Previous Issues Volume 1, Issue 1 - 2016
Developing a Questionnaire for Evaluating T2DM Patients’ Knowledge, Attitude and Practice Regarding Diabetes Diet
Qi Wang1, 4, Shan-Shan Ma1, 2, Xiao-Yan Zhang3, Yao-Fang Shi1, Hu Ji3, Xiao-Hua Wang1
1Department of Endocrinology of the First Affiliated Hospital of Soochow University, Suzhou 215006, China.
2Kangda College of Nanjing Medical University, China.
3The department of endocrinology of the Second Affiliated Hospital of Soochow University, Suzhou 215006, China.
4Huangshi Central Hospital,Wuhan 435000, China.
Corresponding Author: Xiaohua Wang, Mailbox 203 Main Campus, Soochow University; No.1 Shizi Street, Suzhou, Jiangsu, P.R. China, Tel:+86 512 65221447; E-Mail: [email protected]
Received Date: 29 Feb 2016 Accepted Date: 02 May 2016 Published Date:15 May 2016
Copyright © 2016 Wang X
Citation: Wang X, Wang Q, Shan-Shan M, Xiao-Yan Z, et al. (2016). Developing a Questionnaire for Evaluating T2DM Patients' Knowledge, Attitude and Practice regarding Diabetes Diet. Mathews J Diabetes Obes. 1(1): 001.
ABSTRACT
Aims: To develop and evaluate a diabetic diet management questionnaire for patients with T2DM. Methods: The item pool was formulated based on a literature review and in-depth interviews. An initial questionnaire containing three factors and 30 items was constructed through two rounds of Delphi expert consultation and a preliminary test. A total of 334 patients with T2DM in the Yangtze River Delta region were surveyed to test the reliability and validity of the questionnaire. Results: Three factors with 15 items, including Knowledge management, Attitude management and Practice management of a diabetic diet, were extracted by exploratory factor analysis. The final items explained 51.475% of the total variance, and the content validity index was 0.856. The Cronbach's alpha coefficient was 0.815, and the test-retest reliability was 0.742. Conclusion: The questionnaire was proven to be a reliable and valid tool that allows nurses to evaluate the diet management ability of patients with T2DM. The evaluation outcomes can serve as a basis for individualized health education and interventions for patients with T2DM. KEYWORDS T2DM; Diabetes Diet; Reliability; Validity.
INTRODUCTION The prevalence of diabetes has increased significantly to 11.6% in the Chinese adult population in recent decades [1]. Diabetes is a major risk factor for heart disease and stroke and is a leading cause of mortality [2]. According to a crosssectional hospital-based study in 4 major Chinese cities (Shanghai, Chengdu, Beijing, Guangzhou), 63.0% of the 1511 subjects had poor glycemic control with glycosylated hemoglobin (HbA1c) > 7.5%, in addition to complications [3]. A diabetic diet, as the basic component of self-management for patients with diabetes mellitus, is positively associated with health status and glycemic control of T2DM. However, dietary behavior is very difficult for patients to follow. The non-adherence rate of a DM diet is 44.8%-88.0% in T2DM patients according to cross-sectional investigations [4, 5]. In China, the rates of adequate diet adherence (following the recommended diet and controlling total calories) were 23.5% of all diabetes respondents [6]. Only 9.7% of the Chinese diabetes population had an adequate diet quality [7]. The cause of this lack of adherence might be that Chinese food patterns were too complex to combine with food exchange servings based on glycemic load. Currently, there are tools for evaluating diet adherence. Stunkard and Messick developed the Three Factor Eating Questionnaire (TFEQ), which is used to assess restrained eating, uncontrolled eating and emotional eating, particularly with obese patients [8]. In recent years, it was used with obese patients with T2DM [9]. However, the TFEQ does not emphasize dietary knowledge in the diabetes population. The food frequency questionnaire (FFQ), developed by Lassale, contributed most to energy and macronutrient intake in 1 year of food records [10]. The tool is able to evaluate the actual daily diet of diabetes patients. However, the data collection and analysis process of the FFQ is time consuming, and it also is difficult to evaluate patients' attitude and psychology regarding a diabetes diet. In the north of China, an education assessment questionnaire was designed to assess the nutrition knowledge, attitudes and practices of T2DM [11]. However, the subjects of this study were all local residents of Yakeshi City and did not represent a large region. Due to Chinese vast expanses, the food and diet customs of the South and the North differ greatly, so a diabetic diet self-management questionnaire needs to be developed based on these regions. The objective of our study is to develop a dietary self-management questionnaire that is specific to the diet characteristics of T2DM patients. The tool must have adequate reliability and validity for screening the knowledge, attitudes and practices of diabetes patients regarding diet. Moreover, the tool can aid patients'understanding of themselves and their diabetes diet and can provide feedback and improvement of dietary management.
