Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2022
Case Report: Optical Coherence Tomography, as a Non-Invasive Approach to Evaluate Intracranial Pressure in Normal Pressure Hydrocephalus Patients, as with their Treatment Follow-ups and VP Shunts Reprogramming Procedures
Bita Shalbafan1,*, Seyed Kianoosh Naghibzadeh2, Hajar Aminzadeh3,4, Hossein Lanjanian5,6, Bardia D Baloutch7, Hamid Sajjadi8,9
1Clinical Research Development Center of Labbafinejad Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Biological Sciences, Tarbiat Modares University, Tehran, Iran
3Department of Cognitive Science Studies, Shahid Beheshti University, Tehran, Iran
4Department of Cognitive Modeling, Institute for Cognitive Science Studies, Tehran, Iran
5Molecular Biology and Genetics Department, Engineering and Natural Science Faculty, Istinye University, Istanbul, Turkey
6Cellular and Molecular Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran
7TRUST/FALCON RAY Imaging (X-Ray and Visible Spectrum) Tehran, Iran
8Director, Department of Ophthalmology, Acacia Medical Center, Dubai, UAE
9Director of Neuro-Ophthalmology, San Jose Eye and Laser Medical Center, California, USA
*Corresponding author: Bita Shalbafan, Neurologist, Clinical Research Development Center of Labbafinejad Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; Tel: 00989161119656; Email: [email protected]; [email protected]
Received Date: December 19, 2022
Publication Date: December 31, 2022
Citation: Shalbafan B, et al. (2022). Case Report: Optical Coherence Tomography, as a Non-Invasive Approach to Evaluate Intracranial Pressure in Normal Pressure Hydrocephalus Patients, as with their Treatment Follow-ups and VP Shunts Reprogramming Procedures. Mathews J Neurol. 6(1):020.
Copyright: Shalbafan B, et al. © (2022)
INTRODUCTION
Ventriculoperitoneal Shunts are nowadays a reliable solution to control NPH symptoms and maintain patients’ quality of care by its re-programming ability [1]. However, post VP shunt implementation follow-ups are mostly consisted of clinical reviews that rely on observable signs and symptoms by neurologists Williams M, et al. (2016) [2]. In some conditions though ventricle dilation and cortical atrophy extension may address the demand for VP shut to be re-programed [3]. The presenting case outlines difficulties in evaluating the functionality of the VP shunt for an NPH patient. OCT has been therefore experienced to be a non-invasive low-cost study to assist the neurology practice to lead the patient to VP shunt re-programming, due to its possible low pressure that became authentic during its adjustment procedure.
LITERATURE AND METHOD
As described by National Institute of Neurological Disorders and Stroke (2019) [4], Normal Pressure Hydrocephalus (NPH) could be addressed as the consequence of brain ventricles enlargement and cerebrospinal fluid blockage at spinal cord, due to atypical accumulation of CSF. Magnetic Resonance Imaging (MRI) has reported to be a suitable instrument to diagnose NPH via revealing changes in ventricles volume [5]. It is effective along with additional lab workup [6] and clinical diagnosis such as gait observation and dementia measurement to evaluate NPH and rule out additional Cerebrovascular, Alzheimer and Parkinson related diseases [7]. Ventriculoperitoneal Shunt implementation is considered to be a promising surgical solution, with respect to its programable valve to meet the highest efficiency in ventricles drainage; provoking enhanced control on NPH symptoms [8]. Regardless of recent recommendations on employing MRI, utilized by Diffusion Tensor Imaging (DTI) maps analysis [9]; the reliable method to monitor patients [10] and reprogram the shunt valve has mentioned to be through a combination of clinical observations [11] and pondering on patients’ response to mobility and cognitive routines [12]. Moreover, Afonso A, et al. (2017) [13] performed a study to outline changes in choroidal and retinal thickness within sub-foveal and peripapillary areas as a novel biomarker, being measured by Optical Coherence Tomography.
