Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
Current Status of Neonatal Death in a Second Level of Care Hospital in the State of Mexico
Martin Noé Rangel Calvillo*
Specialist in Pediatrics and Neonatology, Former ExChief of Pediatrics and Neonatology (01-2022) at HGE José María Rodríguez, Ecatepec state of Mexico, Mexico
*Corresponding author: Dr. Martin Noé Rangel Calvillo, Specialist in Pediatrics and Neonatology, Former ExChief of Pediatrics and Neonatology (01-2022) at HGE José María Rodríguez, Ecatepec state of Mexico, Mexico, Tel: 5561140092; Email: [email protected].
Received Date: September 11, 2023
Published Date: November 07, 2023
Citation: Calvillo MNR. (2023). Current Status of Neonatal Death in a Second Level of Care Hospital in the State of Mexico. Mathews J Pediatr. 8(2):30.
Copyrights: Calvillo MNR. © (2023).
ABSTRACT
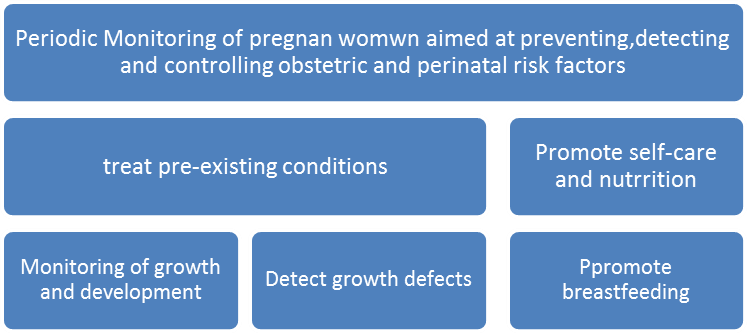
In a previous analysis, it was confirmed that by detecting these opportunities for improvement in the obstetric care process, new strategies will be found each time to avoid factors that seriously impact the health of Neonates. Objective: Monitor the current state of neonatal death taking into account a timeline in a previously monitored population, trying to detect preventive actions, to specifically protect the newborn, and having a favorable impact on maternal health. Method: Under informed consent of patients; Analysis of clinical records of 171 newborn deaths was carried out. The analysis was designed according to the recommendations of Dr. Brown, who assigned a percentage of responsibility basically in 4 areas; 1.- Women's health to whom I give a very high weight of 60% of responsibility. 2.- Maternal care with 10% responsibility. 3.- Neonatal Care 9% responsibility. 4.- Postnatal Care, 21%. In the research design we decided to include the color code recommended by Dr. Brown: #1 Brown, #2, Red, #3, Green, #4 Lilac, which are expressed in a table to contain data for each patient and with This will identify an area of responsibilities to convert it into an area of Opportunity. Once the number of Neonatal deaths from the period 2010-2015 was analyzed, the results were compared with previous periods, previously analyzed, to measure if there are new factors that require new approach strategies. Results: In period 203-206, basically three pathologies responsible for death: 61% Prematurity, 25% sepsis, 61.7% asphyxiation, and according to color code they entered the scope of responsibility of obstetric care In 2007-2008: an increase in Prematurity occurred to 66.6%; There was a decrease in sepsis to 14% and a decrease in babies under 1500g to 46.6%, after applying first analysis strategies. In the period 2010-2015, premature births decreased to 63%; Asphyxias decreased by 38% and sepsis remained at 14%. Babies weighing less than 1500g increased to 57.7%. Conclusions: We can observe that the risk factors for neonatal death remained present, but we noted a significant decrease compared to previous periods, according to the analysis of the Dr. Brown method, which translates into an area of opportunity for improvement with high weight for the area of obstetric care, we can also comment that the newborns within the Neonatal area of responsibility were registered once they were very seriously ill from birth and after neonatal intensive care, by age they entered that area of responsibility, also clarify that the patients, In 98% of cases the asphyxia was intrauterine. Permanent monitoring is urgently needed, and emphasis is placed on applying a 4x4 team formation strategy in the field of women's and pregnant women's health.