METHOD AND SUBJECTS
Designing the Questionaire Theoretical framework and conceptual definition: The theoretical framework of the dietary self-management evaluation questionnaire for patients with T2DM was based on knowledge, attitudes, and practices. In Corbett's study, foundational knowledge was a necessary prerequisite to effective diabetes management [12]. Patients must obtain the correct health care knowledge and information so appropriate attitudes can be established and behaviors can be performed correctly [13]. In 2013, the ADA publications 'Standards of Medical Care in Diabetes' suggested that the initial evaluation of people newly diagnosed with diabetes was limited to their eating patterns, nutritional status and weight history [14]. In secondary and tertiary prevention, nutrition therapy is considered to prevent or control the complications of diabetes. Therefore, diet plays a role in diabetes treatment. Many diabetes diets, such as low fat, limited carbohydrate and Mediterranean diets, have been shown to be associated with improvements in metabolic conditions [15]. Previous qualitative studies have demonstrated nutrition knowledge gaps and difficulties in behaviors and beliefs regarding diet in various populations [16, 17]. The particularity of the Chinese diet indicates that health education and questionnaires in diabetes research must be based on a specific population and the problems they face. Our study focused on the population of the Yangtze River Delta region, which is the central east area of China. Item generation and modification: The item pool was generated by integration from three sources:
- Literature reviews of local and foreign publications;
- In-depth interviews with 12 patients who had been diagnosed with T2DM for more than 1 year to identify problems in dietary self-management; and
- Rounds of Delphi expert consultation.
Based on the literature review and in-depth interviews, the initial pool contained a total of 33 items. A Delphi expert consultation was used to modify the items and dimensions of the initial pool. Thirteen experts in related fields (two academic experts in scale development, two nutritionists, five chief physicians of endocrinology and four diabetes clinic nurses/ nursing educators) were invited to evaluate the initial item pool by email. In the first round, every expert provided his independent judgment after two weeks. Using the consultations of the first round, we integrated the experts' advice into the item pool. The items with repetitions and irrelevance in meaning were deleted. The modified items were delivered to every expert by email for the second round. They altered the wording to ensure the rigor of the items. The content validity ratio was calculated with the formula by Lawshe based on the scores from thirteen experts [18]. Ten T2DM patients of various ages, educational backgrounds and occupations were asked to participate in a pilot study to evaluate the comprehensibility of the items. After adjusting and unifying the multidimensional states, a pre-test questionnaire with three factors and 30 items was established. Scale structure and scoring: The initial scale for T2DM diet management included three dimensions: “Knowledge management”, “Attitude management” and “Practice manage- www.mathewsopenaccess.com Citation: Wang X, Wang Q, Shan-Shan M, Xiao-Yan Z, et al. (2016). Developing a Questionnaire for Evaluating T2DM Patients’ Knowledge, Attitude and 3 Practice regarding Diabetes Diet. M J Diab. 1(1): 001. ment”. Finally, the dimensions were amended or confirmed by factor analysis. The knowledge management included multiple-choice questions, and every item contained ten food options, five of which were the optimal choices and the other five were substandard choices. Each