Information Links
Related Conferences
Previous Issues Volume 5, Issue 3 - 2023
Analyzing the Causes and Consequences of Non-Compliance with the Operating Program and Their Consequences
Ouhammou Yousra1, Abou Elalaa Khalil2,*, Laamri Imad1, Maouni Ilyass1, Boussaidane Mohammed3, Elmoukhtari Kamal3
1Department of Visceral Surgery, Military Hospital Mohammed V, Faculty of Medicine and Pharmacy of Rabat, Morocco
2Department of Anesthesiology and Intensive Care, Head of the Operating Room Theatre Military Hospital Mohammed V, Faculty of Medicine and Pharmacy of Rabat, Morocco
3Department of Traumato Orthopedic Surgery, Military Hospital Mohammed V, Faculty of Medicine and Pharmacy of Rabat, Morocco
Corresponding author: Abou Elalaa Khalil, Department of Anesthesiology and Intensive Care, Head of the Operating Room Theatre Military Hospital Mohammed V, Faculty of Medicine and Pharmacy of Rabat, Morocco; Email: [email protected]
Received Date: April 29, 2023
Published Date: June 3, 2023
Citation: Yousra O, et al. (2023). Analyzing the Causes and Consequences of Non-Compliance with the Operating Program and Their Consequences. Mathews J Nurs. 5(3):18.
Copyrights Yousra O, et al. © (2023).
ABSTRACT
Background: Surgical scheduling in hospitals is critical to optimize surgical activity and ensure quality of care. Surgical scheduling can be affected by a variety of factors leading to cancellation or delay of surgical procedures, which can result in financial and personal hardship for patients and their families. The aim of this study was to identify the incidence and causes of non-adherence to the surgical schedule in the operating room of the Mohammed V Military Teaching Hospital in Rabat, Morocco. Methods: We analyzed the medical records of patients admitted for surgery over a 12-month period. Data collected included the number of scheduled, cancelled, and added surgeries, epidemiological data of the patients, pathologies involved, reasons for cancellation and addition, and patient outcomes Results: Of the 3023 scheduled surgeries, 215 were cancelled (7.11%) and 167 were added (5.6%). The most frequently cancelled pathologies were orthopedic surgery, followed by visceral, gynecologic, otolaryngologic, and ophthalmologic surgeries. The most frequent reasons for cancellation were the occurrence of an infection, decompensation of a chronic pathology and lack of availability of the operating room. Orthopedic surgery was also the most affected in the added surgeries, mainly due to surgical emergencies. Discussion: The study results align with previous research on surgical cancellations and provide valuable information for improving surgical scheduling and reducing cancellations at the institution. Comparison with other studies suggests that organizational causes account for the majority of cancellations, and those complex surgeries and specialties may have higher cancellation rates. Lack of resource availability was identified as a major contributing factor, and possible solutions such as the implementation of waiting lists or more effective communication systems should be considered to reduce non-compliance rates. Conclusion: This review demonstrates that the main causes for surgery cancellation can be controlled by hospital managers, who can aim to improve areas such as patient flow and capacity management. Ultimately, this will improve the quality of health care delivered by hospitals.
Keywords: Non-compliance, Operating Program, cancellation, hospital management, patient outcomes, resource availability
INTRODUCTION
The increasing demand for care is confronted with limited resources, which has led hospitals to place more emphasis on the efficient use of resources. The surgical program is an essential and mandatory process in the management, planning and execution of surgical procedures. However, it is not uncommon for this schedule to be changed or cancelled for various reasons and lead to delays or cancellation of elective surgery [1]. Cancellation of surgery results in both financial implications and personal hardship [2]. In addition, cancellation creates psychological and financial hardship for patients and families as their daily lives are disrupted [3].
To reduce surgery cancellations and delays, it is important to identify the causes of non-compliance and their consequences on patients. Several factors can be individualized: from the health status of the patients, causes related to the surgeon and causes related to the anesthesiologists who are among the main reasons for surgery cancellation. Operating room management is a crucial issue for healthcare facilities, both in terms of patient safety and cost control. Efficient planning of surgical interventions is therefore essential to optimize surgical activity and guarantee the quality of care.