Although gait ataxia was known as a clinical marker for NPH [14], it comes with similar symptoms to other cerebral diseases, such as Parkinson [15]. To avoid miss-diagnosis though, MR study is usually performed to verify if brain ventricles are experiencing any enlargement [16]. Computed Tomography is likewise the additional modality to make such diagnosis by observing ventricles enlargement and its correlation to cerebral atrophy [7]. Also, lumber puncture (LP) would measure the possible gaining of shunt implementation, while other causes of hydrocephalus have been ruled out through MRI [17]. Hence to primarily diagnose the patient, an MR study have become the reference method of diagnose along with LP to clearly cite that patient suffering from NPH. Thus, the well-established trace for NPH consists of gait apraxia measurement, urinary incontinence observation and examining dementia [18]; the patient planned to be monitored through clinical differential diagnosis, as a reference method for evaluating the significance of employing OCT to measure the improvements driven by the VP Shunt reprogramming. The high-end Topcon OCT employs a longer wavelength utilized by swept source technology to enable tomography to scan beyond retina, even over Bruch’s membrane and specially the Choroid with a substantial quality [19]. Topcon Triton is capable of acquiring B-Scans with the axial resolution of 2.6 microns and 20 microns through the transverse axis (Topcon Healthcare, 2020) [20]. Along with its volumetric data set [21], the device reconstructs the histologic data to a great extent [22]. The mentioned properties have made it a suitable device for diagnostic agreements in this case. Otherwise, Topcon OCT Analysis V 1.18 was used as a software tool to quantitatively export retina layers thickness. Therefore, OCT studies performed simultaneously at each session of clinical review to Monitor retina layers thickness and reprogram the shunt.
CASE REVIEW
A 59 years old male patient walked into neurology practice in 2016, suffering from gait disorder and cognitive impairment, as well as additional signs of Parkinsonism. Meanwhile the mobility malfunction was of an obvious consideration through clinical review, his cognitive behavior was far from mind to be associated with a software engineer, once the neurologist opened dialog. Followed by clinical observations, the patient was referred to paraclinical sector, in order to implement an MR study. The addressed MRI exam was lost by the patient and therefore there had been no access to such record, at the time this study planned to be conducted. However, as it could be additionally observed in his further CT datasets (Figure 1), ventricle enlargement along with cortical atrophy concluded the condition to be mostly associated with NPH. At the meantime though, the lab workup and his family history were in contradiction with neurometabolic maladies. Thus, at the time, research indicated that OCT could be used as a biomarker to diagnose neurological ailment across neuro-ophthalmic findings (as cited in Background Literature), such an exam was simultaneously performed to meet the practice research interests; with respect to his guardian’s eager to go for the mentioned investigation. As long as, the report of that paraclinical study was lost and the ophthalmic center was not equipped with PACS, the baseline OCT is currently absent. However, the Neurology practice medical record registered the indication of an increase in Retina Nerve Fiber Layer (RNFL). According to report comparison with normative database, the RNFL elevation above normal in some areas of Circumpapillary tomogram could likewise verify disturbance in cerebrospinal fluid dynamic. As a result, the patient underwent an LP procedure, where 20mL of his CSF was extracted to balance the cerebrospinal tension, as with forecasting the possible significance of installing a VP shunt to progress with his long-term improvement. A dramatic response to NPH symptoms was recorded by neurologist within his clinical reviews at follow-up sessions, along with an OCT result of a much normal RNFL pattern in comparison with normative database. The situation hence improved until 2018, when a gait disorder relapse was experienced. As long as the patient privileged from VP shunt to control NPH; a peripheral study carried out to evaluate any morbidity regarding his lumber structure through an MR exam. The normal report from radiologist though, made it more difficult to figure out the cause of such conspicuous symptom. The patient was therefore advised to withstand a CT scan from his brain, where even no extensive ventricle enlargement observed to explain the prompted disorder that continued with worsen clinical indications of cognitive impairment. With respect to the coefficient experience of employing OCT for NPH evaluation within his diagnostic history, an OCT exam was fulfilled as the last shot. Abnormalities with repeated increase in RNFL thickness was moreover observed that lead neurologist to ask the VP shunt programming specialist to measure the shunt pressure. 1.5 cm of H2O was measured to be his shunt pressure, where encouraged the practice to ask for its re-programming. Healing signs nevertheless started to appear, along with significant recovery that was recorded in clinical reviews within his follow-up sessions for the next two years. An additional OCT was therefore taken in 2020 as a follow-up measure to check for his condition stability, where no substantial changes were noted.
