Previous Issues Volume 4, Issue 1 - 2019
Dyscondrosteosis of Léri-Weill: Presentation of an Affected Family
Elayne Esther Santana Hernandez
Assistant Professor, Comprehensive General Medicine and Clinical Genetics, Provincial Center of Medical Genetics, Cuba.
Received Date: May 22, 2019 Published Date: Jun 28, 2019
Corresponding Author: Elayne Esther Santana Hernandez* Assistant Professor, Comprehensive Child Care, Comprehensive General Medicine and Clinical Genetics, Provincial Center of Medical Genetics, Holguin, Cuba.
Copyright © 2019 Hernandez EES
Citation: Hernandez EES. (2019). Dyscondrosteosis of Léri-Weill: Presentation of an Affected Family. Mathews J Pediatr. 4(1): 17.
ABSTRACT
Background: Léri-Weil dyschondrosteosis, bone dysplasia of genetic origin that affects the mesomelic region with shortening of the extremities, causing short stature with short limbs with deformity of madelung. This disease shows an autosomal dominant pattern of inheritance with high penetrance.
Presentation: a family with sick in three generations with Madelung deformity of both dolls and short stature of mesomelic origin.
Conclusion: The physical and radiological examination essential to reach the clinical diagnosis. The clinical method is of great value to define this genetic disease and to provide adequate genetic counseling to this family.DeCS: BONE DISPLSIA, MESOMÉLICO SHORTENING, LOW SIZE GENETIC ORIGIN
Keywords: Dyschondrosteosis; Léri-Weill’s disease; Deformation of madelung; Mesomelic dwarfism.
INTRODUCTION In 1878, Otto W. Madelung described a painful abnormality of the wrists that usually began in adolescence. Later, in 1929, André Léri and Jean A Weill reported a case of dwarfism that presented the deformation of the wrists described above by Madelung characterizing it as a symmetric congenital condition of bone development which they called discondrosteosis [1,2].
Currently, it is considered that Leri-Weill dyschondrosteosis (DLW) is a hereditary syndrome with autosomal dominant character with a phenotype characterized by short stature of the patients, mesomelic shortening of the extremities and Madelung deformation of the carpus, being able to find cubitus. valgus, short neck. It predominates in women in the order of 4:1 and the prevalence is estimated at 1/2000 live births [3-5].
Leri-Weill dyschondrosteosis (DLW) is a skeletal dysplasia marked by a disproportionately low stature and the characteristic wrist deformation of Madelung. The deformation of Madelung can only be detected at puberty. The deformation of the wrist is bilateral and is characterized by shortening and inclination of the radius and ulna, which leads to a dorsal dislocation of the distal ulna and limits mobility of the elbow and wrist. The disease has variable expressivity, but the clinical manifestations are generally more severe in women. Male patients show athletic habit due to muscle hypertrophy, without any underlying muscle disorder. The intelligence is normal [6,7].
70% of the cases, is produced by a haploinsufficiency of the SHOX gene, mapped on the pseudoautosomal region 1 (PAR1) of the sex chromosomes (Xp22.33 and Yp11.32). The SHOX gene encodes a transcription factor regulating the growth of the middle segment of the extremities (radius and tibia) and the first two pharyngeal arches. The location in this region also implies the possibility that SHOX haploinsufficiency forms part of the contiguous genes syndrome of the distal short arm of the X chromosome [8-10].
Being considered of great value the clinical and radiological study to be able to carry out an adequate genetic counseling, for the representative of this family with several affected is that it was decided to publish the case.
CASE PRESENTATION
We present a family with three generations of individuals with short size shortening of the limbs and deformity of Madelung, here the family tree of this family is represented as shown in Figure 1.
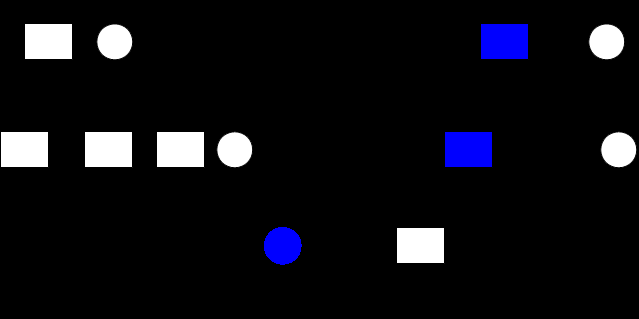
Figure 1: Family tree of the affected family.
In the first generation the first male individual affected with a height of 145 cm and the deformity of Madelung had two offspring an affected male and a healthy female, this son also had two offspring where the female was affected.
14-year-old adolescent with size 135 cm, short stature due to shortening of mesomelic limbs that is symmetrical with Madelung deformity and subluxation of the elbow joint of the forearms that prevents complete extension as seen in Figure 2.


.bmp)
Figure 2: Characteristics of forearm deformities.
The three affected parties are asked to give informed consent to perform a physical and radiological examination to arrive at the clinical diagnosis and take photos to publish in scientific journals which they accept.
After reviewing the updated literature and discussing the radiological studies, we arrive at the clinical diagnosis, a bone dysplasia of the Leri-Weill dyschondrosteosis type. Genetic counseling is provided to the family and the high risk of transmission from each affected to their descendants is explained by 50%.
