Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
Assessment of Methylergonovine Induced Side Effects in Postpartum Period
Priya Brahmbhatt1,*, Dharti Pandya1, Almash Memon1, Akshay Shah1, Jatin Patel2, Jignesh Patel1
1Indubhai Patel College of Pharmacy and Research Centre, Dharmaj, Anand, Gujarat-388430, India
2Referral Hospital and Samuhik Aarogya Kendra (Canady Hospital), Khambhat, Anand, Gujarat-388620, India
*Corresponding Author: Priya Brahmbhatt, Indubhai Patel College of Pharmacy and Research Centre, A-5, Maheshwari society, Metpur road, Khambhat, Anand, Gujarat-388620, India; Tel: 9081113417; Email: [email protected]
ABSTRACT
Background: Methylergonovine is a widely used drug in treating and preventing excessive bleeding from the uterus following delivery or caesarean section. There are some significant side effects observed of Methylergonovine in practice. Therefore to improve the patient outcome and to have a better prescribing method, it is necessary to assess the side effects of Methylergonovine. Result: Tachycardia was observed in 67.50% of participants whereas muscle cramp was observed in 17.50% of participants. Approximately 50% of the total participants experienced Nausea and Palpitation. According to the Statistical analysis, no significant difference in all the side effects (Nausea, Vomiting, HTN, Vasoconstriction, Tachycardia, Palpitation, and Muscle Cramps) was found between the primi and multipara groups as the (p-value >0.2050). Conclusion: From the above result, it was found that methylergonovine does not produce any severe and frequent side effects during postpartum periods. Side effects observed are mostly self-treatable and need no intervention. The most frequent side effect observed in this study was tachycardia which was not severe. There was no statistically significant difference between the primi group and the multipara group observed in the side effects after administration of Methylergonovine, so the drug can be used safely in both types of women.
Keywords: Methylergonovine; Post-partum, Side-effects
Abbreviations: HTN: Hypertension; I.V: Intravenous; OR: Odds Ratio
INTRODUCTION
Postpartum hemorrhage is the leading cause of maternal morbidity and mortality worldwide. Pharmacotherapy remains the first-line preventative therapy for postpartum hemorrhage. These therapies may be single (Oxytocin, Carbetocin, Methylergonovine, Ergometrine, Misoprostol, Prostaglandin analog, or Tranexamic acid) or combination therapies, acting in an additive, infra-additive, or synergistic fashion to prevent postpartum hemorrhage. Evidence is strong for the use of Oxytocin, as the first-line uterotonic agent for prevention of postpartum hemorrhage, it is likely the most effective single pharmacologic therapy for prevention of postpartum hemorrhage and need for additional uterotonics. Use of second-line uterotonics such as Methylergonovine, Misoprostol, and Carboprost in combination with Oxytocin has an additive or synergistic effect and a greater risk reduction for postpartum hemorrhage prevention compared with Oxytocin alone. Therefore, combined therapy rather than Oxytocin alone should be advised for preventing postpartum hemorrhage. Tranexamic acid has been found to be both effective and safe for decreasing maternal mortality in women with postpartum hemorrhage, and prophylactic use of tranexamic acid may decrease the need for packed red blood cell transfusions and/or uterotonics [1]. Rigorous studies are lacking, but Methylergonovine and Carboprost are likely superior to Misoprostol. Currently, the choice of second-line agent should be based on their adverse effect profile and patient comorbidities [2]. Ergometrine plus Oxytocin, Carbetocin and Misoprostol plus Oxytocin are more effective uterotonic drug strategies for preventing PPH than the current standard, Oxytocin. Ergometrine plus Oxytocin and Misoprostol plus Oxytocin cause significant side effects. Carbetocin has a favourable side-effect profile, which was similar to Oxytocin [3]. This study provides the result of use of Methylergonovine only in postpartum period to find out its safety and efficacy, as Methylergonovine is widely used during postpartum period. The aim of this study is to assess the side effects of Methylergonovine in the postpartum period. The need of the study is to assess the side effects of Methylergonovine in a postpartum period which will help to improve patient outcomes. This study will help us to assess the side effects of Methylergonovine when used to prevent or treat bleeding from the uterus that can happen after childbirth or an abortion. Thus, it will help the prescribers to have a better prescribing method. It will also help us to know the prescription pattern of Methylergonovine.
