Information Links
Related Conferences
Previous Issues Volume 6, Issue 2 - 2022
Does Injectable Platelet-Rich Fibrin (i-PRF) Have a Positive Effect on New Bone Formation in the Rapid Palatal Expander?
Antônio Soares Lucas Tunes*
Department of Dentistry, Portugal
Received Date: June 24, 2022
Published Date: July 21, 2022
*Corresponding Author: Antônio Soares Lucas Tunes, Department of Dentistry, Portugal. Tel: 000423-26523-70; E-mail: [email protected]
Citation: Tunes ASL. (2022). Does Injectable Platelet-Rich Fibrin (i-PRF) Have a Positive Effect on New Bone Formation in the Rapid Palatal Expander? Mathews J Dentistry. 6(2):30.
Copyright: Tunes ASL. © (2022).
ABSTRACT
Objective: The goal of this study was to see if injecting i-PRF locally may alter bone growth in surgically expanded mid palatal sutures using MSE2. Materials and methods: 18 adult male pigs were randomly divided into three groups: group I (control), in which expansion with MSE2 was done without corticotomy and i-PRF. Group II, in which the expansion was done with mid palatal corticotomy but without i-PRF injection. Group III, in which the expansion was done with mid palatal corticotomy and injection with 2 ml of i-PRF. Each group consisted of 6 pigs which were subdivided into 3 pigs, sacrificed after 15 day and another 3 pigs sacrificed after 45 day. The number of osteoblasts, blood vessels, and the percentage of new bone formation in each group were statistically analyzed using the Sigma plot program, mean and standard error, ANOVA, and Duncan. P values of less than 0.05 were deemed significant. Results: I-PRF group showed significant increase in the amount of new bone in the mid palatal suture after expansion at 15 and 45 day compared with other 2 groups which were indicated by highest percentages of new bone formation (30.30 % of 15 day and 74.55 % at 45 day) if compared to control group which were (7.72 % at 15 day and 23.30 % at 45 day). The corticotomy groups were between, 15.33% and 47.84% respectively. Conclusion: Outcomes indicated that i-PRF can enhance the formation of new bone in the surgically expanded mid-palatal suture.
Keywords: Bone formation, injectable platelet-rich fibrin (i-PRF), MSE2.
INTRODUCTION
Transverse maxillary insufficiency is one of the most common orthodontic problems in both children and adults. This problem leads to an ugly smile and improper occlusion, crowding, stenosis, and buccal segment crossbite [1,2]. Currently, the prevalence of maxillary transverse shortage has been found to range between 8% and 24% in mixed and deciduous dentitions and less than 10% in adults [3].
Treatment of the tapered maxillary arch requires the application of orthopedic forces or surgical intervention for expansion [4]. Rapid palatal expansion (RPE) with tooth-born expanders has been used for the treatment of maxillary transverse deficiency [5]. Bone dehiscenceor fenestration, root resorption, gingival recession, buccal tilting of posterior teeth, and recurrence are all common RPE side effects [6]. Various varieties of bone-borne RPE have been created to lessen the negative effects of toothborne RPE while also increasing skeletal extension [7]. Patients with minimal or no residual growth are sometimes unwilling to undergo surgery, resulting in attempts to rectify these deficits without surgery, which led to the development of MARPE [4].
The MARPE appliance by Dr. Won Moon, considered a type of the RPE appliance and has developed for correction of transverse malocclusion, it has proved to be a viable and efficient nonsurgical option for young adults [7]. To achieve skeletal changes with MARPE, the force must be sufficient to overcome areas of resistance in the midface region, such as the mid-palatal suture (the first to be disrupted), pterygoid junctions, zygomatic buttresses, and piriform aperture pillars. Force is applied directly into the center of resistance of the maxilla by micro-implants, rather than the tooth, as is the case with conventional tooth palatal expanders. As a result of this force, buccal tipping of the tooth is reduced, and a more parallel suture opening is obtained [8].
Recently, Cortico-punctures or micro-osteoperforations are two minimally invasive surgical treatments linked with MARPE that have been introduced by doctors, to improve the rate of tooth movement and reduce iatrogenic damage produced by the long-term wear of fixed appliances [9,10]. Cortico-puncture was introduced in clinical practice as a surgical procedure to reduce the length of orthodontic treatment It eliminates the cortical bone that resists orthodontic force while maintaining blood circulation and bone tissue continuity to prevent necrosis and allow tooth movement [11].
