Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
Cytodiagnosis of a Thyroglossal Duct Cyst in a Tertiary Facility: A Case Report of a 27-Year-Old Female
Boaz Mwesigwa1,*, Derrick Barry Abila2, Anatoli Mawanda1,2, Tusiime Charity Claire1, Zelma Cason3
1Department of Pathology, Mulago National Referral Hospital, Kampala, Uganda
2Department of Pathology, Makerere University, Kampala, Uganda
3Department of Pathology, University of Mississippi, Tennessee, USA
*Corresponding author: Boaz Mwesigwa, Department of Pathology, Mulago National Referral Hospital, Kampala, Uganda, Tel: +256705482996; Email: [email protected].
Received Date: November 08, 2023
Published Date: December 08, 2023
Citation: Boaz M, et al. (2023). Cytodiagnosis of a Thyroglossal Duct Cyst in a Tertiary Facility: A Case Report of a 27-Year-Old Female. Mathews J Cytol Histol. 7(2):26.
Copyrights: Boaz M, et al. © (2023).
ABSTRACT
A thyroglossal cyst is an inherent anomaly originating from remnants of the thyroglossal duct, a structure that connects the thyroid gland to the tongue during early embryonic development. Typically benign in nature, these cysts are situated along the midline of the neck, often in close proximity to the hyoid bone. In this report, we present an extraordinary and atypical case of a thyroglossal cyst in a 27-year-old female who manifested a painless swelling in the midline of her neck. A subsequent ultrasonogram revealed the presence of a thyroglossal duct cyst in the anterior neck region. Notably, fine needle aspiration cytology (FNAC) yielded benign results. In addition to detailing the cyto-diagnostic features characteristic of this specific lesion, our report underscores the significance of FNAC as a foremost diagnostic approach in the assessment of uncommon anterior neck masses. Through this case, we emphasize the importance of FNAC in the early and accurate management of such distinctive presentations.
Keywords: Cytology, Fine Needle Aspiration, Thyroglossal Cyst.
INTRODUCTION
Thyroglossal duct cysts (TGDCs) are the most prevalent congenital neck cysts, constituting approximately 70% of cases [1], and occurring in about 7% of the general population [2]. Despite their common occurrence, thyroglossal duct cysts are relatively uncommonly reported in the literature. These cysts typically manifest as mobile, non-tender, and non-lobular swellings in the neck, usually located below the hyoid bone [3]. Cytodiagnosis of a thyroglossal cyst involves the collection of cell or fluid samples from the cyst through a fine needle aspiration (FNA) procedure. This technique entails inserting a thin needle into the cyst to aspirate cells for subsequent analysis. The collected cells are then examined under a microscope to discern their characteristics. Notably, instances of thyroglossal cysts located in the anterior neck are infrequently documented in the literature. In this context, our aim was to present a unique case involving the diagnosis of a thyroglossal cyst through fine needle aspiration cytology, highlighting the rarity and diagnostic approach of this condition.
CASE PRESENTATION
A 27-year-old female presented to the Fine Needle Aspiration Cytology (FNAC) clinic at Mulago National Referral Hospital with a painless midline anterior neck mass that had been progressively enlarging over a four-month period (Figure 1). The patient reported no breathing or swallowing difficulties, and no familial history of thyroid carcinoma was reported. Biochemical tests of thyroid function revealed a TSH level of 0.349 miu/ml (Reference Range: 0.600-4.000) and a T4 level of 8.00 ug/dl (Reference Range: 5.00-12.00).

Figure 1. Anterior neck midline swelling.
Ultrasonography of the anterior neck revealed a well-defined hypoechoic mass situated midline between the strap muscles, below the hyoid bone. Color Doppler imaging showed no vascular flow within the mass (Figure 2). On physical examination, the mass was palpable, soft in consistency, non-tender, and exhibited mobility upon swallowing.
.png)
Figure 2. Ultrasonogram of the anterior neck swelling showing a thyroglossal duct cyst.
Following informed consent from the patient, a 23-gauge needle was used to aspirate a yellowish-mucoid material from the nodule. The aspirated material was used to create two slides—one slide air-dried for Diff-Quick stain and the other fixed in alcohol for Papanicolaou stain. Cytological examination of the Fine Needle Aspiration Cytology (FNAC) slides revealed numerous anucleated squames, mature squamous cells, and necrotic debris (Figure 3a & Figure 3b). The FNAC results were indicative of a benign aspirate consistent with a thyroglossal cyst. Consequently, excision was recommended as the course of action.