optimal choice was given one point, and each substandard choice was given -0.5 points. Then, the items were added to obtain a total value. The Likert 5-point scoring system was used for all the three-partial items. The value of a knowledge item was from -0.25~5, so the scores between “-2.5 ~ -1.1”, “-1 ~ 0.49”, “0.5 ~ 1.9”, “2 ~ 3.49”, “3.5 ~ 5” were respectively recorded as 1, 2, 3, 4 and 5 pionts. The attitude management scale comprised “Mostly disagree”, “Definitely disagree”, “ Uncertainty/Not sure”, “Mostly agree”, “Definitely agree” (1, 2, 3, 4 and 5 points, respectively), and the practice management scale comprised “Never”, “Rare”, “Sometimes”, “Often”, and “Always” (1, 2, 3, 4 and 5 points, respectively). The questionnaire included 5 reverse items. A higher score indicated a stronger diet self-management level. Data collection and subjects: The initial questionnaires were Data collection and subjects: The initial questionnaires were distributed by six investigators who were uniformly trained and who came from six hospitals in the Yangtze River Delta region (Shanghai, Zhejiang and Jiangsu). The sample size was calculated based on an estimate of 10 observations per item [19]. Patients with T2DM from the above areas were selected by convenience sampling to ensure the availability of subjects and adequate sample size. Subjects had to meet the following criteria: aged 18 years or older, diagnosed with T2DM for 1 year or more, have a stable condition (excluding hyperuricemia, acute heart failure, respiratory failure, stroke, cancer, etc.), be capable of self-evaluation and describing their selfcare experience and feelings, and volunteered to participate. Subjects needed to independently finish all three parts of the questionnaire (illiterate patients could answer by others' dictation), and investigators were allowed to offer verbal instructions to assure the homogeneity of the survey. The demographic section could be completed by subjects and nurses in cooperation. Ten percent of subjects were selected randomly to repeat the questionnaire after 4-7 days [20]. All the collected questionnaires were examined, and the questionnaires copies with excessive missing items were not included. Data analysis: All the data in this study were entered into and analyzed with SPSS 18.0 software. Mean ± SD was used to express quantitative variables. The critical ratio (CR), as well as values < 3 with p > 0.05, was deleted, which indicated that the entry decision value should not be used to analyze the items. The Kaiser-Meyer-Olkin (KMO) measure of the data was applied to see whether the questionnaire was suitable for factor analysis. Factor analysis was performed for construct validity. Pearson correlation analysis was employed to evaluate the external consistency of the questionnaire, the correlations between each item and total score or the dimension, and the correlations between each dimension and the total score. Cronbach's alpha coefficient was used to calculate the overall internal consistency of the questionnaire. Pearson correlation analysis was also used to analyze re-test reliability. Ethics: This study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University. Subjects willing to participate signed a written informed consent form. All subjects were assured of confidentiality and the right to decline participation in the study.
RESULTS
Demographic data of subjects Of the 350 patients we approached, two patients refused to complete the questionnaire. Ten questionnaires that contained excessive missing items and four copy with the same answer for all the items were rejected. Accordingly, 334 valid questionnaires were completed, with a response rate of 95.43%. The demographic characteristics of the subjects are shown in Table 1.
