EM, Zani A, Huber-Zeyringer A, Höllwarth ME. (2013). Pre- and postoperative rectal manometric assessment of patients with anorectal malformations: should we preserve the fistula? Dis Colon Rectum. 56(4):499-504.
- Kyrklund K, Pakarinen MP, Taskinen S, Rintala RJ. (2015). Bowel function and lower urinary tract symptoms in males with low anorectal malformations: an update of controlled, long-term outcomes. Int J Colorectal Dis. 30(2):221-228.
- Peña A, Devries PA. (1982). Posterior sagittal anorectoplasty: important technical considerations and new applications. J Pediatr Surg. 17(6):796-811.
- Gangopadhyay AN, Upadhyaya VD, Gupta DK, Agarwal DK, Sharma SP, Arya NC. (2008). Histology of the terminal end of the distal rectal pouch and fistula region in anorectal malformations. Asian J Surg. 31(4):211-215.
- Xiao H, Huang R, Cui DX, Xiao P, Diao M, Li L. (2018). Histopathologic and immunohistochemical findings in congenital anorectal malformations. Medicine (Baltimore). 97(31):e11675.
- Duhamel B. (1969). Physio-pathology of the internal anal sphincter. Arch Dis Child. 44(235):377-381.
- Uemura K, Fukuzawa H, Morita K, et al. (2021). Epithelial and ganglionic distribution at the distal rectal end in anorectal malformations: could it play a role in anastomotic adaptation? Pediatr Surg Int. 37(2):281-286.
- Levin MD. (2024). Congenital anal stenosis (etiology, pathogenesis, diagnosis and treatment). Novosti Khirurgii. 32(1):52-60.
- Sfoungaris D, Mouravas V, Lambropoulos V, et al. (2016). Imperforate Anus with Fistula Exiting at the Penile Skin. J Clin Diagn Res. 10(3):PD01-2.
- Yang G, Wang Y, Jiang X. (2016). Imperforate anus with rectopenile fistula: a case report and systematic review of the literature. BMC Pediatr. 16:65.
- Amerstorfer EE, Schmiedeke E, Samuk I, Sloots CEJ, van Rooij IALM, Jenetzky E, et al. (2022). Clinical Differentiation between a Normal Anus, Anterior Anus, Congenital Anal Stenosis, and Perineal Fistula: Definitions and Consequences-The ARM-Net Consortium Consensus. Children (Basel). 9(6):831.
- Levin MD, Averin VI, Degtyarev YG. (2022). Pathological physiology of anorectal malformations (ARM) without visible fistulas. Review. Novosti Chirurgii (Belarus). 30(3):105-112.
- Stephens FD. (1953). Imperforate rectum; a new surgical technique. Med J Aust. 1(6):202-203.
- Ohama K, Asano S, Nanbu K, Kajimoto T. (1990). The internal anal sphincter in anorectal malformation. Z Kinderchir. 45(3):167-177.
- Levin MD. (2021). Anatomy and physiology of anorectum: the hypothesis of fecal retention, and defecation. Pelviperineology. 40(1):50-57.
- Levin MD. (2023). Pathological physiology of the anorectal malformations without visible fistula. A short review. Pelviperineology. 42(2):74-79.
- Kraus SJ, Levitt MA, Peña A. (2018). Augmented-pressure distal colostogram: the most important diagnostic tool for planning definitive surgical repair of anorectal malformations in boys. Pediatr Radiol. 48(2):258-269.
- Swain VA, Tucker SM. (1962). The results of operation in 46 cases of malformation of the anus and rectum. Gut. 3(3):245-251.
- Hendren WH. (1980). Urogenital sinus and anorectal malformation: experience with 22 cases. J Pediatr Surg. 15:628-641.
- Hendren WH. (1986). Repair of cloacal anomalies: current techniques. J Pediatr Surg. 21(12):1159-1176.
- Levitt MA, Peña A. (2007). Anorectal malformations. Orphanet J Rare Dis. 2:33.
- Runck LA, Method A, Bischoff A, Levitt M, Peña A, Collins MH, et al. (2014). Defining the molecular pathologies in cloaca malformation: similarities between mouse and human. Dis Model Mech. 7(4):483-493.
- Wood RJ, Reck-Burneo CA, Dajusta D, Ching C, Jayanthi R, Bates DG, et al. (2017). Cloaca reconstruction: a new algorithm which considers the role of urethral length in determining surgical planning. J Pediatr Surg. S0022-3468(17)30644-30649.
- AbouZeid AA. (2019). Achieving Full Anatomical Correction in Girls with cloacal anomalies: A Necessity or an Overdoing? The Journal of Genital Surgery. 8(1):1-10.
- Rosen NG, Hong AR, Soffer SZ, et al. (2002). Rectovaginal fistula: a common diagnostic error with significant consequences in girls with anorectal malformations. J Pediatr Surg. 37(7):961-965.
- Versteegh HP, van Rooij IA, Levitt MA, et al. (2013). Long-term follow-up of functional outcome in patients with a cloacal malformation: a systematic review. J Pediatr Surg. 48(11):2343-2350.
- Kittur DH, Vora RM. (2017). Persistent Cloaca: A Long-term Follow-up Study. J Indian Assoc Pediatr Surg. 22(2):126-127.
- Levin MD. (2023). Pathological physiology of the anorectal malformations without visible fistula. A short review. Pelviperineology. 42(2):74-79.
- Pakarinen MP, Rintala RJ. (2010). Management and outcome of low anorectal malformations. Pediatr Surg Int. 26(11):1057-1063.
- Levin MD. (2013). [The pathological physiology of the anorectal defects, from the new concept to the new treatment]. Eksp Klin Gastroenterol. (11):38-48.
- Levin MD. (2023). Theoretical Basis of New Surgical Tactics for Anorectal Defects without Visible Fistulas. Novosti Khirurgii. 31(5):397-404.