Keywords: Death, Neonatal, Current Analysis.
BACKGROUND
Concern about obstetric care dates back to pre-Columbian times in Mexico, where the midwife was already a respected character in society [1]. Since then, obstetric complications continue to be considered as a setback that puts the life of the patient at risk. Product and of the pregnant woman, during childbirth or puerperium; or that generates serious sequelae, or death to the baby and/or the mother.
Currently in our country the social, economic, educational factors converge strongly in the health systems, causing the pregnant woman to appear in the care services have failures in some of the "Critical links of her care"
In a previous article (Analysis of neonatal mortality Aug 2015 M.N. Rangel Calvillo Rev.Perinatologia y Reprooduccion Humana) the first analyzes were carried out in this regard and already suggesting the strategies that at some point when applied Iván will favorably influence the chain of links critical, identified, as opportunities for improvement during the care of the binomial that would reduce neonatal death in addition to neurological damage and its serious sequelae in newborns. These studies also mention the prevailing need to continuously evaluate the state of Neonatal mortality, as an index of high hospital weight that will help verify obstetric care in the country.
The foregoing with the sole intention of detecting opportunities for improvement in the obstetric care process and detecting strategies that help us avoid factors that have a serious impact on neonatal health.
The current objective of this analysis will be to verify the current state of neonatal death at the time of the cut and shed light to improve the care of the pair. Yes, we detect preventive actions to specifically protect the newborn and with repercussions on the mother or vice versa seen as a palindromic concept.
This is a retrospective study, carried out in the period from 2010 to 2015 in a population of pregnant women treated at the HGEJMR public hospital with a second level of care and which at the time was classified as a high specialty in Neonatology under the Catastrophic Expenses regime. Where open care is offered to the low-income population, located north of Mexico City in the most densely populated municipality in our country.
The already mentioned objective will be to detect factors that have an impact increasing the number of neonatal deaths. We hope to increase a database that helps make urgent decisions to avoid not only neonatal death but also serious neurological sequelae, as well as maternal death. Obviously with repercussions in the reduction of hospital expenses.
The current objective of this analysis will be to verify the current status of neonatal death at the time of the cutoff and shed light to improve the care of the binomial. Yes, we detect preventive actions to specifically protect the newborn and with repercussions on the mother or vice versa, seen as a palindromic concept.
This is a retrospective study, carried out from 2010 to 2015 in a population of pregnant women treated at the HGEJMR second-level public hospital, which at the time was classified as a high specialty in Neonatology under the Catastrophic Expenses regime. Where open care is offered to the low-income population, located north of Mexico City in the most densely populated municipality in our country.
The aforementioned objective will be to detect factors that have an impact by raising the number of neonatal deaths. We hope to increase a database that will help make emergency decisions to avoid not only neonatal death but also serious neurological sequelae, as well as maternal death. Evidently with an impact on the decrease in hospital spending [2-10].
METHOD
We will analyze clinical records according to the recommendations of Dr. Brown, applied at the time in Georgia, we remember that this analysis helped reduce maternal death in the USA by 80%, which seemed attractive to us to try, set our precedents means when trying to apply it, the system is ordered in areas, which can be seen as improvement opportunities for the areas, which detect responsibilities in their medical care processes, without forgetting the limitations, which implies, scarcity of resources.
These areas were called the area of responsibility and a percentage of responsibility was assigned to them, namely:
1.-Women´s health 60%
2.-maternal care 10%
3.-Neonatal care 9%
4.-Postnatal care 21%.