Table 1: Demographic characteristics of participants (n=334)
| Baseline items Gender [n (%)] | Value |
|---|---|
| Male | 171(51.2) |
| Mean age, years (SD) Education [n (%)] | 59(13.8) |
| Primary school or below | 99(29.6) |
| Middle and high school | 191(57.2) |
| College or above Married situation [n (%)] | 44(13.2) |
| Unmarried | 10(3.0) |
| Married | 304(91.0) |
| Widowed/Divorce | 20(6.0) |
| Diabetes duration years (SD) Diabetic complication [n (%)] | 8(6.6) |
| Yes | 115(34.4) |
Validity Analysis Surface validity and content validity: The item pool was established based on the literature and interviews with T2DM patients. Two rounds of Delphi expert consultations were held to evaluate the content of the questionnaire. The average work experience of the experts was more than 21 years. Of the initial items, the CVI of items were 0.73 to 1.0, and the average CVI was 0.856. Structure ValidityAccording to our initial structure of the questionnaire, items 1-10 comprised “Knowledge management”, items 11-18 comprised “Attitude management”, and items 19-30 comprised “practice management”. Only the CR value of the item “I don’t eat immoderately, even have dinner outside” was not significant. Therefore, 29 items were retained for factor analysis. The Kaiser-Meyer-Olkin (KMO) value was 0.902, and Bartlett’s sphericity was significant (χ2 = 2258.977, p < 0.001), which indicated the sample was suitable for factor analysis [20]. In the principal component factor analysis, a higher extraction communality value indicates greater influence of the corresponding item. An item was deleted if its extraction communality was less than 0.2. Our communalities were 0.41-0.64. Factor analysis yielded 7 factors with an explained variance of 53.95%. However, not all the items loaded on expected factors. Seven items of “Knowledge management” were retained. The four items of “Attitude management” and four items of “Practice management” did not load on expected factors. The second factor analysis yielded 3 factors, the cumulative explained variance rate of 15 items was 51.475%, and the variance contribution rate of each factor decreased to 13.307%-19.236% (Table 2).
Table 2: Factor Structure and Loading Coefficients of Items Under Each Factor (n = 334)
| Explained Variance Rates (%) / Item | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|
| 18.932 | 19.236 | 13.3.7 | |
| Factor 1. Knowledge management | |||
| 1. Which of the following foods have less effect on blood glucose? | 0.569 | - | - |
| 2. Which of the following vegetables would be the best choice? | 0.666 | - | - |
| 3. Which of the following foods were rich in starch, eating them and reducing the amount of staple food? | 0.488 | - | - |
| 4. Which of the following meat products would be the best choice? | 0.674 | - | - |
| 5. Which of the following foods were rich in dietary fiber, it could increase satiety and promote intestinal peristalsis. | 0.677 | - | - |
| 6. Appropriate intakes of nuts are advantage to the prevention of vascular complications of diabetes,which of the following is nuts? | 0.475 | - | - |
| 7. When you are hungry, which of the following snacks would be the best choice? | 0.653 | - | - |
| Factor 2. Attitude management | |||
| 8. Diet has a great influence on diabetes | - | 0.813 | - |
| 9. Regular quantitative meal is good for stabilizing blood glucose | - | 0.842 | - |
| 10. High fiber foods can alleviate hyperglycemia after meal | - | 0.754 | - |
| 11. Adhering to intake appropriate healthy edible food (eg. Olive oil, rapeseed oil, walnut, almond, peanut) can delay diabetic vascular complications. | - | 0.810 | - |
| Factor 3. Practice management | |||
| 12. I get some coarse grain to substitute for part of polished rice or wheat. | - | - | 0.766 |
| 13. I regard high starchy food (Chinese yam, broad bean, pea) as staple food, and limit the amount. | - | - | 0.706 |
| 14. I get some protein food (tofu, milk, egg, fish, meat) | - | - | 0.565 |
| 15. While going out, I carry candy or snake for hypoglycemia, just in case. | - | - | 0.632 |
The eigenvalues of the common factors were 1.247-4.659. According to the final Scree Plot analysis (Figure 1), three factors were retained, which was consistent with the initial structure. The final questionnaire included 3 factors with 15 items.
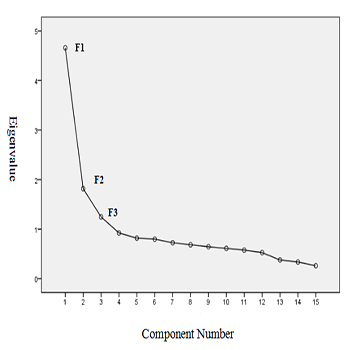
Figure 1:Screen Plot.
Furthermore, the CR values of 15 items were greater than 3, which ensured the identification capability of all items. The final items were measured according to the correlation coefficient between each subscale score and the total score. The correlation coefficient of the final items' scores and the total score was 0.414-0.755. The correlation coefficient of the final items and each subscale were all greater than 0.580, and most were greater than 0.650 (Table 3).
