Information Links
Related Conferences
Previous Issues Volume 6, Issue 2 - 2023
Curious Case of Obstructive Jaundice: A Case Report
Shaikh Mohd Shaad1, Pathrikar Prathamesh1, Desai Shivani1, Sheth Neil1, Chatterjee Sanjay2,*
General Surgery Resident at Bombay Hospital, Mumbai, Maharashtra, India
Assistant Professor, Maharashtra University of Health Sciences, Nashik Postgraduate Teacher, Bombay Hospital Institute of Medical Sciences, Mumbai, Maharashtra, India
*Corresponding Author: Dr Chatterjee S, Assistant Professor, Maharashtra University of Health Sciences, Nashik Postgraduate Teacher, Bombay Hospital Institute of Medical Sciences, Chamber no. 108, Bombay Hospital Institute of Medical Sciences, Bombay Hospital Avenue, New Marine Lines, Mumbai-400020; Tel: +919322243938; Email: [email protected]
Received Date: May 02, 2023
Publication Date: May 18, 2023
Citation: Shaad SM, et al. (2023). Curious Case of Obstructive Jaundice: A Case Report. Mathews J Surg. 6(2):19.
Copyright: Shaad SM, et al. © (2023)
ABSTRACT
Background: Mirizzi syndrome is defined as common hepatic duct obstruction caused by extrinsic compression from an impacted stone in the cystic duct or infundibulum of the gallbladder. Patients with Mirizzi syndrome can present with jaundice, fever, and right upper quadrant pain. Mirizzi syndrome is often not recognized preoperatively in patients undergoing cholecystectomy and can lead to significant morbidity and biliary injury, particularly with laparoscopic surgery. Summary: Here we present a case of a 53 year old women, known case of hypertension, presented with complaints of abdominal pain, yellowish discoloration of eyes, and fever with chills since 15 days. Clinically, patient was pale, icteric. Tenderness was noted in the right hypochondrium with no guarding/rigidity. Biochemical parameters were suggestive of pancreatitis with deranged ALP, GGTP and Bilirubin values. Ultrasonography was suggestive of a 16 mm calculus at infundibulum. MRCP was suggestive of Acute Oedematous Interstitial Pancreatitis, 16 mm GB calculous causing external compression of CBD with Proximal IHBRD suggestive of Type 1 Mirizzi syndrome. An ERCP with CBD stenting was done and the patient was advised interval cholecystectomy. Intraoperatively during interval cholecystectomy it was revealed to be a Type 3 Mirizzi syndrome. Fundus first approach was used and partial cholecystectomy with transcholecystic retrieval of the stone was done. Conclusion: Laparotomy with Complete Cholecystectomy remains the ideal management of Mirizzi Syndrome. Cases where the Calots Triangle Anatomy is Difficult to define, a Sub-total/partial cholecystectomy is suggested leaving behind a stump of GB or Cystic duct. Laparoscopic Subtotal Cholecystectomy can be safely undertaken for up to type 3 Mirizzi syndrome.
Keywords: Obstructive jaundice, cholelithiasis, Pancreatitis, Mirizzi Syndrome
INTRODUCTION
Mirizzi syndrome is defined as common hepatic duct obstruction caused by extrinsic compression from an impacted stone in the cystic duct or infundibulum of the gallbladder. Patients with Mirizzi syndrome can present with jaundice, fever, and right upper quadrant pain. Mirizzi syndrome is often not recognized preoperatively in patients undergoing cholecystectomy and can lead to significant morbidity and biliary injury, particularly with laparoscopic surgery. The pathophysiological process leading to the subtypes or stages of Mirizzi syndrome, has been explained as an inflammatory phenomenon secondary to a pressure ulcer caused by an impacted gallstone at the gallbladder infundibulum. The impacted gallstone together with the inflammatory response, causes first external obstruction of the bile duct, and eventually erodes into the bile duct evolving into a cholecystocholedochal or cholecystohepatic fistula with different degrees of communication between the gallbladder and bile duct.
CASE REPORT
Patient was a 53 year old female Known case of Hypertension, presented with complaints of, abdominal pain, Yellowish discoloration of eyes, Fever with chills since 15 days. Abdominal Pain was located in right upper abdomen, dull aching, radiating to back, associated with yellowish discoloration of eyes and high grade fever with chills.
On Examination: Patient was averagely built, afebrile, and conscious oriented, Pallor and icterus were present. Oral cavity examination revealed Tobacco stains. Abdomen was soft, No guarding / rigidity, Tenderness was present in Right upper quadrant, No rebound tenderness. Rest of the systemic examination was within normal limits.
Investigations, revealed, raised Serum Amylase and Lipase were raised, a diagnoses of gall stone pancreatitis was made. Other Biochemical Abnormalities included significantly raised ALP, GGTP, S. Bilirubin and liver enzymes.
USG revealed Grade 1 Fatty Infiltration Of Liver, Solitary Gall Bladder Calculi at infundibulum 16 mm in size ; No Peri GB fluid or GB wall thickening, Minimal Biliary Sludge Present. MRCP was suggestive of Acute Oedematous Interstitial Pancreatitis, GB calculi 16 mm in size in infundibulum causing external compression of CBD with proximal IHBRD Type 1 Mirizzi Syndome. ERCP was done with selective CBD Cannulation CBD swept Multiple Times, Cholangiogram done which revealed No filling defects, 10 FR Plastic stent placed in-situ [1-7].