METHODS
Study Site
Referral Hospital and Samuhik Aarogya Kendra (Canady Hospital), Khambhat.
Duration of Study
The study was conducted for 3 months after approval from IEC.
Study Design
Cross-sectional Observational Study.
No. of samples collected: 160
The sample size is calculated using COCHRAN’S FORMULA with a standard error of 8% and a confidence interval of 95%.
Sources of Data
- Participant case sheets (Demographic details, history)
- Participant’s laboratory data
- Participant’s vitals before and after drug administration
- Data collection form
Study Criteria
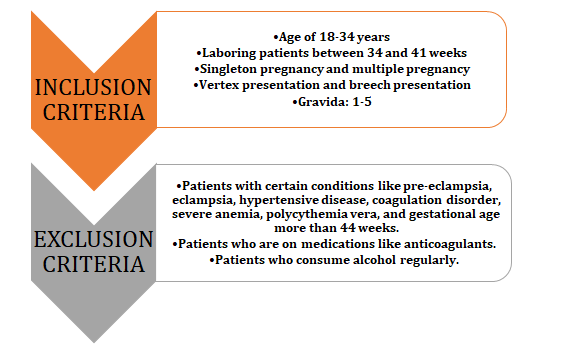
Figure 1.1: Inclusion and Exclusion criteria for the study [4].
Materials Required
- Data Collection form
- Patient Information Sheet
- Informed consent form
Method of Study
A Cross-sectional observational study was conducted, after the approval of the ethics committee of CHARUSAT. The study was conducted at Referral Hospital and Samuhik Aarogya Kendra (Canady Hospital), Khambhat. Participants were screened for the inclusion and exclusion criteria and those who follow the inclusion criteria were included in the study. A detailed history was taken including intrapartum history to collect demographic data and clinical history.
The Gynecologist, after delivery, administered methylergometrine IV 0.2 mg to the participant to prevent excessive bleeding from the uterus. After injecting the drug, the patient was observed for the study. Afterward, side effects were observed by the Gynecologist and the investigators. All the details of the participant were filled in the Case Report Form (CRF) by the investigator.
The information collected was then evaluated and the outcome and the data obtained were analyzed by appropriate statistical method.
Statistical Analysis
The data were entered in Microsoft Excel and were analyzed using GraphPad. Statistical technique used was Fisher’s Exact Test.
RESULTS
Side effects of Methylergonovine were observed during the study. Based on the inclusion and exclusion criteria subjects were recruited in the study. Total there were 160 subjects included in the study. Out of which, 77 participants were in the primi group and 83 participants were in the multipara group.
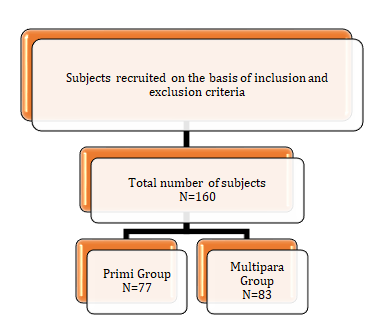
Figure 1.2: Subjects recruited [49].
According to this study, there was a total of 160 participants (women) who were administered Methylergonovine. There were 75 (46.87%) women who experienced Nausea. Side effect of Vomiting was observed in 61 (38.12%) women out of 160. Moreover, 52 (32.50%) women had experienced HTN. The side effect of Vasoconstriction was observed in 97 (60.62%) women. The participants who experienced side effects of Tachycardia, Palpitation, and Muscle cramps were 108 (67.50%), 84 (52.50%) and 28 (17.50%) respectively. Overall, there was the highest ratio (67.50%) of participants who experienced Tachycardia whereas the lowest ratio (17.50%) of side effects was Muscle Cramps.