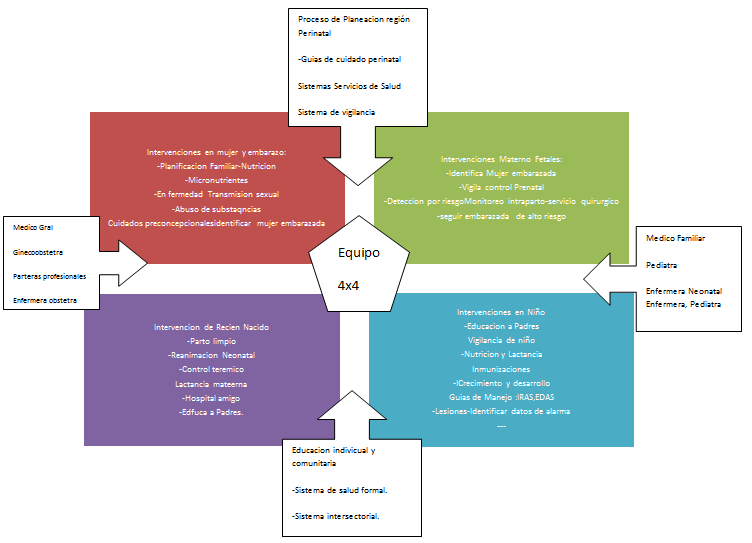
In turn, each of these opportunities bécame perinatal interventions, which in the method Dr Brown assigns with color code:
1.-For women´s health the color Brown
2.-Maternal fetal care network
3.-Newborn care the green
4.-Postnatal care lilac color.
Interventions in the lilac child With this, neonatal, deaths were grouped and weight was assigned by, which interventions are assigned to reduce or eliminate the factors that contribute to death in neonatal case. (Colaborating Centered in Reproductive Health the National Centers For Disease Control and Prevention Georgia Department of Human Resource)
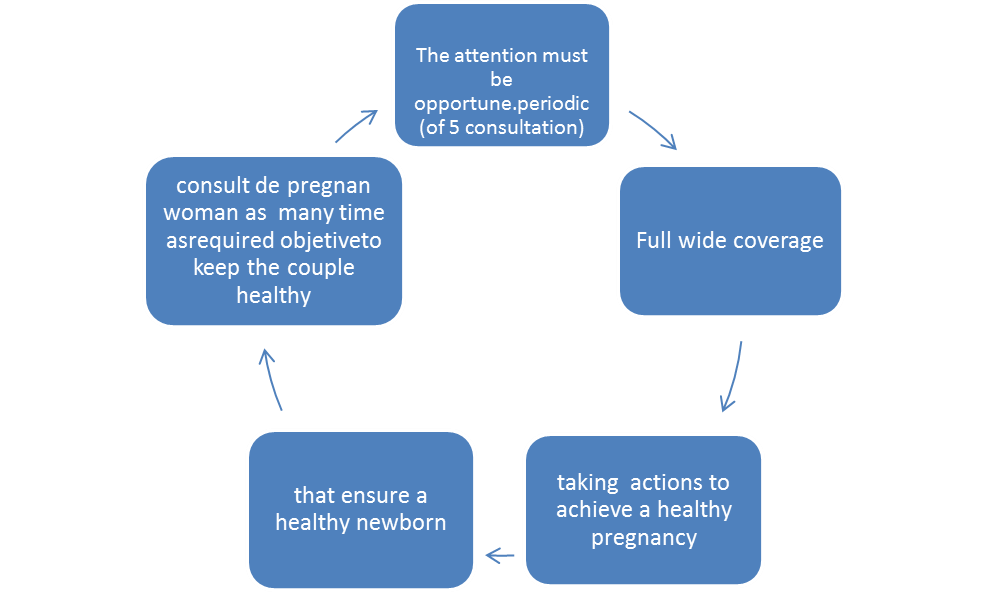
The result is a survillance system for the management of perintal care, integrated by a data collections system once the problem has been defined. Data analysis, which leads us to the solution of the problem or response when applying the solution, the results are monitored, until a specific solution is obtained for each area of opportunity.
We also rely on the official Mexican standard. To monitor the health of women and babies.
Color code table was applied where we can observe, color code where late fetal death is first classified by age in those:
-older 28weeks
Early neonatal death in those younger so 7 days
-Late neonatal death from 7 to 27 days
-And Postnatal death in the olders 28 days and more
Brown’s colors were assigned by weight the group from 0 to 999gr. Second group from 999 to 1499gr. And weight very low birth.
The low birth weight from 1.499gr to 2400gr.