Promoting new bone formation and mineralization in the mid-palatal suture after RME will be important to resist the retractive force produced by surrounding tissue and maintain the stability of the maxilla structure, which shortens the retention period after expansion, and prevent relapse of the arch width [12]. The use of platelets has increased in recent years. Platelets, which contain growth factors, play major roles in cell migration, proliferation, differentiation, and angiogenesis and are associated with the tissue regeneration process. Autologous platelet concentrates are produced by the centrifugation of blood at different speeds and the use or non-use of thrombin and anticoagulant. A fibrin clot is formed as a result of these processing protocols, whichcontain platelets and leukocytes [13]. The use of external chemicals and activation factors may increase the contamination risk that makes the use of platelet-rich plasma in clinical routine an elaborate procedure. Platelet concentrates were further developed, leading to the creation of platelet-rich fibrin (PRF), a wholly autologous system. PRF is obtained through one-step centrifugation without any anticoagulants. PRF includes a high number of leukocytes, in addition to fibrin, platelets, and plasma proteins. It is possible to generate either a solid or a liquid PRF without anticoagulants depending on the blood collection tube and the centrifugation protocol [14].
Recent research provided a new protocol for a liquid type of PRF called injectable PRF (i-PRF). Blood in a plastic tube without anticoagulant is centrifuged at 700 rpm (50 g) for 2 minutes to obtain this injectable version of PRF. Plastic tubes used in this protocol do not activate the coagulation process, since they possess hydrophobic surface. So, this process permits blood components to be separated in just a few minutes of centrifugation., leaving the orange layer (plasma, clotting factors, and platelets) at the top of the tube, which is easily aspirated and applied as an injectable form [15]. Because no investigation of the effect of local application of i-PRF on bone regeneration of the surgically extended midpalatal suture has been found to date, this study will be a significant step forward in the orthodontic field, with due regard to all critical work done previously.
MATERIALS AND METHODS
Animals and Groups Eighteen skeletally mature male pigs, 1.5-3 years and weighing 13-22 kg were used, pigs were clinically healthy as determined by physical examination, normal haemogram, and clinical chemical profiles, the pigs were housed separately in a controlled environment in animal house in a 12-h light / dark environment at the same conditions of humidity, temperature, and ventilation, and fed a home-made diet containing chicken and rice twice a day with sufficient tap of water all the period of study, animal care was done with the aid of suitably qualified veterinarian. After a two-week adaption period, the study’s experimental segment began. Experimental protocols were approved by the guidelines of the Institutional Animal Care unit of the College of Veterinary Medicine at Federal University of Minas Gerais in accordance with the ethical approval of Research of Ethics Committee of the Faculty of Dentistry, Federal University of Minas Gerais, on 20\52020.
The sample was randomly divided into 3 main groups. Group I (control group) in which expansion was done without corticotomy and i-PRF injection. Group II, in which the expansion was done with mid palatal corticotomy but without i-PRF injection. Group III, in which the expansion was done with mid palatal corticotomy and i-PRF injection. Each group consisted of 6 pigs which are subdivided into 2 subgroups (3 pigs) which were sacrificed after 15 and 45 day.
MARPE appliance
Dr. Won Moon, UCLA School of Dentistry (Biomaterials Korea, INK) invented the MSE2 screw expander, which is a variant of the Micro-implant Assisted Rapid Palatal Expander (MARPE) and was released to the market in 2010, it uses 4 titanium alloy TADs for fixation to the palate and a wrench for activation. It is stabilized by four legs that adhere to two molar bands (Dentarum, Germany). A screw expander with a diameter of 10 mm, four mini-implants with a width of 1.8 mm and a length of 11 mm was employed. Anesthesia was induced by injecting a mixture of 10% Ketamine hydrochloride (10mg/ kg) (Nederhorst den Berg, Holland) and 2% Xylazine (3mg/ kg) into the thigh muscle (Venray, Holland). Perforated special tray was previously fabricated of cold cure acrylic (New Stetic S.A., Colombia) was used, impression was taken by rubber base impression material (Dentplus, E.E.C.) and powered with stone [Figure1], After mesial and distal disking of the teeth from the cast, stainless steel bands (Dentaurum, Germany) were created on the upper right and left 1st molars., MSE2 placed on the cast leaving 1mm clearance between the screw and the cast, the holding arms were soldered to the bands with 3-4 mm clearance from the cast, The appliance was finished and polished by a polishing machine after soldering to be ready for insertion. [Figure1]. On the day of insertion of appliance the dog was anesthetize, disking of the mesial and distal sides of upper 1st molars by disking bur to occupy the bands and the MSE2 placed on the palate with bands cemented on the 1st molars using glass ionomer cement (Medifil, Germany) and the 4 mini-screws were placed in the miniscrew holes of the expander and screwed with manual screwdriver diagonally, one miniscrew at each time [Figure2]. Dr. Won Moon’s activation procedure was followed, with the expander being turned by ratchet 6 times per day (3 in the morning and 3 in the evening), with the activation continuing until the screw opened nearly 10 mm (which is the amount of opening that can be obtained from the expander) [Figure2].