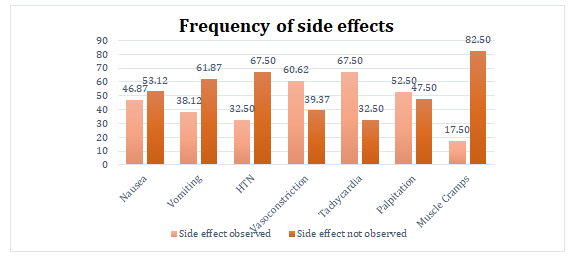
Graph 1.1: Frequency of side effects of Methylergonovine.
Comparison of Nausea observed between Primi and Multipara groups
In the primi group, there were 77 women whereas in the multipara group there were 83 women. Firstly, in the primi group, Nausea was observed in 39 (50.65%) women while participants who did not experience Nausea were 38 (49.35%). Furthermore, the participants who experienced Nausea were 36 (43.37%) in the multipara group whereas the remaining participants who did not experience it were 47 (56.63%).
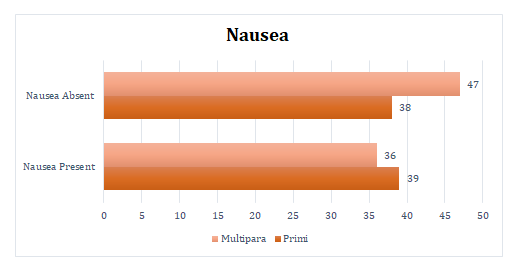
Graph 1.2: % of Participants experienced and did not experience Nausea in Primi and Multipara groups.
Comparison of Vomiting observed between Primi and Multipara groups
On analysis and comparing both of the groups, 28 (36.36%) women suffered from vomiting out of 77 in primi group and 33 (39.76%) women suffered from vomiting out of 83 in multipara group. Overall, in both groups, the ratio of participants who did not experience vomiting was higher.
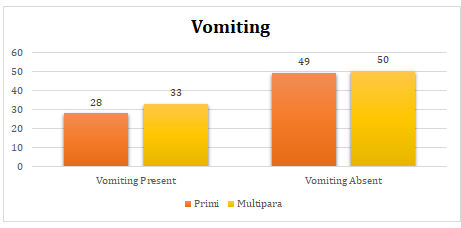
Graph 1.3: % of Participants experienced and did not experience Vomiting in Primi and Multipara groups.
Comparison of HTN observed between Primi and Multipara groups
The data analyzed the ratio of participants who experienced HTN were 24 (31.17%) and 28 (33.73%) in primi and multipara groups respectively. The patient who did not experience HTN were 53 (68.83%) in the primi group and 55 (66.27%) in the multipara group.
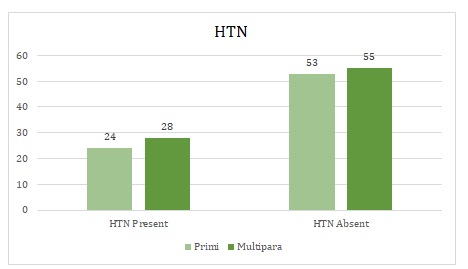
Graph 1.4: % of Participants experienced and did not experience HTN in Primi and Multipara groups.
Comparison of Vasoconstriction observed between Primi and Multipara groups
The side effect of Vasoconstriction was observed in 48 (62.34%) in the primi group and 49 (59.04%) in the multipara group, while in the primi group, exactly 29 (37.66%) of participants who did not experience it and in the multipara group it was 34 (40.96%).
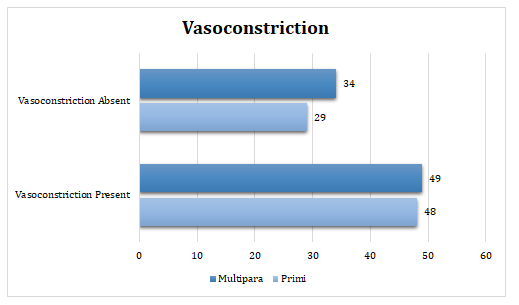
Graph 1.5: % of Participants experienced and did not experience Vasoconstriction in Primi and Multipara groups.