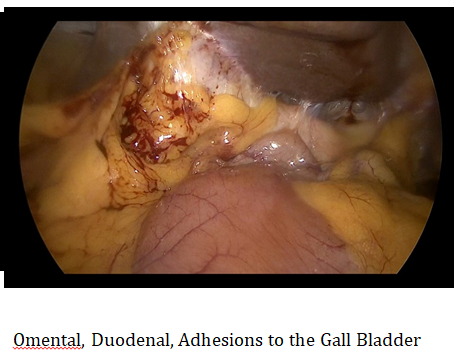
INTRA-OPERATIVE FINDINGS
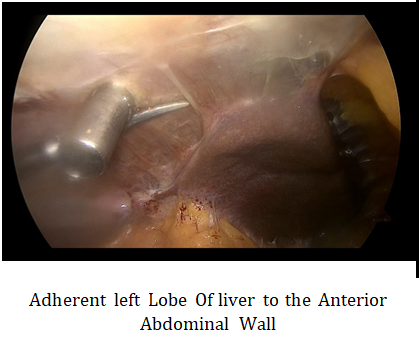
.PNG)
.PNG)
CONCLUSION
Mirrizi Syndrome is a chronic complication of Cholelithiasis which almost always presents with a clinical presentation of Obstructive Jaundice. In this case the initial presentation of the patient was that of Gall stone Pancreatitis along with Obstructive jaundice. In a setting of Acute Pancreatitis, an approach of conservative management was undertaken. Pre-operative Biliary drainage was done with the help of ERCP. ERCP with CBD stent placement plays a crucial role in stemming the tide in an acute setting of obstructive jaundice due to gall stones. Not only does it relieves the obstructed system but also prevents further repeated attacks of pancreatitis in the interval period. Surgical Management of Mirizzi Syndrome remains the Mainstay of its treatment. Interval Cholecystectomy (4-6 weeks later) was advised to the patient. A sub-total cholecystectomy was done laparoscopically and impacted stone was retrieved via the trans-cystic approach. The patient was followed up after 4 weeks for Stent Removal.
The treatment for Mirizzi syndrome is cholecystectomy. Laparoscopic cholecystectomy is preferable, but a more involved surgery may be needed if the condition is advanced. An open cholecystectomy is an option. In cases of a more progressed disease, a partial cholecystectomy can be considered. This would involve leaving Hartman's pouch in place and removing the body of the gallbladder and the gallstones. This will lower the incidence of injury to the porta hepatis and bile ducts. If a fistula is present, then an open cholecystectomy with bilioenteric anastomosis, possibly with a Roux-n-Y, has been shown to be effective.
In patients without fistula formation, the surgical repair and outcome are usually favorable. Due to the distorted anatomy and high rate of conversion to open cholecystectomy for this disease; however, some sources recommend an open surgical approach for all patients affected by Mirizzi syndrome. The prognosis for patients with fistula formation involves prolonged treatment with T-tube placement through the small-moderate sized fistula or biliary diversion with a choledochoduodenostomy or a Roux-en-Y choledochojejunostomy for larger fistulas. A prolonged surgical and hospital course for the latter group of patients increases their risk of complications and increases their morbidity and mortality rate. Gallbladder cancer has been associated with Mirizzi syndrome as well, although this is thought to be due to prolonged inflammation leading to both diseases, rather than a result of Mirizzi syndrome itself [8]. In elderly patients with multiple comorbidities and a high risk of surgical complications, nonoperative methods should be considered to minimize morbidity associated with the surgery. The most common complication of Mirizzi syndrome is cholecystobiliary or cholecysto-enteric fistula formation due to prolonged inflammation. Surgical complications with prolonged procedure time due to dense adhesions may also occur. These include bile duct injury and hemorrhage. Massive hemorrhage during dissection of the Calot triangle can occur in complex cases. Other complications of prolonged inflammation that can be seen in patients with Mirizzi syndrome include:
- Cutaneous fistula formation
- Secondary biliary cirrhosis
- Delayed onset biliary strictures
REFERENCES
- Beltran MA, Csendes A, Cruces KS. (2008). The relationship of Mirizzi syndrome and cholecystoenteric fistula: validation of a modified classification. World J Surg. 32:2237–2243.
- McSherry CK, Ferstenberg H, Virshup M. (1982). The Mirizzi syndrome: suggested classification and surgical therapy. Surg. Gastroenterol. 1:219–225.
- Csendes A, Díaz JC, Burdiles P, Maluenda F, Nava O. (1989). Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg. 76:1139–1143.
- Antoniou SA, Antoniou GA, Makridis C. (2010). Laparoscopic treatment of Mirizzi syndrome: a systematic review. Surg Endosc. 24:33–39.
- Yonetci N, Kutluana U, Yilmaz M, Sungurtekin U, Tekin K. (2008). The incidence of Mirizzi syndrome in patients undergoing endoscopic retrograde cholangiopancreatography. Hepatobiliary Pancreat Dis Int. 7:520–524.
- Piccinni G, Sciusco A, De Luca GM, Gurrado A, Pasculli A, Testini M. (2014). Minimally invasive treatment of Mirizzi's syndrome: is there a safe way? Report of a case series. Ann Hepatol. 13:558–564.
- Kulkarni SS, Hotta M, Sher L, Selby RR, Parekh D, Buxbaum J, et al. (2017). Complicated gallstone disease: diagnosis and management of Mirizzi syndrome. Surg Endosc. 31(5):2215-2222.
- Jones JD, Pawa R. (2017). Single-Operator Peroral Cholangioscopy for Extraction of Cystic Duct Stones in Postcholecystectomy Mirizzi Syndrome. Case Rep Gastrointest Med. 2017:1710501.