Corticotomy
The surgeries were performed at the College of Veterinary Medicine’s Department of Surgery and Obstetrics. Federal University of Minas Gerais. The pigs were sedated with an intramuscular injection of ketamine (8-24 mg/ kg intramuscularly) mixed with xylazine (0.22 mg/kg intramuscularly), In the mid palatal suture region, the soft tissue of the palate was sliced backward from the canines to the 4th premolars. Another two horizontal cuts were made anteriorly and posteriorly, the mucoperiosteal flap was reflected bilaterally, and the hard palate was punctured in the mid palatal suture using a round bur and a micromotor hand piece (Strong 204, 35000 rpm, 280N/cm, Korea)., 5 perforations were done along the mid palatal suture with 5mm space between each 2 perforations (the depth of each perforation was 2mm), another cuttings were done using fissure bur between each 2 perforations laterally and diagonally to the mid palatal suture. Finally suturing with 0.1 black silk suture using simple interrupted suture technique. [Figure 3 a, b, c, and d]. The pigs were injected with 1 ml /10 kg body weight per day of penicillin (PEN/ STREP, Nederhorst den Berg, Holland) for up to 5 days and 1ml of Metalgin (SPI, Saudi) twice daily for up to 3 days. All operated pigs resumed their consciousness and activities normally nearly 4-5 hours postoperatively. The suture was removed after one week, and the MSE2 was implanted and activated as previously described.
Preparation and injection of i-PRF
Blood collection was done using 10-ml plastic tubes (i-PRF, Choukron plastic, pan vacuum without any additive, USA) from the jugular vein, the tube placed quickly in the horizontal centrifuge (PC-02 Centrifuge, to isolate the i-PRF, the upper plasma layer was collected and designated as i-PRF, then taken from the tube and administered by disposable 5ml syringe (Hettich Universal 320 Zentrifugen, France) at 700 rotations per minute for 3 minutes at room temperature. [15]. The injection was done along the mid palatal suture from anterior (canine areas) to posterior region (4th premolars). The injection of i-PRF was done after opening the suture and mid diastema was appeared (nearly after 1 week of expansion) [Figure 4].
Specimen preparation
The animals were euthanized by injecting an overdose of a combination of Xylazine and ketamine, the procedure was done without causing any suffering to the animals, the MSE2 was removed from the mouth by unscrewing the mini-screws.and remove of bands from the molars by band removal plier, maxilla separated from the mouth and the other region of the head by using a cutting machine, manual scalpel, and surgical scissor to remove the soft tissues. After rinsing with running water, the pieces were placed in containers with a 10% buffered formalin solution to prepare them for histological processing, which included the steps below [16].
• Decalcification: It was done by 10% forming acid and hydrochloric acid 10% for 4 weeks at 37º C.
• Dehydration: By using ethyl alcohol, 70%, 90%, and 100% primary alcohol then 100% secondary alcohol (1.5 hour for each).
• Clearing: Specimens passed 3 times through xylene for 1.5 hour to complete the clearance.
• Paraffin wax embedding: Putting the specimens in a dish of melted paraffin then putting the dish in a temperature of 56-60º C until the xylene was replaced by paraffin (1 hour for each dish). Finally, the specimens placed in a centre of the paraffin block.
• Sectioning: Sectioning of 5-µm thickness, putting glass slide and the wax was molten away using hot oven then cleared using xylene.