The first color is Brown, second reed, third green and fourth laila
Including the appropriate weight up to 2500g
Two previously analyzed periods will be taken into account to make a comparison with
RESULTS
Once we apply the analysis table proposed by Dr. Brown, we find in the year 203-206 61% premature, 25% sepsis, 61.7% asphyxia as the main causes of neonatal death.
It draws our attention that when applying the color code again we find variations in the prevalence of causes of death
In 2007-2008 there was an increase in premature to 66.6%, a decrease in sepsis to 14%, and a decrease in babies under 1500gr to 46.6%.
In the period 2010-2015: premature infants decreased to 63%, asphyxia decreased to 38%, and sepsis decreased to 14%, those <1500gr increased to 57.77%.
Table 1. Neonatal mortality analysis of the HGEJMR period 2010-2015.
|
Late Fetal deaths (28+ Weeks ) |
Early Neonatal deaths (<27days) |
Late Neonatal deaths (7-27 days) |
Deaths Post neonatal (28+ days) |
|
|
Weight 0-999gr |
28 |
25 |
7 |
|
|
Very low Weight 999-1499gr |
60 |
38 |
16 |
|
|
Low birth weight 1449-2499gr |
54 |
33 |
21 |
|
|
Suitable weight 2500>gr |
46 |
32 |
16 |
In the following tables we present other biological factors that were monitored, and continue to be observed,
|
Age of product |
# de casos |
|
21-24 semanas |
17 |
|
25-28 |
47 |
|
29-32 |
101 |
|
33-35 |
66 |
|
37-40 |
59 |
|
Product age in weeks |
|
|
21-24 |
18 |
|
25-28 |
48 |
|
29-32 |
101 |
|
33-35 |
75 |
|
37-40 |
64 |
|
# of consultations |
#of cases |
|
01-02 |
71 |
|
03-05 |
103 |
|
5 |
88 |
|
none |
38 |
|
education of the mothers |
|
|
Illiterate |
21 |
|
Primary |
89 |
|
Secondary |
127 |
|
High School |
57 |
|
Professional |
12 |
|
Product Age |
# of Patients |
|
<de 60 minutes |
25 |
|
2-48hrs |
52 |
|
24-48hrs |
18 |
|
48-72 |
29 |
|
72-160 |
37 |
|
+ 6 dias |
123 |
|
APGAR |
# of patients |
|
0-3 |
83 |
|
04-Jun |
84 |
|
05-Sep |
139 |
|
Personnel who attended delivery |
89 |
|
Medical Intern |
103 |
|
M Resident |
81 |
|
Random |
10 |
|
Random |
23 |
|
M Private |
1 |
|
Another |
3 |
|
Pasante |
|
Risk according to method of obtaining |
|
|
vagina |
151 |
|
Abdominal |
136 |
|
Forceps |
16 |
|
Maternal age in years |
# of cases |
|
16 |
53 |
|
17-20 |
89 |
|
20-30 |
100 |
|
30-38 |
47 |
|
40 |
19 |
|
Marital status |
# of patients |
|
Single |
98 |
|
Married |
69 |
|
free union |
135 |
|
Widow |
1 |
|
Separate |
3 |
|
|
Premature |
Sepsis |
Asphyxia |
<1500gr |
|
2003-2006 |
⇧5.6% |
⇧2.5% |
⇩7.6% |
⇧14% |
|
2007-2008 |
⇩5.6% |
⇩14% |
⇧30.7% |
⇧4% |
|
2010-2015 |
⇩3.6 |
⇩14% |
⇩13.72% |
⇧11.7% |
|
# of patients per year |
Brown code |
Red code |
Green code |
Purple code |
|
2003-2006 |
41.75 |
25 |
21.5 |
2.75 |
|
2007-2008 |
26.82 |
2.5 |
10.3 |
8 |
|
2010-2015 |
28.5 |
|
|
|
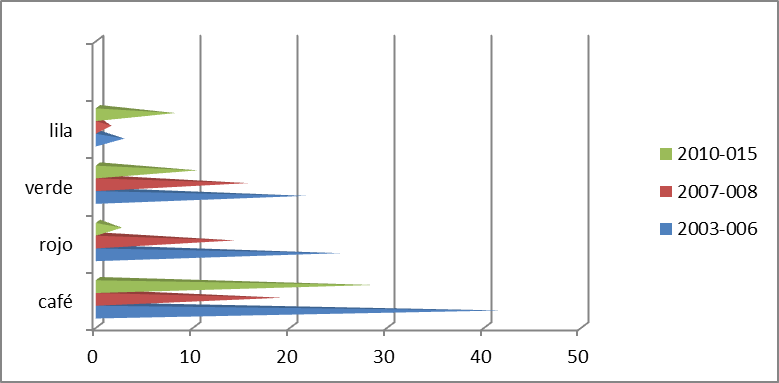
Graph 1. Graph of deaths according to color code per year.
