Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2022
Dilemma of Papilledema
Anubhav Chauhan1*, Ajay Sharma2, Deepak Kumar Sharma3
1Assistant Professor, Department of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Himachal Pradesh, India
2Assistant Professor, Department of Medicine, Shri Lal Bahadur Shastri Government Medical College and Hospital, Himachal Pradesh, India
3Associate Professor, Department of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Himachal Pradesh, India
*Corresponding author: Anubhav Chauhan, Assistant Professor, Department of Ophthalmology, Shri Lal Bahadur Shastri Government Medical College and Hospital, Mandi at Ner Chowk, Himachal Pradesh, India; Tel: +919816991482; Email: [email protected]
Received Date: December 5, 2022
Publication Date: December 21, 2022
Citation: Chauhan A, et al. (2022). Dilemma of Papilledema. Mathews J Ophthalmol. 7(2):29.
Copyright: Chauhan A, et al. © (2022)
ABSTRACT
Papilledema, when diagnosed, requires urgent management on the part of the treating specialist, as a number of life-threatening diseases are known to be associated with it. We report a rare case of papilledema diagnosed at our center. Multiple interventions helped us in clinching the diagnosis, as early magnetic resonance imaging of the brain and orbit of the patient turned out to be normal.
Keywords: Papilledema, Hypoparathyroidism, Optic disc edema, Intracranial pressure
CASE
A twenty-two-year-old male, admitted to the medicine ward with a history of headache, binocular double vision, and vomiting, was sent to the department of ophthalmology for fundus examination. His general physical examination, systemic examination, routine blood investigations, and neuroimaging were within normal limits as per records. There was no previous history of any systemic disease. Fundus examination revealed bilateral papilledema (Figures 1a and 1b). A suspicion of hypoparathyroidism was also kept as it is often an important, but an overlooked condition. So before performing any further laboratory investigations, the medical specialist ordered an ultrasonography of the neck which revealed right internal jugular vein thrombosis. His serum calcium levels were within normal limits. A repeat magnetic resonance imaging plus magnetic resonance venography of the brain and orbit revealed ' absent flow related