• Staining with Hemotoxylin and Eosin: Dehydration is first performed in decreasing alcohol, followed by staining with Mayer’s hemotoxylin [7-10] for 7-10 minutes, then washing with water for 1-5 minutes to remove any remaining stains., staining with eosin for 1-2 minutes, dehydrated in absolute alcohol for 2-3 minutes, cleared with xylene. Lastly, the coverslips fixed on the stained tissue using Dixtrene Plasticiser Xylene (D.P.X).
Histomorphometric analysis
Three histological sections were studied for each animal, and the results were taken as an average of the counts. Histomorphometric evaluation was performed in a blind analysis by an experienced researcher, these were observed under a light microscope (B-383PLi, OPTIKA, Italy using digital camera, OPTIKA, Italy and a PROVIEW Program). Each slide section was divided into four quadrants; the mean value of these quadrants was estimated to ensure approximately complete scanning of each histological section. This mean is the number of osteoblasts (obs) and blood vessels (bvs). The number of obs were counted at 400x while the number of bvs were counted at 100x. The ratio of non-ossified tissue to new bone development was also calculated [17].
To assess the validity of the reading of slides, inter-examinercalibration by second examiner and intra-examiner calibration by the same operator with time lapse of two weeks were done by repeating the counting of osteoblasts, 10 randomly selected slides with blood vessels and percentages of newly generated bone measures A paired t-test revealed no significant differences at the 0.05 level.
Statistical analysis
The number of osteoblasts, blood vessels, and percentage of newly formed bone were statistically analysed using Sigma plot program, mean and standard error, ANOVA, and Duncan test was performed among the different groups. Values of p≤0.05 were considered significant.
RESULTS
The study showed that MSE2 appliance was effective in expanding of mid palatal suture in all groups. It was tolerated by the pigs and all animals survived till the end of the study. No adverse side effects including weight loss, inflammation, wound infection, dehiscence, or appliance failure were occurred.
Histological findings
On day 15, the control group showed mature connective tissue in the middle of the palatal suture gap biopsies, which was characterized by the presence of collagen fibers and a small number of freshly blood vessels, while the corticotomy group showed dense connective tissue, disorganized congested blood vessels and irregular trabeculae bordering the suture space. In corticotomy group with i-PRF, there were mature bone lamellae formations with the connective tissue were observed in the middle of the palatal suture and formation of bone marrow within the bone tissues (Figure 1). On day 45, irregular bone lamellae with presence of bone marrow space, small osteocytes lacunae were seen in control group. Bone marrow space, bone lamellae, osteocytes, and remnants of connective tissue were evident in the corticotomy group, but the corticotomy group with i-PRF demonstrated mature bone development with substantial bone space.
Number of osteoblast cells
Histological finding revealed that the number of osteoblasts were significantly higher in the two experimental groups than the control group on day 15 with the highest number were in the corticotomy with i-PRF group. The number of osteoblasts in each group differed significantly. . .(p≤ 0.05; table 1;.On day 45, the reverse was occurred in which the number of the osteoblasts were the lowest in the corticotomy with i-PRF group and highest in the control groups, while the corticotomy group was in between (Table 1).
Number of blood vessels
The corticotomy with i-PRF group showed a significant increase in the number of blood vessels relative to the other groups on day 15. The numbers of blood vessels were also significantly higher in the corticotomy group than control group. (Table 2; Figure 1). The blood vessels decreased in number in all groups in 45 day with significant different between the three groups, the corticotomy with i-PRF group were the highest and the control group was the lowest value. (P ≤ 0.05; Table 2).
New bone formation
The groups were compared based on newly formed bone percentage (P ≤ 0.05), and considerable differences were found among the groups. The results showed that the corticotomy with i-PRF group had a much higher rate of new bone creation than the other two groups, the corticotomy group was significantly higher than that in control group (Table 3).
Table 1: Comparisons of the number of osteoblast cells among different groups in 15 and 45 day.
|
Group |
Days |
Mean |
SE* |
Duncan** |
P*** |
|
Control |
15 day |
24.25 |
0.62 |
A |
0.001 |
|
Corticotomy |
|
35.25 |
0.35 |
B |
|
|
Corticoromy with i-PRF |
|
50.75 |
0.42 |
C |
|
|
Control |
45 day |
34.75 |
0.52 |
A |
0.001 |
|
Corticotomy |
|
25.00 |
0.30 |
B |
|
|
Corticotomy with i-PRF |
|
21.50 |
0.28 |
C |
|
- Standard error ** Different letters vertically mean a significant difference *** A significant difference existed at p≤ 0.05
Table 2: Comparisons of the number of blood vessels among different groups in 15 and 45 day.