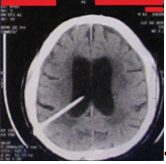
Figure 1: Patient’s CT scan in July 2019.
As long as the baseline OCT observed to be a considerable biomarker, the patient was continuously sent for OCT studies throughout the time, so that the shunt efficiency could be paraclinically logged, next to clinical examinations. The report pasted in Figure 2, indicates the NFL trends from a selective set of consecutive studies from changes in shunt performance within the period of interest for this study, in order to debate on OCT significance for measuring VP Shunt reprogramming and functionality.
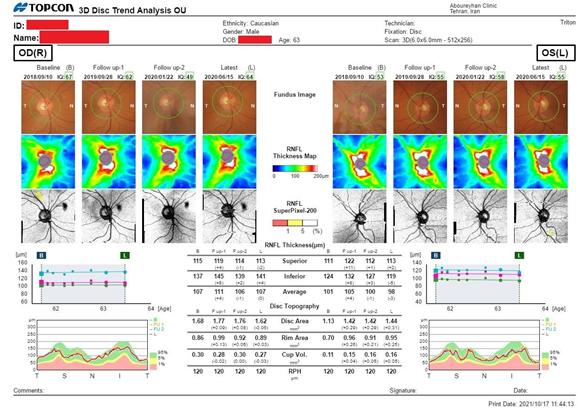
Figure 2: Patient’s NFL Trend Analysis from September 2018 to June 2020.
Chan AW, et al. (2014) [23] debated the phenomenon of age-related thinning, in association with Average Nerve Fiber Layer (ANFL). A study by Parikh RS, et al. (2007) [24] on the other hand, confirms the cited incident, especially with their over 50 years old scope of study. Topcon Medical Systems (2017) [25] reported their study details for Triton’s normative database, where age has been considered as a factor. While pondering on the RNFL Average reflection in the given trend report (Figure 3); change rates are placed within parenthesis to apply such consideration, in order to evaluate NFL thickness with respect to age factor.
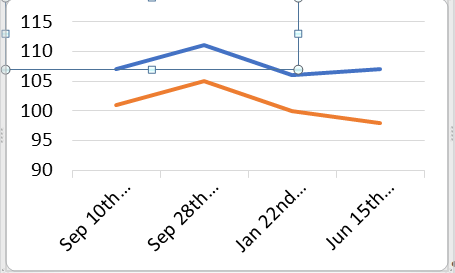
Figure 3: ANFL Trend (in Microns).
The study on September 10th 2018 was arranged here to act as the baseline; when clinical follow-up certified patient’s fine status. The ANFL was reported to be 107 microns for right eye and 101 microns for left eye. About a year after though (September 28th 2019), gait deterioration and cognitive decline was perceived within the clinical review that indicated possible mal-functioning of VP Shunt. Otherwise, the existence of any musculoskeletal conditions was ruled out through lumbosacral imaging, meanwhile a brain CT indicated not much considerable changes to ventricle sizes. The patient was simultaneously undergone an OCT examination, where the right eye ANFL increased to 111 microns, meanwhile his left eye experienced an increase in ANFL to reach 105 microns (4 microns increase bilaterally, considering age thinning). The patient was sent for Shunt reprogramming at that time, once his next follow-up in 3 months (January 22nd 2020) illustrated improvements in his gait apraxia.