DISCUSSION
Leri-Weill discondrosteosis (LWD) to mild forms of dyschondrosteosis. The classic form is short stature, mesomelia and Madelung type deformity. Mesomelia is the most frequent clinical manifestation, in which the middle part of a limb is short in relation to the proximal portion. The deformity of Madelung includes the abnormal alignment of the radius, ulna, and carpal bones of the wrist, which usually develops from mid to late childhood; being more common and severe in women [1-3].
Radiological signs of Madelung’s deformity were proposed 1939 by radiographs of the forearms and wrists with the following signs: deformation of the proximal carpus, widening of the distal radioulnar joint, early fusion of the ulnar face of the radial epiphysis, short radius and bent, ulnar deviation of the articular surface of the radius, triangular deformation of the radial epiphysis, whose external edge is strikingly thicker than the internal one, dorsal subluxation of the ulna [4,5].
The Madelung deformity of the distal radius is the result of premature closure of the volar medial aspect of the distal radial fissure, resulting in an increased inclination of the radial articular surface, triangulation of the carpus with proximal migration of the lunate and dorsal displacement of the distal ulna. . The deformity is particularly frequent in Leri- Weill dyschondrosteosis, but it can also occur in isolation [5-7].
Bone dysplasias or congenital anomalies that occur with short stature encompass a wide range of syndromes and diseases. The differential diagnosis should include the other haploinsufficiencies related to SHOX and other diseases such as Turner syndrome and distal monosomy Xp, chondrodysplasia punctata, ichthyosis linked to theX-chromosome, Kallmann syndrome. It includes trauma, infections, multiple exostosis, Ollier’s disease, multiple epiphyseal dysplasia, chondroectodermal dysplasia (Ellis-van Creveld disease), mesomelic dwarfism (Langer’s disease) and mucopolysaccharidosis [7,8].
Haploinsufficiency is caused by heterozygous mutations and deletions in SHOX, or in PAR1, due to haploinsufficiency (monoallelic deficit) of the SHOX gene in heterozygous males and females. Although in 30% the molecular cause is unknown [9-10].
The diagnosis can be suspected by the clinical and radiological findings and the clinical diagnosis can be made, confirmation of the SHOX gene deletion is made by molecular analysis, the analysis of microsatellite markers, FISH or MLPA for the PAR1 deletions and high resolution fusion (HRM), dHPLC and/or DNA sequencing for point mutations, small deletions and SHOX insertions) [10]. Due to the characteristic of the phenotype and the radiological studies of the three affected in this family with the same deformities of the mesomelic region, the clinical diagnosis was Lars Weill dyschondrosteosis.
CONCLUSION
The physical and radiological examination essential to reach the clinical diagnosis. The clinical method is of great value to define this genetic disease and to provide adequate genetic counseling to this family.
Recommendations
We recommend performing a thorough physical examination to all possible relatives even without referring any symptoms because the expression is variable and may be more affected in the same family by the autosomal dominant pattern of inheritance. Also provide genetic counseling to affected families so they know the risk of recurrence of this disease.
REFERENCES
- Ali S, Kaplan S, Kaufman T, Fenerty S, et al. (2015). Madelung deformity and Madelung-type deformities: A review of the clinical and radiological characteristics. Pediatr Radiol. 45(12): 1856-1863.
- Rodríguez FA, Unanue N, Hernandez MI, Basaure J, et al. (2013). Clinical and molecular characterization of Chilean patients with Léri-Weill dyschondrosteosis. J Pediatr Endocrinol Metab. 26(7-8): 729-734.
- Hisado-Oliva A, Garre-Vázquez AI, Santaolalla-Caballero F, Belinchón A, et al. (2015). Heterozygous NPR2 mutations cause disproportionate short stature, similar to Léri-Weill Dyschondrosteosis. J Clin Endocrinol Metab.100(8): E1133-1142.
- Abasq-Thomas C, Schmitt S, Brenaut E, Metz C, et al. (2016). A case of syndromic x-linked ichthyosis with léri-weill dyschondrosteosis. Acta Derm Venereol. 23:96(6): 814-815.
- Choi WB, Seo SH, Yoo WH, Kim SY, et al. (2015). A Leri-Weill dyschondrosteosis patient confirmed by mutation analysis of SHOX gene. Ann Pediatr Endocrinol Metab. 20(3): 162-165.
- Kozin SH and Zlotolow DA. (2015). Madelung deformity. J Hand Surg Am. 40(10): 2090-2098.
- Huguet S, Leheup B, Aslan M, Muller F, et al. (2014). Radiological and clinical analysis of Madelung’s deformity in children. Orthop Traumatol Surg Res. 100(6 Suppl):S349-352.
- Alexandrou A, Papaevripidou I, Tsangaras K, Alexandrou I, et al. (2016). Identification of a novel 15.5 kb SHOX deletion associated with marked intrafamilial phenotypic variability and analysis of its molecular origin. J Genet.95(4): 839-845.
- Shima H, Tanaka T, Kamimaki T, Dateki S, et al. (2016). Systematic molecular analyses of SHOX in Japanese patients with idiopathic short stature and Leri-Weill dyschondrosteosis. J Hum Genet. 61(7): 585-591.
- Bunyan DJ, Baffico M, Capone L, Vannelli S, et al. (2016). Duplications upstream and downstream of SHOX identified as novel causes of Leri-Weill dyschondrosteosis or idiopathic short stature. Am J Med Genet A. 170A(4): 949-957.