|
Group |
Days |
Mean |
SE* |
Duncan** |
P*** |
|
Control |
15 day |
3.00 |
0.40 |
A |
0.001 |
|
Corticotomy |
|
7.25 |
0.25 |
B |
|
|
Corticotomy with i-PRF |
|
14.5 |
0.40 |
C |
|
|
Control |
45 day |
1.00 |
0.40 |
A |
0.001 |
|
Corticotomy |
|
5.00 |
0.30 |
B |
|
|
Corticotomy with i-PRF |
|
10.50 |
0.68 |
C |
|
- Standard error ** Different letters vertically mean a significant difference *** A significant difference existed at p≤ 0.05
Table 3: Comparisons of the percentage % of new bone development among different groups in 15 and 45 day.
|
Group |
Days |
Mean |
SE* |
Duncan** |
P*** |
|
Control |
15 day |
7.72 |
1.67 |
A |
0.001 |
|
Corticotomy |
|
15.33 |
2.87 |
B |
|
|
Corticotomy with i-PRF |
|
28.30 |
5.76 |
C |
|
|
Control |
45 day |
22.3 |
1.80 |
A |
0.001 |
|
Corticotomy |
|
46.84 |
2.61 |
B |
|
|
Corticotomy with i-PRF |
|
75.55 |
2.27 |
C |
|
- Standard error ** Different letters vertically mean a significant difference *** A significant difference existed at p≤ 0.05
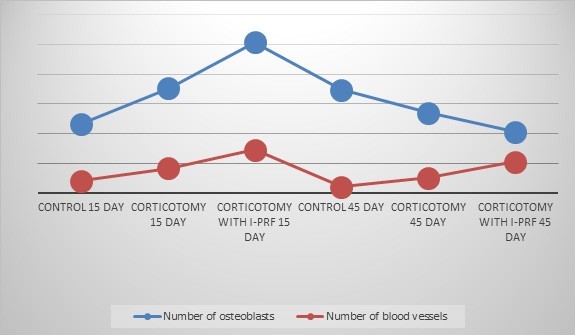
Figure 1: Comparison of the amount of osteoblasts and blood vessels among the groups after 15 and 45 day of expansion.
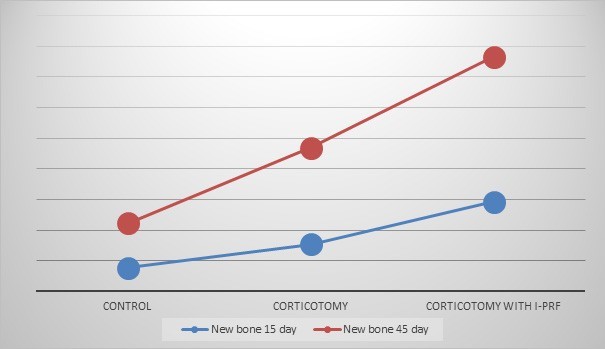
Figure 4: Comparison of the percentage of new bone formation between the groups after 15 and 45 day of expansion.
DISCUSSION
Rapid maxillary expansion is commonly used method to correct transverse maxillary deficiency which is accompanied by unilateral or bilateral posterior cross bite to increase the arch perimeter and relieve crowding in children and adolescents [18]. Recently, successful maxillary skeletal expansion with a tooth bone-borne RME appliance based on mini-screw (MARME), was introduced, which has a higher capacity orthopedic effects than dento-alveolar effects compared to RME in adults [19]. The pigs in some ways are similar to humans in bone composition and this makes them an appropriate animal for research [20]. Also, the pig is tiny in size, easy to manipulate, has an acceptable coast, is easy to house, and is surgically tolerable. When compared to rodents, it possesses a big maxilla; the palate and dental arch are both wide enough to accommodate the surgery. The shape of the molar teeth allowed in fabrication of the expansion appliance. Pigs are used in many medical branches, which include surgery, physiology, and toxicology. This is anticipated to increase in the future due to genetic and oral health [21]. The number of experimental animals were reduced for ethical reasons, so it decreased to the minimal number required to achieve a scientific protocol. The age of the animals was 1.5-2 years old which resemble a skeletally mature pig. All the pigs were males to avoid the possible hormonal changes which could compromise the results. The appliances were tolerated by the animals, Throughout the research, the appliance’s stability was maintained. In this study, the local effect of i-PRF on bone formation in the mid-palatal suture after expansion was investigated by using histomorphometric method. This is the first study that we are aware of that used i-PRF with an enlarged mid-palatal suture. Bone histomorphometry is a reliable and dependable method which can be used to estimate bone formation in experiment in both in vitro and in vivo studies [22]. The histomorphometric parameters used in this study were the number of osteoblasts, to all groups, the number of blood vessels and the percentage of new bone growth were calculated. Mechanical force considered as an important signal which activate growth and regeneration in orthodontic and orthopedic treatments. So, expansion itself can stimulate new bone formation in mid palatal suture [23]. Thus, our study showed that all groups had new bone in the midpalatal suture after expansion but with different significant values among them. The corticotomy with i-PRF group had more beneficial results than the other two groups.