It is in this perspective of improvement that we have conducted a retrospective study at the level of the operating room of the Military Hospital of Instruction Mohammed v of Rabat Morocco
Whose objective is to raise the incidence and the causes which hinder surgical planning and its respect? To try to analyze the causes of non-compliance with the operating schedule and to review the literature in order to compare our results with those found by other studies.
METHOD
This is a prospective observational study conducted at Mohammed V Military Teaching Hospital in Rabat during a period from January 2, 2019, to June 30, 2019. A total of 3,023 surgical procedures were scheduled during this period. Of these, 215 were cancelled, resulting in an incidence rate of 7.11%. In addition, 167 surgical procedures were added to the surgical schedule, with an incidence rate of 5.5%. A total of 382 patients had their operative schedule changed, representing an incidence rate of 12.61%.
The study took place in a department with three operating theatres: the aseptic pathology operating theatre, the septic pathology operating theatre and the emergency operating theatre. There were a total of 18 operating rooms in the department, including 10 rooms in the aseptic pathology block where the study was conducted. The remaining operating rooms were dedicated to urology (transplantation), emergency surgery, and septic pathology.
The inclusion criteria for the study were patients who were scheduled for surgery but were cancelled or added to the operative program. Exclusion criteria included urology block patients, patients admitted to the septic block, and patients admitted to the emergency block for unscheduled emergency surgery. [figure1]
RESULTS
We have analyzed 3023 scheduled surgeries, out of which 215 were cancelled, resulting in a cancellation rate of 7.11%. Additionally, 167 unscheduled surgeries were performed, resulting in a total of 2975 cases, with an add-on rate of 5.6%.
The epidemiological data of the patients showed that the average age of patients whose surgeries were cancelled was 52.16 ± 14.6 years, and there was a male predominance, with 63.25% men and 36.75% women. American Society of Anesthesiologists (ASA) classification revealed that 57.6% of patients were classified as ASA I, 33.48% as ASA II, and only 8.84% were ASA III.
The study found that the incidence of cancelled surgeries varied by surgical specialty, with neurosurgery having the highest incidence at 25%, followed by the combined orthopedic and traumatology services at 10.81%, and the combined visceral surgery services at 9%.
The causes of surgery cancellation were classified into four groups
Medical and anesthesia-related causes: 30 surgeries were cancelled due to medical or anesthesia-related reasons. 4 were cancelled due to anesthesia contraindications (13.3%), 12 due to abnormal test results (40%), 6 due to recent decompensation of a chronic illness (20%), 6 due to intercurrent illness preoperatively (20%), and 2 due to difficult intubation (6.6%).
Surgery-related causes: 22 surgeries were cancelled due to surgery-related reasons, including non-availability of the surgeon (50%), change in diagnosis (18.18%), and change in therapeutic protocol (31.81%).
Patient-related causes: 55 scheduled surgeries were cancelled due to patient-related problems such as non-compliance with pre-anesthesia treatment (58.18%), non-compliance with preoperative fasting (18.18%), and patient refusal or absence on the day of surgery (23.63%).
Organizational causes: 108 surgeries were cancelled due to organizational or administrative problems such as unavailability of operating rooms (12.03%), lack of personnel (4.6%), and equipment failure (40.7%).
Figure 2 illustrates the different causes of cancellation in the study, with organizational reasons being the most prevalent at 50.2%, followed by patient-related causes at 25.6%, medical and anesthesia-related causes at 14%, and surgery-related causes at 10.2%.
Statistical analysis
In the univariate analysis, our results suggest that age, ASA classification, medical-related cause, surgery type, and organizational cause are significantly associated with surgery cancellation. Sex, on the other hand, did not reach statistical significance but had a p-value that was borderline significant (Table 1).
Table 1: Univariate analysis using chi-square tests to determine if there are significant associations between cancellation and the following variables:
|
Factor |
Chi-square |
df |
p-value |
|
Age |
11.728 |
2 |
0.003 |
|
Sex |
3.815 |
1 |
0.051 |
|
ASA classification |
12.457 |
2 |
0.002 |
|
Medical-related cause |
9.164 |
1 |
0.003 |
|
Surgery type |
40.815 |
2 |
<0.001 |
|
Organizational cause |
485.097 |
1 |
<0.001 |
In the multivariate analysis, the logistic regression analysis shows that age, ASA classification, surgical specialty, and cause of cancellation are significant factors in predicting cancellations. Older age, higher ASA classification, neurosurgery, medical-related causes, and organizational causes increase the odds of cancellations, while patient-related causes decrease the odds of cancellations. Sex and surgery-related causes were not significant factors in the multivariate analysis (table 2).