From the reviewed files, 308 deaths were found in the 2010-2015 period. Of this total there were: 244 premature deaths with an annual rate of 40.66 and a monthly rate of 3.38. A total of 64 deaths in term newborns, with an annual number of 10.66 monthly of 0.88 deaths, the annual general death of neonates was 51 and a monthly of 4,277 cases.
In the previous periods we found an annual average of 4,161 births and an average number of annual deaths of 68, up to the year 2006-During the period analyzed, the annual average of births was 3,854 with a death rate of 13.43. The number of annual deaths was 51.
In the previous periods we found an annual average of births of 4161 and number of annual deaths of 68 on average, until the year 2006.
We also found that these results were associated with the number of births per year. Be shows number of births in the following table. And we include in the table, impact on the number of cesarean sections, which was associated with the application of the analysis methodology (Table 4).
|
Year |
2017 |
2018 |
2019 |
2020 |
Annual average |
|
# of births |
32995 |
3159 |
2734 |
2190 |
2844 |
|
# of Cesárean |
1117 |
1330 |
1267 |
788 |
1125.5 |
|
|
Year 2003 |
Year 2004 |
Year 2005 |
Year 2006 |
|
Births |
4611 |
3905 |
3631 |
4500 |
|
# of income |
112 |
904 |
1260 |
1655 |
|
# of Deaths |
50 |
56 |
96 |
70 |
|
Death rate |
10.84 |
11 |
14.3 |
12.2 |
Vulvovaginitis, Premature rupture of membranes, General anesthesia, Transfer of premature infants and newborns, Severe respiratory distress, Obstetric trauma, Maternal urinary tract infection, Persistent low APGAR, Prevalence in males, The age of the mother even with the presence of minors in 23 %, The degree of studies to background in 83%. Delivery care by medical personnel remains in a 14 for inmates; residents 59%.
Frame with high abdominal delivery by last hour of death in first 72 hours of intensive care in 82%, single mothers 21%, Free union 32%, the number of consultation 35.5%, and only 2 consultations 22.5% to 3-5 21%.
Analysis of results
According to the Georgia Method proposed by Dr. Brown, the current analysis shows that more than 88% of Neonatal death cases are located in the area of health of women and pregnant women, which have a very high weight of responsibility for obstetric care, and that must be definitively converted to opportunities for improvement, in the care of the risk group.
The asphyxia found 98% were intrauterine, so they fall under obstetric responsibility, and the number of premature babies, obviously also due to the need to improve the care of women and pregnant women, the same occurs with newborns under 1500gr, in Regarding the septic process, we were struck by the fact that 86% of the newborns also had a history of a maternal infectious process during pregnancy, as can be seen in the number of women, without obstetric care as a rule, and with a history of premature ruptures of membranes, and/or vulvovaginitis, among other factors expressed, and in this study [11-15].