The histological observations of the expanded mid palatal suture were studied in two times interval at 15 and 45 day to observe the early and later effects of i-PRF on bone regeneration in response to maxillary expansion and compared to other groups. At 15 day, the corticotomy group showed denser collagen fibers than the control group, the corticotomy group with i-PRF showed increase number of osteoblasts, blood vessels and new bone formation than the other two groups. Regarding the corticotomy group, the surgery initiates the normal healing process which is called Regional Acceleratory phenomena (RAP), which is a response to stimuli on a local level. In this phenomenon, the tissues formed faster than the normal physiological regional regeneration process, so more bone has been formed than in the control group [24].
Zhou et al., 2019, Corticotomy stimulates osteoblast activity and maturation while also modulating bone metabolism, as explained. in early stage and increase osteogenesis stability after expansion [25]. Some authors recommended the use of cortico-punctures in the cortex of palatine bone in the level of mid-palatal suture and facilitate the process of bone regeneration [26-27].
There were no evident inflammatory cells or osteoclastic activity in the investigation because the osteoclast increased initially and then began to decrease nearly at 7 days, this comes in agreement with others [28,29]. Inside the suture, there were newly formed bone after rapid maxillary expansion in all the groups which were not in contact with the pre-existing bone, which was similar to other study [28].
The corticotomy group with i-PRF showed significant increase in the number of osteoblast, blood vessels and accordingly the percentage of new bone formation than the other two groups.
It is possible to obtain solid or liquid form of PRF according to the blood collection tube and centrifugation protocol. Glass tube used to obtain solid form of PRF because the platelet interacts with glass surface lead to activation of their coagulation by centrifugation process. While the i-PRF collected in a plastic tube maintains its liquid state, 15-30 minute and forms a fibrin clot thereafter [30].
In the current study, we used i-PRF to obtain a liquid formulation taking the advantages of slow and short centrifugation velocity (700 rpm for 3 minutes), so it ispossible to observe an increase in number of regenerative cells, compared to other PRF kinds produced at a faster centrifugation velocity, this PRF type has a higher concentration of growth factors. In addition, the i-PRF is easily manipulated in the mid-palatal suture. I-PRF is an easy, repeatable, minimally invasive, low cost and totally autogenous procedure [31].
I-PRF demonstrated higher release of growth factors at the end of ten days like PDGF-AB, PDGF-AA, epidermal growth factors (EGF) and insulin–like growth factor -1 (IGF-1), cellular migration, induced significantly m-RNA expression of transforming growth factor (TGF-β) and collagen-1 on 7th day, presence of leukocytes in i-PRF act as antimicrobial activity [15,32]. These growth factors promote osteoblast activity, which leads to osteogenesis and new bone production, by stimulating cell mitosis, neo-angiogenesis, and neo-collagenogenesis [30].
I-PRF able to glue all biomolecules within the fibrin scaffold leading to little release to the surrounding media till resorption of fibrin has occurred, which ensures direct administration of biomaterials to the needed environment [30].
The scientific and safe therapy technique was demonstrated in the literature. by using PRF, You et al., concluded that PRF can promote bone regeneration and it is valuable in clinical use [30]. PRF can enhance alveolar cleft reconstruction [31]. PRF considered as a simple, effective and low cost therapeutic support for the treatment of extraction socket in pigs [31].