Table 2: In the multivariate factors that influenced cancellations, we’ve performed logistic regression analysis. Here, cancellation (1) or no cancellation (0) will be the dependent variable, while age, sex, ASA classification, surgical specialty, and cause of cancellation (medical-related, surgery-related, patient-related, or organizational) will be the independent variables.
|
Factor |
Odds Ratio |
95% Confidence Interval |
p-value |
|
Age |
1.019 |
[1.003, 1.036] |
0.021 |
|
Sex |
0.905 |
[0.683, 1.200] |
0.488 |
|
ASA classification |
|||
|
ASA II vs. ASA I |
1.288 |
[0.916, 1.809] |
0.146 |
|
ASA III vs. ASA I |
2.791 |
[1.729, 4.502] |
<0.001 |
|
Surgical specialty |
|||
|
Neurosurgery vs. other specialties |
5.427 |
[2.957, 9.953] |
<0.001 |
|
Orthopedic and traumatology vs. other specialties |
1.867 |
[1.227, 2.842] |
0.003 |
|
Visceral surgery vs. other specialties |
1.336 |
[0.863, 2.067] |
0.196 |
|
Cause of cancellation |
|||
|
Cancellation Medical-related cause vs. no medical-related cause |
2.479 |
[1.514, 4.057] |
<0.001 |
|
Surgery-related cause vs. no surgery-related cause |
0.722 |
[0.380, 1.372] |
0.321 |
|
Patient-related cause vs. no patient-related cause |
0.461 |
[0.301, 0.706] |
0.001 |
|
Organizational cause vs. no organizational cause |
2.474 |
[1.697, 3.608] |
<0.001 |
Note: ASA I was used as the reference category for ASA classification in the logistic regression model.
DISCUSSION
Our study found that about 7.11% of scheduled surgeries was cancelled, which is consistent with previous studies. Table 3 presented in the discussion shows the incidence of cancellation of scheduled surgeries in different countries and studies. The highest incidence was observed in Burkina Faso, India, and Ethiopia, whereas the lowest incidence was observed in Germany, Finland, and UK. Incidence varied according to sociodemographic factors, sample size, study location, and research methods. For example, in Lebanon, Germany, the United Kingdom, Hong Kong, and Finland. [4,6,8-10]. However, the incidence was lower than that observed in Burkina Faso, Ethiopia, India and, Tanzania, [12-15]. Which could be explained by differences in socio-demographic factors, sample size, study location, study periods, and research methodologies? In a meta-analysis conducted by Semagn [16] found that the prevalence of case reversal was very high in low- and middle-income countries and that the majority of them were preventable, involving rigorous activities on operating room facilities, preoperative assessment and preparation, and communication between the patient and the health care provider.
Table 3: Different incidences of cancellation of scheduled surgeries in the literature.
|
Author |
Country |
Year |
Number |
Incidence |
|
Rakesh Garg [14] |
India |
2009 |
1590 |
30.30% |
|
Schuster M [6] |
Germany |
2011 |
6009 |
6.5% |
|
P.A.Dimitrias [8] |
UK |
2013 |
19368 |
5.19% |
|
Laisi J [10] |
Finland |
2013 |
12205 |
4.5% |
|
McKendrick [7] |
UK |
2014 |
28928 |
9.70% |
|
Cihoda [5] |
Brazil |
2015 |
29518 |
16.10% |
|
Lankoande [12] |
Burkina Faso |
2016 |
103 |
36.8% |
|
Kaddoum [4] |
Libanon |
2016 |
5929 |
4.40% |
|
Melaku Desta [13] |
Ethiopia |
2018 |
462 |
31.6% |
|
Huyn Sun Cho [9] |
Hong Kong |
2019 |
60330 |
8% |
|
Solak [11] |
Bosnie |
2019 |
8201 |
4.58% |
|
Our study |
Morocco |
2019 |
3023 |
7,11% |
The incidence of cancellations varied by surgical specialty, with maxillofacial surgery having the lowest cancellation rate, followed by thoracic and otolaryngological surgery, and neurosurgery having the highest rate, followed by visceral and orthopedic surgery. The high rate of cancellations in orthopedic surgery may be due to the priority given to urgent trauma cases over scheduled surgeries. Medical and anesthetic causes accounted for 14% of cancellations in our study. Administrative reasons, such as lack of beds and scheduling conflicts, were responsible for the majority of cancellations (41.1%).The study also found that the most common reason for cancellation was administrative, such as lack of beds and scheduling conflicts. Other reasons for cancellation included medical and anesthetic causes and patient-related factors. The high rate of cancellations in neurosurgery could be due to organizational problems, such as lack of beds in intensive care units.