Table 3: Results of structure validity analysis.
| Items | Critical ratio (CR) | Correlation coefficient of each individual item and its dimension | Correlation Coefficient of each Dimension and total score | |
|---|---|---|---|---|
| Factor 1. Knowledge management | 7 | 6.85~11.00* | 0.580~0.676* | 0.747* |
| Factor 2. Attitude management | 4 | 17.30~20.67* | 0.845~0.880* | 0.840* |
| Factor 3.Practice management | 4 | 7.65~10.51* | 0.580~0.731* | 0.673* |
Reliability Analysis
Internal consistency coefficient: The internal consistency coefficient of the questionnaire, known as the Cronbach's coefficient, was 0.815. The internal consistency coefficients of the knowledge, attitude, and practice management subscales were 0.739, 0.885 and 0.616, respectively (Table 4).
Table 4: Reliability of the questionnaire and its subscales.
| Subscale | Items | Cronbach’ alpha coefficient | Re-test reliability |
|---|---|---|---|
| Factor 1. Knowledge management | 7 | 0.739 | 0.859 |
| Factor 2. Attitude management | 4 | 0.885 | 0.779 |
| Factor 3.Practice management | 4 | 0.616 | 0.724 |
Re-test reliability: According to the results of the re-test performed by twenty-nine patients 4-7 days later, the re-test reliability of the final 15 items was 0.742. The coefficients of the knowledge management, attitude management and practice management subscales were 0.859, 0.779 and 0.724, respectively, which were significant (p < 0.001). These results indicated that our questionnaire had adequate stability over time.
DISCUSSION Diet is regarded as the basic component of diabetes self-management. Diabetes patients' compliance to a diabetes diet determines their progression of diabetes. This questionnaire that evaluated diabetes dietary self-management in patients living in the Yangtze River Delta, China, demonstrated adequate reliability and validity. The tool also provided a comprehensive and practical guide for patients with T2DM and nurse specialists. The knowledge section of our questionnaire was relevant, as all the options were common and specific foods in the local population. Accordingly, the tool can aid diabetes educators to understand the details and to help patients recognize highfiber, health fat, and low starch foods, which strengthen the diabetes diet. Basic food exchange methods were integrated into the practice section to accurately screen compliance to a diabetes diet. Finally, patients received targeted feedback without the bias of subjective assessment. The tool also can aid diabetes patients and educators that intaking and exchanging of high-fiber grains, control of carbohydrates are first-aid for hypoglycemia. We adopted a weighting method to score the knowledge subscale, and we considered that some foods were optional, some were substandard, and all the choices were appropriate for this population. This questionnaire was developed in strict accordance with the literature, interviews, expert consultations and actual investigation. The validity of the questionnaire for T2DM diet management was examined with content validation by multidisciplinary experts and construct validation by exploratory factor analysis. The Cronbach's alpha coefficient of the questionnaire was 0.815, which is superior to the ideal value of 0.8. The Cronbach's alpha coefficients of the three subscales were all greater than 0.6, which indicates that the questionnaire had high internal consistency. Despite the strict process, the study had some limitations. (1) In this study, we used convenience sampling instead of random sampling, although our samples came from different hospitals. (2) We could not identify the participants' ancestral home in advance. Dietary behavior has distinct regional characteristics. Our study neglected floating populations that included non-native patients. These people are not suited for evaluating this region-specific questionnaire. (3) Due to substantial missing data of FBG and HbA1C, concurrent validity was not measured in our study. Further research should consider these limitations to improve future studies.
CONCLUSION
This study demonstrated the validity and reliability of a questionnaire for evaluating diabetes diet management in patients with T2DM in the Yangtze River Delta, China. The questionnaire focused on modification of dietary knowledge, attitudes and practices throughout the entire course of diabetes. This tool could be a practical guide for nurses to identify existing diet problems, provide feedback that includes individualized health education and interventions to patients, and help patients change to a healthy dietary pattern.