enhancement in superior sagittal sinus, right transverse sinus, right sigmoid sinus and right internal jugular vein suggestive of venous sinus thrombosis plus findings suggestive of mastoiditis (right) were also found (Figure 2). His definitive treatment was started by the medical specialist along with workup for coagulation profile, plus an ENT consultation.
.jpg)
Figure 1: Right Eye.
.jpg)
Figure 1(a): Left Eye.

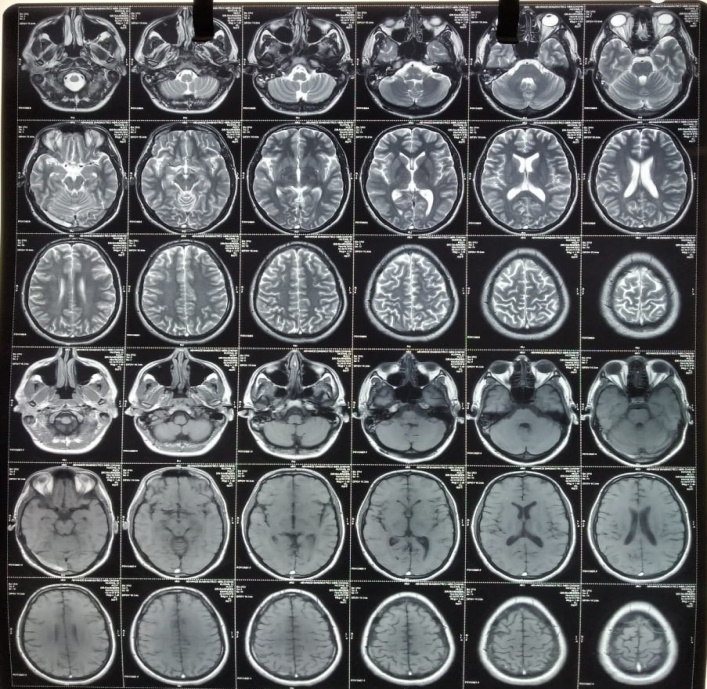

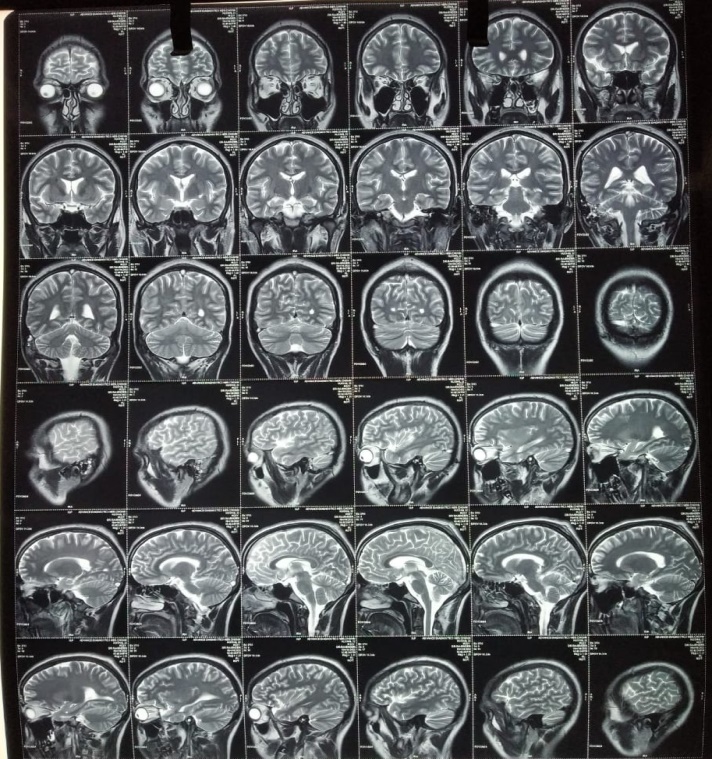
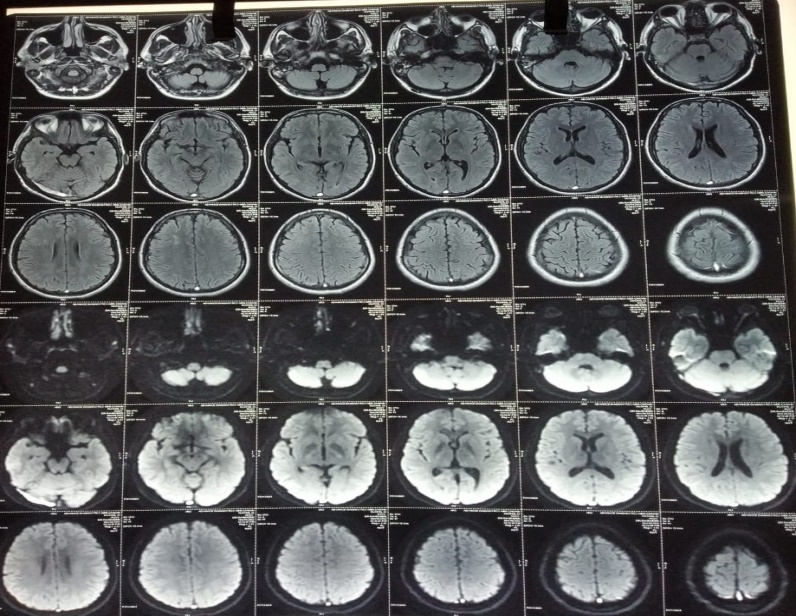
Figure 2: The MRI collage of brain and orbit.
DISCUSSION
The term “papilledema” is defined as optic disc edema secondary to elevated intracranial pressure. Etiology includes intracerebral mass lesions and haemorrhage, hydrocephalus, spinal cord lesions, impairment of cerebral sinus drainage, head trauma, meningitis, idiopathic intracranial hypertension (IIH) etc. [1]. The idiopathic form is diagnosed based on Modified Dandy criteria [2]. Hypoparathyroidism should always be ruled out in these patients [3]. The differential diagnosis includes conditions causing pseudopapilledema like optic disc drusen and hypermetropic disc. Other differentials include optic disc swelling secondary to central retinal vein occlusion, optic neuritis, ischemic optic neuropathy etc. [4]. With the exception of IIH, treatment of papilledema is directed toward correcting the underlying cause [5]. Treatment modality for venous sinus thrombosis include anticoagulation therapy plus management of its complications [6].
REFERENCES
- Rigi M, Almarzouqi SJ, Morgan ML, Lee AG. (2015). Papilledema: epidemiology, etiology, and clinical management. Eye and Brain. 7:47-57.
- Friedman DI, Jacobson DM. (2002;). Diagnostic criteria for idiopathic intracranial hypertension. Neurol. 59:1492-1495.
- Gradisnik P. (2017). Hypoparathyroidism Should Always Be Checked in Papilledema. J Neurosci Rural Pract. 8(3):329.
- Ferreira BFA. (2017). Papilledema: A Comprehensive Assessment. J Neurosci Rural Pract. 8(4):683-684.
- Xie JS, Donaldson L, Margolin E. (2022). Papilledema: A review of etiology, pathophysiology, diagnosis, and management. Survey Ophthalmol. 67(4):1135-1159.
- Saposnik G, Barinagarrementeria F, Brown RD, Bushnell CD, Cucchiara B, Cushman M, et al. (2011). Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 42:1158-1192.