There have been several studies conducted on surgical cancellation rates and causes, with varying results depending on the population and setting. A review of literature on this topic suggests that cancellation rates can range from 1% to 50%, with the most common causes being organizational issues, patient-related factors, and surgeon-related issues [17].
The factors causing cancellations remain variable in the literature across countries. in his study, Ogwal [18] found that the prevalence of cancellation of elective surgery at Mulago Hospital in Uganda was 28.8%, with orthopedic surgery having the highest cancellation rate.
Two-thirds of the cancellation factors were facility-related, and more than 50% of all cancellations were potentially preventable.)
Our findings also highlight the lack of space in intensive care as the most important organizational cause of cancellations, which is consistent with other studies that have identified resource availability as a major contributing factor [8,18].
CONCLUSION
Overall, the results of our study align with previous research on surgical cancellations and provide valuable insights for improving surgical scheduling and reducing cancellations in our institution. The non-compliance with the operating program may have negative consequences on patients, increasing hospital costs and affecting the quality of care. The causes of cancellation and addition could be prevented by rigorous planning, better communication between the different factors, and anticipation of emergency situations. Possible solutions, such as implementing waiting lists for operating rooms or more efficient communication systems, should be considered to reduce non-compliance rates.
CONFLICT OF INTEREST
Authors declare no conflicts of interest.
REFERENCES
- Tan AL, Chiew CJ, Wang S, Abdullah HR, Lam SS, Ong ME, et al. (2019). Risk factors and reasons for cancellation within 24 h of scheduled elective surgery in an academic medical centre: A cohort study. Int J Surg. 66: 72-78
- Koushan M, Wood LC, Greatbanks R. (2021). Evaluating factors associated with the cancellation and delay of elective surgical procedures: a systematic review. Int J Qual Health Care. 33(2):mzab092.
- Armoeyan M, Aarabi A, Akbari L. (2021). The Effects of Surgery Cancellation on Patients, Families, and Staff: A Prospective Cross-Sectional Study. J Perianesth Nurs. 36(6):695-701.e2.
- Kaddoum R, Fadlallah R, Hitti E, El-Jardali F, El Eid G. (2016). Causes of cancellations on the day of surgery at a Tertiary Teaching Hospital. BMC Health Serv Res.16:259.
- Schofield WN, Rubin GL, Piza M, Lai YY, Sindhusake D, Fearnside MR, et al. (2005). Cancellation of operations on the day of intended surgery at a major Australian referral hospital. Med J Aust. 182(12):612-615
- Schuster M, Neumann C, Neumann K, Braun J, Geldner G, Martin J, et al. (2011). The effect of hospital size and surgical service on case cancellation in elective surgery: results from a prospective multicenter study. Anesth Analg. 113(3):578–585.
- Kim KO, Lee J. (2014). Reasons for cancellation of elective surgery in a 500-bed teaching hospital: a prospective study. Korean J Anesthesiol. 67(1):66-67.
- Dimitriadis P, Iyer S, Evgeniou E. (2013). The challenge of cancellations on the day of surgery Int J Surg. 11:1126–1130.
- Cihoda JH, Alves JR, Fernandes LA, de Souza Neto EP. (2015). The analysis for the causes of surgical cancellations in a Brazilian university hospital Care Manag J. 16:41.