Other studies showed that PRF is completely an autologous products without biochemical handling, in expensive, contain extended growth factors leukocytes and cytokines which involved in the healing process [31]. I-PRF containing platelet, Type I collagen, leukocytes, growth factors and osteocalcin can induce soft and mineralized tissue healing, it improved the effect of osteogenesis [31].
In 45 day, with a considerable quantity of bone growth, all groups demonstrated an increase in the amount of bone formation was seen in corticotomy with i-PRF group which insure the sustained release of i-PRF in this group.
The physiological polymerization of i-PRF permits the cytokines and growth factors to be stored and slowly released which ensuring a bioactive levels for a long period up to 28 day [31] Study by To et al., showed that in control group, In comparison to dense bone growth, new bone trabeculae were seen. In the socket after 30 day of extraxtion of tooth in A-PRF group, by enhancing the osteoblastic activity [32]. Following expansion, in the early stages of bone rearrangement, there were many fibroblasts and blood vessels present in the suture, while in the stage of maturation, few osteoblasts and fibroblasts were present with small blood vessels, and more regular trabeculae were seen, this is in line with what other people have said [33].
CONCLUSION
Our experimental results indicated that local injection of i-PRF can induce a favorable effect on bone regeneration in the expanded mid-palatal suture of pigs using MSE2 type of MARPE. Accordingly, this will reduce retention time after the enlargement surgery and avoid recurrence.
REFERENCES
1. MacGinnis M, Chu H, Youssef G, Wu KW, Machado AW, et al. (2014). “The effects of micro-implant assisted rapid palatal expansion (MARPE) on the nasomaxillary complex—a finite element method (FEM) analysis” Progress in Orthodontics. 15(1):52.
2. Wang H, Sun W, Ma J, Pan Y, Wang L, et al. (2015). Biglycan mediates suture expansion osteogenesis via potentiation of Wnt /beta-catenin signaling. J Biomech. 48(30):432-440.
3. Le MHT, Lau SF, Ibrahim N, Hayatyd AKN, and Radzia ZB. (2018). Adjunctive buccal and palatal corticotomy for adult maxillary expansion in an animal model. Korean J Orthod. 48(2):98-106.
4. Bazargani F, Feldmann I and Bondemark L. (2013). Three-dimensional analysis of effects of rapid maxillary expansion on facial sutures and bones. Angle Orthod. 83 (6):1074-1082.
5. Kumar N, Desai A, Nambia S and Shetty S. (2021). Miniscrew Assisted Rapid Palatal Expansion (Marpe) – Expanding Horizons To Achieve An Optimum In Transverse Dimension: A Review. European Journal of Molecular & Clinical Medicine. 8(2):389-403.
6. Lion R, Franchi L and Cozza P. (2013). Does rapid maxillary expansion induce adverse effects in growing subjects? Angle Orthod. 83(1):172-182.
7. Carlson C, Sung J, McComb RW, Machado AW, Moon W. (2016). Microimplant-assisted rapid palatal expansion appliance to orthopedically correct transverse maxillary deficiency in an adult. Am J Orthod Dentofacial Orthop. 149 (5):716-728.
8. Möhlhenrich SC, Modabber A, Kniha K, Peters F, Steiner T. (2017). Simulation of three surgical techniques combined with two different bone-borne forces for surgically assisted rapid palatal expansion of the maxillofacial complex: A finite element analysis. Int J Oral Maxillofac Surg. 46(10):1306-1314.
9. AlQadasi B, Aldhorae K, Halboub E, Mahgoub N, Alnasri A. (2019). The Effectiveness of Micro-osteoperforations during Canine Retraction: A Three-dimensional Randomized Clinical Trial. J Int Soc Prev Community Dent. 9 (6):637-645.
10. Melo ACEDO, Carneiro LOT, Pontes LF, Cecim RL, De Mattos. (2013). Factors related to orthodontic treatment time in adult patients. Dent Press J Orthod. 18 (5):59-63.
11. Suri L, Taneja P. (2008). Surgically assisted rapid palatal expansion: A literature review. Am J Orthod Dentofac Orthop. 133(2):290-302.
12. Zhao S, Wang X, Chen NY, Su Y, Zhang J. (2015). Effects of strontium ranelate on bone formation in the mid-palatal suture after rapid maxillary expansion. Drug Des Devel Ther. 9:2725-2734.
13. Cakir S, Gultekin BA, Karabagli M, Yilmaz TE, Cakir E. (2019). Histological Evaluation of the Effects of Growth Factors in a Fibrin Network on Bone Regeneration. J Craniofacial Surg. 30(4):1078-1084.
14. Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, et al. (2014). Advanced platelet rich fibrin: A new concept for cell based tissue engineering by means of inflammatory cells. J Oral Implantol. 40(6):679 689.
15. Miron RJ, Fujioka-Kobayashi M, Hernandez M, Kandalam U, Zhang Y. (2017). Injectable platelet-rich fibrin (i-PRF): opportunities in regenerative dentistry? Clin Oral Investig. 21(8):2619-2627.
16. Suvarana SK, Layton C and Bancroft JD. (2013). Bancroft’s Theory and practice of histological techniques. seventh edition. Churchil Livingstone Elsevier. 317-348.
17. Uysal T, Gorgulu S, Yagci A, Karslioglu Y, Gunhan O, et al. (2011) Effect of resveratrol on bone formation in the expanded inter-premaxillary suture: early bone changes. Orthod Craniofac Res. 14(2):80-87.
18. Choi SH, Shi KK, Cha JY, Park YC, Lee KJ. (2016). Nonsurgical mini-screw assisted rapid maxillary expansion results in acceptable stability in young adults. Angle Orthod. 86(5):713-720.
19. Lin L, Ahn HW, Kim SJ, Moon SC, Kim SH, et al. (2015). Tooth born vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 85 (2):253-262.
20. Mahdi AA, Al-Adili SS, Mohammed ZI. (2020). Clinical and Histomorphomertic Evaluation of Effects of Plateletpoor Plasma and Platelet-rich Plasma on Healing of Extraction Sockets with Buccal Dehiscence: An Experimental Study in Pigs. J Res Med Dent Sci. 8(1):01- 09.
21. Lacombe VA, Podell M, Furr M. Reed SM, Oglesbee MJ, et al. (2001). Diagnostic validity of electroencephalograpgy in Equine intracranial disorders. J Vet Intern Med. 15(40):385-393.
22. Uysal TM, Enhos S, Sonmez M, Sagdic D. (2009). Effect of ED-71, a new active vitamin d analog, on bone formation in an orthopedically expanded suture in rats. A Histomorphometric Study. Eur J Dent b. 3(3):165-172.
23. Zhao S, Yu S, Zhu D, Dai L, Yang P, Xing X. (2020). Stimulatory effects of simvastatin on bone regeneration of the expanded suture in rats. Am J Transl Res. 12(5):1767-1778.
24. Ferguson DJ, Thomas Wilcko M, Wilcko WM, Makki L. (2015). Scope of treatment with periodontally accelerated osteogenic orthodontics therapy. Semin Orthod. 21(3):176-186.
25. Zhou Y, He X, Zhang D. (2019). Study of bone remodeling in corticotomy-assisted orthodontic tooth movement in rats. J Cell Biochem. 120 (9):15952-15962.
26. Cantarella D, Dominguez-Mompell R, Mallya SM, Moschik C, Pan HC, et al. (2017). Changes in the midpalatal and pterygopalatine sutures induced by micro-implantsupported skeletal expander, analyzed with a novel 3D method based on CBCT imaging. Prog Orthod. 18(1):34.
27. Caprioglio A, Fastuca R, Zecca PA, Matteo B, Mangano C, et al. (2017). Cellular midpalatal suture changes after rapid maxillary expansion in growing subjects: a case report. Int J Mol Sci. 18(3):615.
28. Wend S, Kubesch A, Orlowska A, Al-Maawi S, Zender N, et al. (2017). Reduction of the relative centrifugal force influences cell number and growth factor release within injectable PRF based matrices. J Mater Sci Mater Med. 28(12):188.
29. Erdura EA, Karakaslıb K, Oncuc E, Ozturkd B, Hakk S. (2021). Effect of injectable platelet-rich fibrin (i-PRF) on the rate of tooth movement: A randomized clinical trial. Angle Orthod. 91(3):285-292.
30. Agrawal DR, Jaiswal PG. (2020). Injectable Platelet Rich Fibrin (i-PRF): A Gem in Dentistry. International Journal of Current Research and Review. 12(21):25-30.
31. Gulati U, Gulati M, Singh G, Rai D, Vasudeva R, et al. (2019). PRF: A Revolutionary Multipurpose Autogenic Biomaterial. EC Dental Science. 18(9):1977-1999.