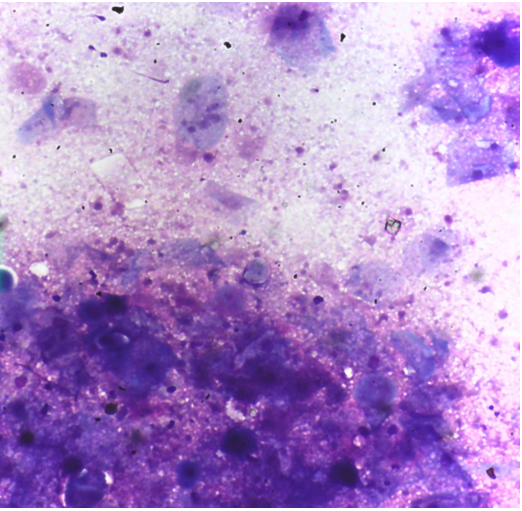
Figure 3a. Photomicrograph of Fine needle aspirate reveals numerous anucleate squames and mature squamous cells (Diff quick stain X200)
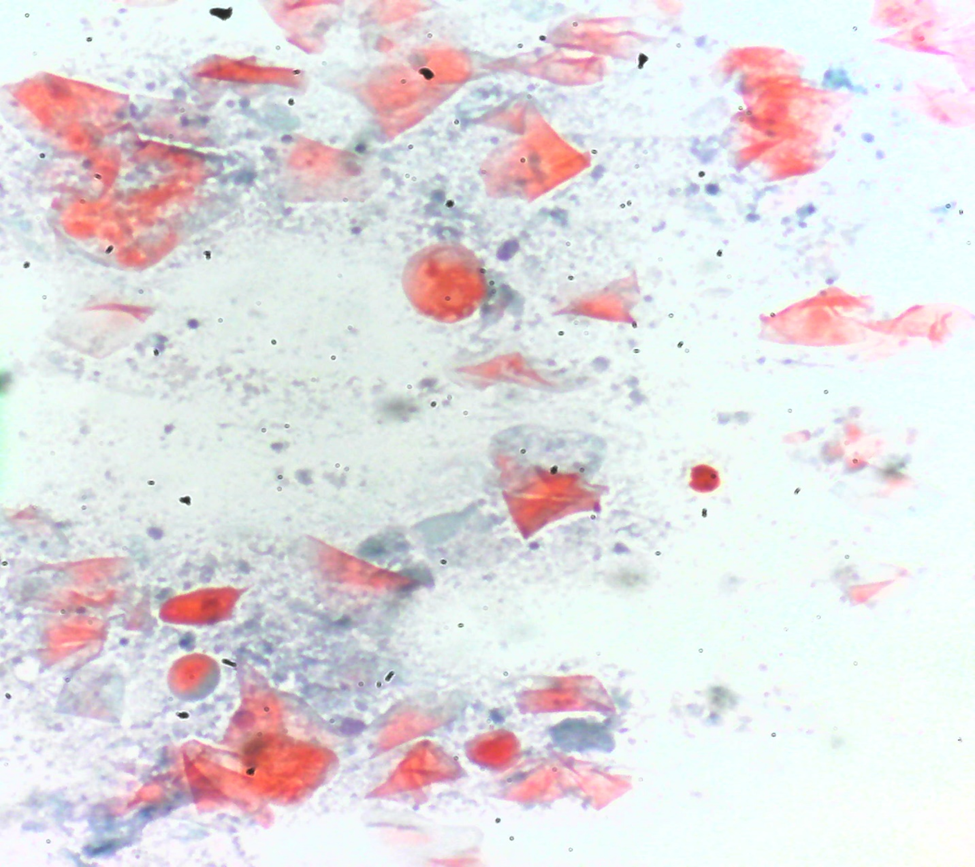
Figure 3b. Photomicrograph of Fine Needle Aspirate reveals a dirty necrotic background (Papanicolaou stain X200).
DISCUSSION
Thyroglossal duct cysts (TGDCs) represent a prevalent congenital anomaly manifesting as anterior cervical masses. These cysts stem from remnants of the thyroglossal duct, a structure originating during embryonic thyroid development. The duct typically regresses as the thyroid migrates to its final position in the neck, but incomplete obliteration can lead to the formation of TGDCs. Although commonly encountered in pediatric patients, TGDCs can also arise later in life [4]. Typically situated midline, TGDCs can occasionally occur paramedian and are commonly found below the hyoid bone [5].