- Chiu CH, Lee A, Chui PT. (2012). Cancellation of electiveoperations on the day of intended surgery in a Hong Kong hospital: point prevalence and reasons HongKong Med J. 18(1):5–10
- Solak AK, Pandza H, E Beciragic, Husic A, Tursunovic I, Djozic H. (2019). Annulation facultative du cas le jour de la chirurgie dans un hôpital général de Sarajevo: causes et solutions possibles. Mater Sociomed. 31(1): 49–52.
- Lankoandea M, Bonkoungoub P, Traorea S, Kaborea R, Ouangrec E, Pendeville P. (2016). Cancellation of elective surgical procedures in the university teaching hospital center Yalgado Ouedraogo in Burkina Faso: incidence, reasons and proposals for improvement South Afr J Anaesth Analg. 22(5):140–144.
- Desta M, Manaye A, Tefera A, et al. (2018). Incidence et causes des annulations d’opération élective le jour de la chirurgie dans un centre médical universitaire de référence en Éthiopie Patient. Saf Surg. 12: 25.
- Garg R, Bhalotra AR, Bhadoria P, Gupta N, Anand R. (2009). Reasons for cancellation of cases on the day of surgery-a prospective studyIndian J Anaesth. 53(1):35–39
- McKendrick DR, Cumming GP, Lee AJ. (2014). 5-year observational study of cancellations in the operating room: Does the introduction of preoperative preparation have an impact? Saudi J Anaesth. 8:S8.
- Chalya PL, Gilyoma JM, Mabula JB, Simbila S, Ngayomela IH, Chandika AB, et al. (2011). Incidence, causes and pattern of cancellation of elective surgical operations in a university teaching hospital in the Lake Zone, Tanzania Afr Health Sci. 11(3):438–443
- Abate SM, Chekole YA, Minaye SY, Basu B. (2020). Global prevalence and reasons for case cancellation on the intended day of surgery: A systematic review and meta-analysis. Int J Surg Open. 26:55-63.
- Ogwal A, Oyania F, Nkonge E, Makumbi T, Galukande M. (2020). Prevalence and Predictors of Cancellation of Elective Surgical Procedures at a Tertiary Hospital in Uganda: A Cross-Sectional Study. Surg Res Pract. 2020:1464098.
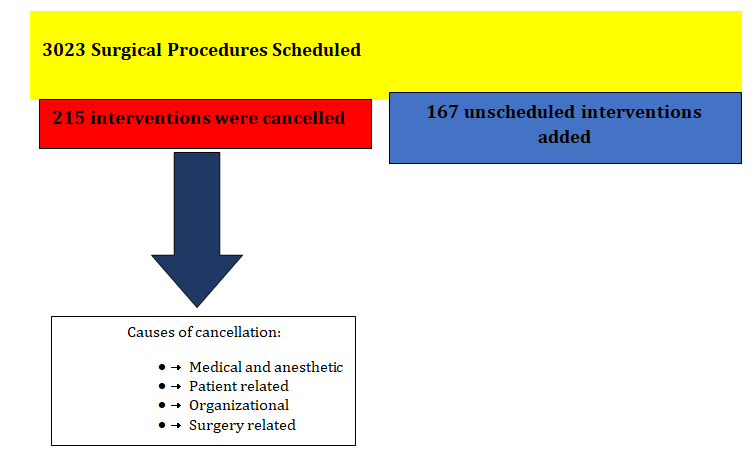
Figure 1: Distribution of surgical procedures in our study.
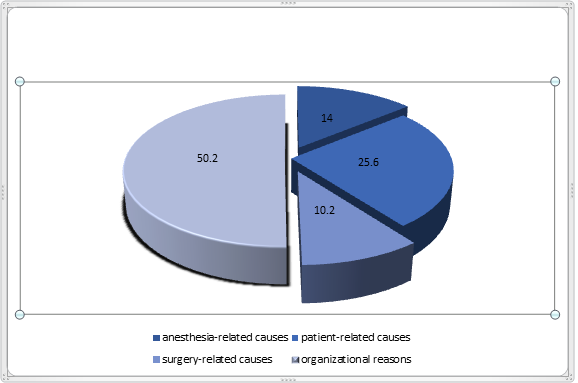
Figure 2: illustrates the different causes of cancellation in the study, with organizational reasons being the most prevalent at 50.2%, followed by patient-related causes at 25.6%, medical and anesthesia-related causes at 14%, and surgery-related causes at 10.2%.