DISCUSSION AND CONCLUSION
We wish to clarify that along with the previous neonatal mortality analysis, an attempt was made to maintain a hospital structure for quality care backed by quality care standards which were severely monitored under the quality management system by the state under the Catastrophic Expenditure system. where the last recertification successfully acquired by the neonatology service was at the end of 2019, obviously it had to be verified that the technical structure of the service was strongly supported, by manuals, service, guides, management, strategies, management, and a whole baggage of technical support, in addition to constantly monitoring the effectiveness in neonatal CPR, and energetic resource management, which in the long run due to non-medical situations were reduced to only 3.3% of supply at the end of 2015, even so it was possible to obtain mention within the first 10 best hospitals in decrease in neonatal death, c However you want, we continued to strengthen essential aspects such as staff training, Human Milk Bank accreditations as a strategy to protect Humanized childbirth, with which we turned the state's attention to delivery care in a convincing manner, promoting greater care in the care of childbirth for example
As we can see, mortality in the period 2010-2015 was reduced by: 40.5%
What is striking is that the population served continues to present practically the same risk factors found in previous analyses, with a large number of these factors that probabilistically should increase death
|
1.-Identification and management |
|
2.-Preconception risk |
|
3.-Obstetric Risk |
|
4.-Prenatal risk |
|
--Identification of preconception risk. |
|
-Antecedentes obstétricos desfaborables |
|
-Unfavorable obstetric history |
|
-Family history |
|
-extreme ages of women |
|
- Nutritional condition |
|
- Exposure to teratogens |
|
-Addictions |
|
-chronic diseases |
|
1.-Prevention |
|
2.-Diagnosis |
|
3.-Reference |
|
4.-Adequate medical management |
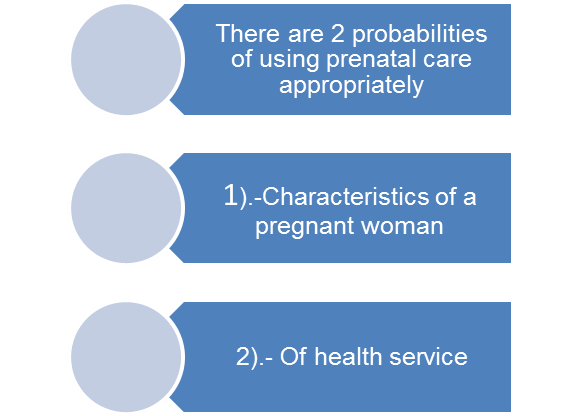
The first considers level of schooling, socioeconomic status, race parity, marital status, and desire to be pregnant, stress, pregnancy problems, the Social Support network, lack of knowledge about the state of pregnancy, during 1st and 4th °
month, birth interval, motivation to seek care, state of depression, availability of transportation, availability of people who care for their children, language and some cultural factors.
Characteristics of health services include:
Accessibility, availability, quality of care provided, attitude of staff receiving patients in medical establishments, satisfaction of health staff working in institutions, as well as "Financing Scheme"
When prenatal care is ensured with these considered, the survival of the newborn will also depend on:
- Weight.
- Age at birth.
- Conditions of Birth [15,16]
As we can corroborate in this study a baby less than 2500 gr. he suffers from a weight deficiency, and according to the WHO this fact alone constitutes a risk to his health. Premature or very low birth weight infants of course they constitute a major public health problem, both in developed countries and in the third world, as they present higher rates of morbidity and mortality, in addition to a great risk of later developing physical, neurological and mental deficiencies [12,17,18].
The analyzes presented here show a clear prevalence of the same risk factors, which are likely to continue as long as no changes are made in the care structure, in the quality of obstetric care and in the health services provided to the population [19-38].
It is urgent to monitor the application of the following factors that tend to limit the high risk for newborns:
- Pregnancy, childbirth and puerperium must be attended by trained and authorized personnel.
- Assess each case individually in the prenatal period, identifying the High risk
- Strengthen prenatal care in the third trimester
- Establish adequate birth plan in advance
- Reduce unnecessary risks
- Adequate surveillance of labor and puerperium
- Document care process
Analyzed period 2010-2015 we found similar conditions than previous analyzes so we urgently suggest to reduce Neonatal death based on 4x4 table strategies proposed by analysis of Georgia Dr. Brown. And that are marked as reproductive health interventions in México. Shoume in this box
CONFLICT OF INTEREST
We do not have any conflict of interest, in the preparation of this study, with companies or other institutions.