In the case presented, the patient exhibited a painless midline neck swelling, consistent with a thyroglossal duct cyst. The utilization of fine needle aspiration cytology (FNAC) facilitated a definitive diagnosis. FNAC offers a sensitivity, specificity, and diagnostic accuracy of 100% for TGDCs, underscoring its role as the primary diagnostic modality for these lesions [6]. The cytologic evaluation of TGDCs reveals diverse cellular components, including proteinaceous material, squamous cells, inflammatory cells, and colloid [7]. Stratified squamous cells and cholesterol crystals distinguish TGDCs from thyroid cystic nodules [8]. Our findings align with these cytologic features, strengthening the accuracy of the FNAC-based diagnosis.
Notably, the FNAC technique offers a simple, safe, and cost-effective means of pre-operative assessment for TGDCs. Its role in the accurate identification of benign lesions is underscored by our case report. This approach obviates the need for more invasive diagnostic procedures, which would be particularly relevant for cystic masses with benign attributes. The successful diagnosis and subsequent recommendation for excision in our case exemplify the clinical utility of FNAC in guiding patient management.
CONCLUSION
In conclusion, our case contributes to the existing literature by presenting a rare instance of a thyroglossal duct cyst diagnosed through FNAC. The diagnostic accuracy and minimal invasiveness of FNAC make it a valuable tool for the assessment of anterior neck masses. Further research and case reports will likely continue to highlight the crucial role FNAC plays in diagnosing and managing these conditions.
STUDY APPROVAL STATEMENT
This study was granted a waiver since it did not entail the introduction of novel techniques or procedures. The data presented in this study are derived from established clinical practices and diagnostic procedures.
DECLARATION OF PATIENT CONSENT
Written informed consent was duly obtained from the patient for the purpose of publishing this case report along with its accompanying images. A copy of this written consent is readily available and can be provided for review upon request by the Editor-in-Chief of this journal.
FINANCIAL SUPPORT AND SPONSORSHIP
This research was conducted without receiving any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The study was entirely self-funded and not reliant on external financial support or sponsorship.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest associated with the content presented in this case report.
AUTHOR CONTRIBUTIONS
M.B. conceptualized and designed the study, conducted a comprehensive literature search, and authored the manuscript. D.A., A.M., T.C, D.W and K.S. conducted preliminary data analysis, contributed to manuscript writing, and participated in shaping the content. Z.C. performed formal data analysis, created visualizations, contributed to study design, and actively participated in manuscript composition. All authors collectively participated in the final review and editing of the manuscript, ensuring its accuracy and coherence.
DATA AVAILABILITY STATEMENT
All data generated or analyzed during the course of this study are comprehensively included within this article. For any additional inquiries or further information, interested parties are encouraged to directly contact the corresponding author.
REFERENCES
- Mortaja S, Sebeih H, Alobida NW, Al-Qahtani K. (2020). Large Thyroglossal Duct Cyst: A Case Report. Am J Case Rep. 21:e919745.
- Park JS, Kim DW, Shin GW, Park JY, Lee YJ, Choo HJ, et al. (2020). Prevalence and Features of Thyroglossal Duct Cyst on Ultrasonography, According to Radioactive Iodine Therapy: A Single-Center Study. Front Endocrinol (Lausanne). 11:188.
- Taha A, Enodien B, Frey DM, Taha-Mehlitz S. (2022). Thyroglossal Duct Cyst, a Case Report and Literature Review. Diseases. 25;10(1):7.
- Thabet H, Gaafar A, Nour Y. (2011). Thyroglossal duct cyst: Variable presentations. . 12:13-20.
- Vazquez Salas S, Pedro K, Balram A, Syed S, Kotaka K, Kadivar A, et al. (2022). Head and Neck Cystic Lesions: A Cytology Review of Common and Uncommon Entities. Acta Cytol. 66(5):359-370.
- Komal Singh L, Rakesh AH, Santosh GG, Umashankar S. (2013). Diagnostic accuracy of fine needle aspiration cytology in thyroid lesions: A hospital-based study. . 10(2):68-71.
- Hou T, Liu Z, Gan Q, Debnam JM, Krishnamurthy S. (2022). Clinical and cytopathological features of suspected thyroglossal duct cysts and neoplasms arising from them: A large series from a referral cancer center. Cancer Cytopathol. 130(1):72-79.
- Mikac G, Biukovic M. (2016). Cytological Analysis of Thyroglossal Duct Cysts. Med Pregl. 69(5-6):135-139.