AUTHORS CONTRIBUTION
Qi Wang and Shan-shan Ma made the same contribution to this study.
DISCLOSURES
The authors hereby declare that no conflict of interest exists regarding this article.
REFERENCES
- Xu Y, Wang L, He J, Bi Y, et al. (2013). Prevalence and Control of Diabetes in Chinese Adults JAMA. 310(9), 948-958.
- Roglic G and Unwin N. (2010). Mortality attributable to diabetes: estimates for the year 2010 Diabetes Res Clin Pract. 87(1), 15-19.
- Liu Z, Fu C, Wang W and Xu B. (2010). Prevalence of chronic complications of T2DMmellitus in outpatients - A cross-sectional hospital based survey in urban China Health and Quality of Life Outcomes. 8, 62.
- Mumu SJ, Saleh F, Ara F, Afnan F, et al. (2014). Non-adherence to life-style modification and its factors among T2DM patients Indian J Public Health. 58(1), 40-44.
- Saleh F, Mumu SJ, Ara F, Hafez MA, et al. (2014). Non-adherence to self-care practices & medication and health related quality of life among patients with type 2 diabetes: a crosssectional study BMC Public Health. 14, 431.
- Yang X, Li X and Zhang R. (2010). The Investigation of Relationship between Dietary Therapy Adherence and Metabolism Control in Patients with Type 2 Diabetes Chinese Journal of Nursing. 45(7), 624-626.
- Lin Y, Guo H and Deng Z. (2004). Evaluating dietary quality of type 2 diabetics in Macao by healthy eating index Journal of Hygiene Research. 33(6), 737-740.
- Stunkard AJ and Messick S. (1985). The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger J Psychosom Res. 29(1), 71-83.
- Ryan M, Gallanagh J and Livingstone MB. (2008). The prevalence of abnormal eating behaviour in a representative sample of the French diabetes population Diabetes & Metabolism. 34(6), 581-586.
- Lassale C, Guilbert C, Keogh J , Syrette J, et al. (2009). Estimating food intakes in Australia: validation of the Common wealth Scientific and Industrial Research Organisation (CSIRO) food frequency questionnaire against weighed dietary intakes J Hum Nutr Diet. 22(6), 559-566.
- Wang H, Song Z, Ba Y, Zhu L, et al. (2013). Nutritional and eating education improves knowledge and practice of patients with T2DM concerning dietary intake and blood glucose control in an outlying city of China Public Health Nutrition. 17(10), 2351-2358.
- Corbett CF. (1999). Research-based practise implications for patients with diabetes.Part II: diabetesself-efficacy Home Healthc Nurse. 7(9), 587-596.
- Kobe JA. Aspects of nutritional knowledge, attitudes and practices of nurses working in the surgical division at the Kenyatta national hospital, Kenya. 2006-2012.
- Standards of medical care in diabetes -2013. (2013). Diabetes Care, 36(supplement1). S11-S66.
- Khazrai YM, Defeudis G and Pozzilli P. (2014). Effect of diet on T2DMmellitus: a review Diabetes Metab Res Rev, 30(suppl. 1), 24-33.
- Wermeling M, Thiele-Manjali U, Koschack J, Lucius-Hoene G, et al. (2014). T2DM patients' perspectives on lifestyle counselling and weight management in general practice: a qualitative study BMC Family Practice. 15, 97.
- Mathew R, Gucciardi E, De Melo M and Barata P. (2012). Self-management experiences among men and women with T2DM mellitus: a qualitative analysis BMC Family Practice. 13, 122.
- Wu ML. (2003). SPSS statistics application Peking, Science Press. 62-110.
- Browne MW. (2001). An Overview of analytic rotation in exploratory factor analysis Multivar Behavl Res. 36(1), 111- 150.
- Daving Y, Andren E, Nordholm L and Grimby G. (2001). Reliability of an interview approach to the Functional Independence Measure Clin Rehahil. 15(3), 301-310.