Thus, OCT was a paraclinical solution to record each step quantitatively; another study was performed right away. As shown in trend report, his right RNFL was 106 microns thick in average (met 1 micron decrease considering age thinning); whereas his left eye’s ANFL thickness exhibited to be 100 microns (a decrease of 1 micron considering age thinning). His next follow-up in 6 months (June 15th 2020) demonstrated cognitive and gait stability within the clinical review. Otherwise, the executed OCT at the time indicated the ANFL thickness of his right eye to be 107 microns (sustainable, considering age thinning). His left eye though projected an Average NFL thickness of 98 microns (3 microns decrease, considering age thinning) (Figiure 4).
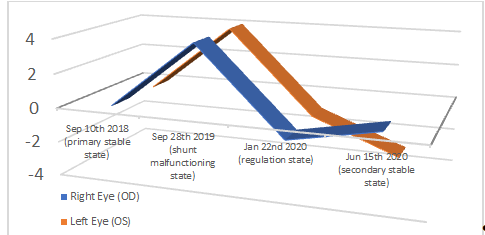
Figure 4: ANFL Trend (Considering Age).
Poster No: P.029, Presenting at The Lancet Summit: Preclinical Neurodegenerative Disease
Being Held in London (QEII Centre) from December 14th to 16th 2021
CONCLUSION, RECOMMENDATION, AND FURTHER WORK
This case report was an example of utilizing Optical Coherence Tomography as a non-invasive approach to measure the functionality of, and reprogramming a Ventriculoperitoneal Shunt, with respect to those effects that Raised Intracranial Pressure (RICP) leaves on RNFL Thickness. Parallel to clinical assessment, OCT verified its capability of diagnosing and monitoring an NPH patient who has been implemented by such an instrument, through a quantitative manner.
This study was limited to Electronic Medical Record (EMR), for which the patient’s primary OCT exam and MR study was missed. A single case report is not moreover as significant as a case series; therefore, further investigation is recommended to study a population of NPH patients, being treated by VP Shunts. This would enhance the significance of OCT applications in diagnosing and treating NPH patients with the addressed solution in a quantitative approach.
Special thanks to the patient who has allowed his medical record to be used, as with kind acknowledgements to Mr. Younes Ashhari for his financial support to NPH and OCT study. Moreover, Mr. Mahdi Bagheri is appreciated for his precise raw data acquisition as the team Optometrist.
REFERENCES
- Limbrick DD Jr, Leonard JR. (2018). Cerebrospinal Fluid Disorders: Lifelong Implications. Springer International Publishing, Germany.
- Williams MA. Malm J. (2016). Diagnosis and Treatment of Idiopathic Normal Pressure Hydrocephalus. Continuum (Minneap Minn). 22(2): 579-599.
- Yamada Sh, Ishikawa M, Yamaguchi M, Yamamoto K. (2019). Longitudinal morphological changes during recovery from brain deformation due to idiopathic normal pressure hydrocephalus after ventriculoperitoneal shunt surgery. Sci Rep. 9(1): 17318.
- National Institute of Neurological Disorders and Stroke. (2019). Normal Pressure Hydrocephalus: Information Page. National Institute of Health.
- Miskin N, Patel H, Franceschi AM, Ades-Aron B, Le A, Damadian BE, et al. (2017). Diagnosis of Normal-Pressure Hydrocephalus: Use of Traditional Measures in the Era of Volumetric MR Imaging. Radiology 285(1): 197-205.
- Wanucha G. (2018). Inventing a Blood Test for Early Detection of Alzheimer’s and Parkinson’s Diseases. Dimensions: The Magazine of the UW Alzheimer’s Disease Research Center. Fall Edition: 22-24.