CONTRIBUTION
By translating and applying a monitoring method that was initially designed by Dr. Brown to improve women's mortality, and that we transferred to the field of newborn health in a high-demand hospital with few resources for care; In a timeline with continuous monitoring, and application of obstetric surveillance and newborn care standards, a substantial improvement in the quality of obstetric care could be verified, even leading our unit to be Accredited as a BFHI Hospital (Friend of the child and Humanized Birth), translating it into a notable decrease in Neonatal mortality, when we methodically apply surveillance for care under critical links in women's health. The above resulted in mention by the Federal government for the Neonatology service as a Hospital within the first five places in decrease in Neonatal death at the national level in 2016.
REFERENCES
- Norma Oficial Mexicana, para la atención de la mujer durante el embarazo, parto y puerperio y del recién nacido 1995. México, DF: Diario Oficial de la Federación, 1995.
- Colaborating Centered in Reproductive Health the National Centers for Disease Control and Prevention Georgia Department of Human Resource
- Kotelchuck M. (1994). An evaluation of the Kessner Adequacy of Prenatal Care Index and a proposed Adequacy of Prenatal Care Utilization Index. Am J Public Health. 84(9):1414-1420.
- Toan NV, Hoa HT, Trong PV, Höjer B, Persson LA, Sundström K. (1996). Utilisation of reproductive health services in rural Vietnam; are there equal opportunities to plan and protect pregnancies? J Epidemiol Community Health. 50(4):451-455.
- Sen DK, Yusof K, Rajaswari K. (1991). Are three antenatal visits enough for low riskmothers? Singapore J Obstet Gynaecol. 22:83-86.
- Leveno KJ, Cunningham GF, Roark ML, Nelson SD, Williams ML. (1985). Prenatal care Relación entre la mortalidad neonatal y el número de consultas prenatales otorgadas and the low birth weight infant. Obstet Gynecol. 66:599-604.
- Faneite P, Rivera R, Montilla A. (2000). Análisis de la mortalidad perinatal (1993-1997) IIMortalidad Neonatal. Rev Obstet Gineco Venez. 60(2):81-84.
- Vandale S, Rascón-Pacheco RA, Kageyama ML. (1997). Time-trends and causes of infant, neonatal and postneonatal mortality in México, 1980-1990. Salud Public Mex. 39(1):48-51.
- Rangel MN. (2015). Analisis de Mortalidad Neonatal en HGE México.Revista de Perinatología y reproducción humana en NUM 3. 29:90.
- Arredondo A, Meléndez V. (1992). Modelos explicativos sobre la utilización de servicios de salud: revisión y análisis. Salud Publica Mex. 34(1):36-49.
- Ticona M, Huancano D. (2005). Mortalidad perinatal hospitalaria en el Perú: Factores de riesgo. Rev Chil Obstet Ginecol. 70(5):313-317.
- Sánchez-Pérez HJ. (1991). Mortalidad infantil en Tlaxcala, México: ¿Quién tiene mayor riesgo de morir? (Tesis de Maestría en Investigación de Servicios de Salud). México, D.F.: Universidad Nacional Autónoma de México.
- Rodríguez Ye, Velásquez TM y Rois HJ. (1988). Mortalidad perinatal en las unidades de atención médica del IMSS en el Centro Médico Nacional de Torreón. Ginecol Obster Mex. 66:297-300.
- Schwarz R. (1992). Atención prenatal y del parto de bajo riesgo. Publicaciones científicas CLAP No. 1234 OPS/OMS.
- Armas DJ, Shor PV, Mac GC, Karchmer KS. (1977). Factores socioeconómicos en el embarazo de alto riesgo. Ginecol Obstet Mex. 41(247):369-382
- Bortman M. (1998). Factores de riesgo de bajo peso al nacer. Neuquen-Argentina. Rev Pan Am J Public Health. 3(5):314-321.
- Coopland AT, Peddle LT, Basket TF, et al. (1973). A simplified antepartum high-risk screeníng: I Prediction of the high risk neonate. Am J Obstet Gynecol. 117:119.