Comparison of Tachycardia observed between Primi and Multipara groups
In the primi group, Tachycardia was observed in 50 (64.94%) women while participants who did not experience Tachycardia were 27 (35.06%), whereas, in the multipara group, Tachycardia was observed in 58 (69.88%) women while participants who did not experience Tachycardia were 25 (30.12%).
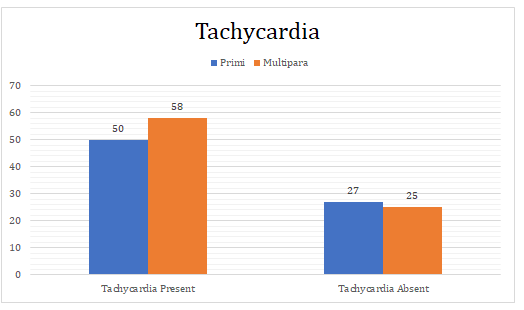
Graph 1.6: % of Participants experienced and did not experience Tachycardia in Primi and Multipara groups.
Comparison of Palpitation observed between Primi and Multipara groups
Participants who had experienced Palpitation in primi and multipara groups were 36 (46.75%) and 48 (57.83%) respectively. On the other hand, in the primi group, 41 (53.25%) of participants did not experience Palpitation and in the multipara group, it was 35 (42.17%).
Graph 1.7: % of Participants experienced and did not experience Palpitation in Primi and Multipara groups.
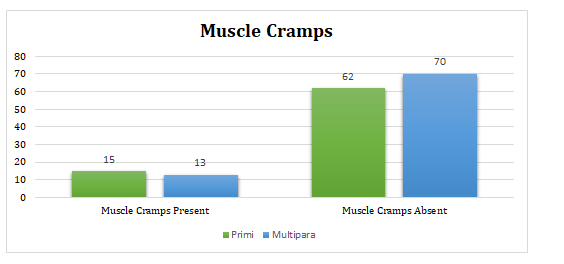
Comparison of Muscle Cramps observed between Primi and Multipara groups
From the graph, it has been observed that most of the women did not experience muscle cramps which were 80.52% in the primi group and 84.34% in the multipara group. Oppositely, the participants who experienced muscle cramps in primi and multipara groups were 19.48% and 15.66% respectively.
Graph 1.8: % of Participants experienced and did not experience Muscle Cramps in Primi and Multipara groups.
DISCUSSION
The frequency of side effects of Methylergonovine was assessed during this study. Comparison of side effects of Methylergonovine was analyzed between the primi and multipara groups. A total of 160 women were included in this study. Commonly observed side effects of Methylergonovine were Nausea, Vomiting, HTN, Vasoconstriction, Tachycardia, Palpitation, and Muscle Cramps.
The comparison of side effects of Methylergonovine between primi and multipara groups was done by Fisher’s exact test using GraphPad software. The statistical technique used was an independent two-tailed Fisher’s exact test.
According to this study, there was a total of 160 participants (women) who were administered Methylergonovine. There was the highest ratio (67.50%) of participants who experienced Tachycardia whereas the lowest ratio (17.50%) of side effects was Muscle Cramps. Approximately 50% of the total participants experienced Nausea and Palpitation.
There was no statistical difference in the side effects observed between both the groups as the p-value for all the side effects was greater than 0.05. The p-value for Nausea was 0.4283, the p-value for Vomiting was 0.7450, the p-value for HTN was 0.7390, the p-value for Vasoconstriction was 0.7466, the p-value for Tachycardia was 0.6126, the p-value for Palpitation was 0.2050 and the p-value for Muscle cramps was 0.5403.
Relative risk is a ratio of the probability of an event occurring in the exposed group versus the probability of the event occurring in the non-exposed. Thus relative risk provides an increase or decrease in the likelihood of an event based on some exposure. Relative risk is applied to populations with different disease prevalence. The Relative Risk does not specify the absolute risk of the event occurring [5].