- Damasceno BP. (2015). Neuroimaging in normal pressure hydrocephalus. Dementia Neuropsychologia. 9(4): 350-355.
- Wu EM, Ahmadieh TYE, Kafka B, Caruso J, Caruso SG, Caruso AR, et al. (2019). Ventriculoperitoneal Shunt Outcomes of Normal Pressure Hydrocephalus: A Case Series of 116 Patients. Cureus. 11(3):e4170.
- Kanno Sh., Saito M., Kashinoura T., Nishio Y., Iizuka O., Kikuchi H., Takagi M., Iwasaki M., Takahashi Sh., Mori E.; 2017. A change in brain white matter after shunt surgery in idiopathic normal pressure hydrocephalus: a tract-based spatial statistics study. Fluids and Barriers of the CNS, V. 14, A. 1.
- Gürer B. (2018). Hydrocephalus: Water on the Brain. IntechOpen, London, United Kingdom.
- Kleinman K., McDaniel L., Molloy M., Johns Hopkins Hospital; 2020. The Harriet Lane Handbook, 22 Edition: South Asia Edition. Elsevier Health Sciences, New Dehli, India.
- Kiefer M, Unterberg A. (2012). The Differential Diagnosis and Treatment of Normal-Pressure Hydrocephalus. Deutsches Ärzteblatt Int. 109(1-2): 15-26.
- Afonso JM, Falcão M, Schlichtenbrede F, Falcão-Reis F, Silva SE, Schneider TM. (2017). Spectral Domain-Optical Coherence Tomography as a New Diagnostic Marker for Idiopathic Normal Pressure Hydrocephalus. Frontiers in Neurol. 8: 172.
- Meier U, Zeilinger FS, Kintzel D. (1999). Signs, symptoms and course of normal pressure hydrocephalus in comparison with cerebral atrophy. Acta Neurochirurgica. 141: 1039-1048.
- Molde K, Söderström L, Laurell K. (2017). Parkinsonian symptoms in normal pressure hydrocephalus: a population‑based study. J Neurol. 264: 2141-2148.
- Oliveira LM, Nitrini R, Román GC. (2019). Normal-pressure hydrocephalus: A critical review. Dementia and Neuropsychologica. 13(2): 133-143.
- Shprecher D, Schwalb J, Kurlan R. (2008). Normal Pressure Hydrocephalus: Diagnosis and Treatment. Curr Neurol Neurosci Rep. 8(5): 371-376.
- Gosh S, Lippa C. (2014). Diagnosis and Prognosis in Idiopathic Normal Pressure Hydrocephalus. Am J Alzheimers Dis Other Demen. 29(7): 583-589.
- Bandello F, Souied EH, Querques G. (2016). OCT Angiography in Retinal and Macular Diseases. Indian J Med Res. 56: 13-17
- Topcon Medical Systems. (2017). Topcon DRI OCT Triton Reference Database Study. National Institute of Health: US National Library of Medicine. NCT03067675.
- Gao SS, Jia Y, Zhang M, Su JP, Liu G, Hwang TS, et al. (2016). Optical Coherence Tomography Angiography. Invest Ophthalmol Vis Sci. 57(9): OCT27-OCT36.
- Michalewska Z, Michalewski J, Nawrocki J. (2013). Going Deeper and Wider: New OCT technologies offer the possibility of imaging the choroid, retina, and vitreous. Retinal Physician. 10: 42-48.
- Chan JW. (2014). Optic Nerve Disorders: Diagnosis and Management. (2nd Ed.) Springer. New York, United States.
- Parikh RS, Parikh SR, Sekhar GC, Prabakaran S, Babu JG, Thomas R. (2007). Normal age-related decay of retinal nerve fiber layer thickness. Ophthalmology. 114(5): 921-926.
- Topcon Medical Systems (2017). Topcon DRI OCT Triton Reference Database Study. National Institute of Health: US National Library of Medicine. NCT03067675.