- General Directorate of Statistics and Informatics of the Ministry of Health. (1997). The principal results of statistics on mortality in Mexico, 1996. Salud Pública Mex. 39(5):486-492.
- Moctezuma Hernández SL, Tene Pérez CE, Aguayo Godínez A, Millán Guerrero R. (2000). Mortalidad perinatal 1 en Colima, Col. Estudio de casos y controles [Perinatal mortality 1 in Colima, Col. Case-control study]. Ginecol Obstet Mex. 68:207-211.
- Wise PH. (2003). The anatomy of a disparity ín infant mortality. Ann Rev Public Health. 24:341-362.
- Vintzileos AM, Ananth CV, Smulian JC, Scorza WE, Knuppel RA. (2002). The impact of prenatal care on neonatal deaths in the presence and absence antenatal hig hrisk conditions. Am J Obstet Gynecol. 186(5):1011-1016.
- Essén B, Bódker B, Sjóberg NO, Langhoff-Roos J, Greisen G, GudmundsonS, et al. (2002). Are some perinatal deaths in inmigrant groups linked to suboptimal perinatal care services? BJOG. 109(6):677-682.
- Rivera L, Fuentes Román Mde L, Esquinca Albores C, Javier Abarca F, Hernández Girón C. (2003). Perinatal mortality associated factorsin a General Hospital of Chiapas, Mexico.Rev Sald Publica. 37(6):687-692.
- Dennis PM, Connell GR, Lacy DG. (1984). Evaluation of the effects of the North Carolina improved pregnancy outcome project: Implication for state-level decision-making. Am J Public Health. 74(6):549-554.
- Showstack JA, Budetti PP, Minkler D. (1984). Factors associated with birth weight: An exploratíon of the roles of perinatal care and length of gestation. Am JPublicHealth. 74(9):1003-1008.
- Joan P, Cooney MA. (1985). What determines the start of prenatal care? Prenatal care, insurance, and education. Med Care. 23(8):986-997.
- Sable RR, Stockbauer JW, Schramm WF, Land GH. (1990). Differentiating the barrier to adequate prenatal care ín Missouri, 1987-88. Public Health Rep. 105(6):549-555.
- Moss NE, Hensleigh PA. (1990). Initiation of prenatal care by adolescents. Associations with social support, stress, and Hispanic ethnicity. J Perinatol. 10(2):170-174.
- Ahmed F, McRae JA, Ahmed N. (1990). Factors associated with not receiving adequate prenatal care in an urban black population: program planning implications. Soc Work Health Care. 14(3):107-123.
- Leatherman J, Blackburn D, Davidhizar R. (1990). How postpartum women explain their lack of obtaining adequate prenatal care. J Adv Nurs. 15(3):256-267.
- Pascoe JM, Milburn M, Haynes K. (1990). Correlates of first trimester care in a public health prenatal clinic. Fam Med. 22(1):25-28.
- Hulka BS, Wheat JR. (1985). Patterns of utilization. The patient perspective. Med Care. 23(5):438-460.
- Vandale S, Rascón-Pacheco RA, Kageyama ML. (1997). Time-trends and causes of infant, neonatal and postneonatal mortality in Mexico, 1980-1990. Salud Publica Mex. 39(1):48-52.
- Cumbre mundial a favor de la infancia. (1991). Declaración mundial sobre la supervivencia, la protección y desarrollo del niño. Washington DC: Organización de las Naciones Unidas.
- Frank R, Pelcastre B, Salgado de Snyder VN, Frisbie WP, Potter JE, Bronfman-Pertzovsky MN. (2004). Low birth weight in Mexico: new evidence from a multi-site postpartum hospital survey. Salud Publica Mex. 46(1):23-31.
- Wilcox AJ. (2001). On the importance--and the unimportance--of birthweight. Int J Epidemiol. 30(6):1233-1241.
- Moreno A, Cano V, García R. (1994). El Riesgo como indicador de necesidad en: Epidemiología Clínica. Segunda Edición. México, Nueva Editorial.-Interamericana. p. 1-6.