An odds ratio (OR) is a measure of association between an exposure and an outcome [4]. OR > 1 means greater odds of association with the exposure and outcome. OR = 1 means there is no association between exposure and outcome. OR < 1 means there is a lower odds of association between the exposure and outcome [6].
Relative risk was computed using Koopman’s asymptotic score. The Relative risk for Nausea, Vomiting, HTN, Vasoconstriction, Tachycardia, and Muscle cramps was found to be 1.168, 0.9146, 0.9239, 1.056, 0.9292, and 1.244 respectively.
The Odds ratio was computed using Baptista-Pike. The Odds ratio for Nausea, Vomiting, HTN, Vasoconstriction, Tachycardia, and Muscle cramps was found to be 1.340, 0.8658, 0.8895, 1.148, 0.7982, and 1.303 respectively. The Odds ratio >1 indicates there is an association between the exposure and the outcome.
The Relative risk and Odds ratio Palpitation was found to be the lowest i.e. 0.8084 and 0.6402 respectively. The Odds ratio <1 indicates there is less association between the exposure and the outcome.
CONCLUSION
Methylergonovine can be used as a safe and effective alternative agent in the active management of the third stage of labor in the caesarean section. From the above result, it was found that methylergonovine does not produce any severe and frequent side effects during postpartum periods. Side effects observed are mostly self-treatable and need no intervention. The most frequent side effect observed from this study was Tachycardia which was not severe. There was no statistically significant difference between the primi group and the multipara group observed in the side effects after administration of Methylergonovine, so the drug can be used safely in both types of women after delivery. Further evaluation is needed to compare this drug with another choice of drug to decide the first choice of drug to treat and prevent excessive bleeding from the uterus with better efficacy and safety.
AUTHOR CONTRIBUTIONS
Priya Brahmbhatt- She prepared the CRF, analysed the result by appropriate statistical analysis and concluded the research. Also she prepared the manuscript of article.
Dharti Pandya- She collected the data and filled the CRF. Also she calculated the result figures from the Data Collection Form to apply statistical test and analyse the result.
Almash Memon- He collected the Data and filled the CRF.
Dr. Akshay Shah- He was the mentor and advisor of the entire research. His guidance helped us a lot all the time in the research. The research would not have landed at the conclusion without the participation of Dr. Akshay Shah.
Dr. Jatin Patel- He guided us in selecting the title of this research and to help and support us throughout the research in the hospital.
Mr. Jignesh Patel- He did analysis of the data and its statistical computation and landed us to a final results and conclusion.
Why this work is appropriate for Scientific Reports?
As the title indicates the purpose of the research is to assess the side effects of Methylergonovine in the postpartum period, so our research concludes that Methylergonovine does not produce any severe and frequent side effects during postpartum periods. There was no statistically significant difference between the primi group and the multipara group observed in the side effects after administration of Methylergonovine, so the drug can be used safely in both types of women after delivery. So the results show the gynaecologists to safely use Methylergonovine to treat Uterine bleeding after delivery.
REFERENCES
- Jones AJ, Federspiel JJ, Eke AC. (2023). Preventing postpartum hemorrhage with combined therapy rather than oxytocin alone. Am J Obstet Gynecol MFM. 5(2S):100731.
- Balki M, Wong CA. (2021). Refractory uterine atony: still a problem after all these years. Int J Obstet Anesth. 48:103207.
- Gallos I, Williams H, Price M, Pickering K, Merriel A, Tobias A, et al. (2019). Uterotonic drugs to prevent postpartum haemorrhage: a network meta-analysis.
- Szumilas M. (2010).Explaining odds ratios. J Can Acad Child Adolesc Psychiatry. 19(3):227-229.
- Tenny S, Hoffman MR. (2023). Odds Ratio. StatPearls; StatPearls Publishing.
- Smith C. (2018). Idiot’s guide to odds ratios.