Previous Issues Volume 1, Issue 1 - 2016
An Atypical Endoscopic Presentation of Sessile Serrated Adenoma
Nicholas M McDonald1,Guru Trikudanathan1,Khalid Amin2,Stuart K Amateau1
Corresponding Author: Stuart K Amateau, Assistant Professor, Director of Endoscopy, Division of Gastroenterology, VFW Cancer Research Center, 406 Harvard Street SE V371 MMC 36 Minneapolis, MN 55455, USA, Tel: (844) 273-8383; Email:[email protected]
Received Date: 02 Aug 2016 Accepted Date: 14 Sep 2016 Published Date: 19 Sep 2016
Copyright © 2016 Amateau S
Citation: McDonald NM, Trikudanathan G, Amin K, and Amateau SK. (2016). An Atypical Endoscopic Presentation of Sessile Serrated Adenoma. M J Gast. 1(1): 005.
ABSTRACT
Sessile serrated adenomas (SSA) were originally thought to be rare lesions, but recent literature suggests they may account for 3% to 9% of all colorectal polyps. Morphologically, these lesions are typically flat and Paris classification 0-IIa. The classic location of SSA is within the right colon. Here, we present a SSA which was pedunculated, Paris classification 0-Ip, and obtained from the sigmoid colon. To our knowledge, this represents a rare presentation of SSA with a limited number of previous cases. This observation should be considered by endoscopists when encountering similar lesions given the malignant potential of these polyps.
KEYWORDS
Sessile Serrated Adenoma; Polyp; Adenoma.
INTRODUCTION
Sessile serrated adenomas (SSA) are pre-malignant lesions that most commonly present in the right colon [1]. Recent literature has shown that SSA may account for up to 3% to 9% of all colorectal polyps [2]. Classically, SSA have a flat morphology and are often found along a mucosal fold. This flat morphology and location on mucosal folds can often present challenges in endoscopic detection [1]. SSA are most commonly class 0-IIa by Paris classification with a nonprotruding, nonexcavated, and slightly elevated (0 to 2.5 mm) appearance. Other typical l endoscopic findings of SSA include a thick “mucus cap” or “cloudlike”endoscopic findings of SSA include a surface and there is ongoing study regarding the utility of narrow-band imaging for improved detection; however further study is required [2-4]. Histologically, sessile serrated adenomas may be easily confused with other serrated lesions. In 2010 the World Health Organization categorized these serrated lesions into three groups: hyperplastic polyps, traditional serrated adenomas, and SSA. Sessile serrated adenomas are then further subdivided based upon presence or absence of dysplasia. Determining the specific lesion type, as well as presence or absence of dysplasia is important for both prognosis and determining the screening interval. SSAs are histologically differentiated through several features: degree of crypt dilatation, irregularity of crypt branching, and boot-shaped appearance of crypts [2]. In addition, SSA often contain higher concentrations of goblet cells. Presence of dysplasia is also used for differentiating prognosis and surveillance periods within SSA.
CASE REPORT
A 47-year-old woman with a history of endometriosis, gastric ulcer, Roux-en-Y gastric bypass surgery, and hysterectomy was referred to our group for evaluation of subacute abdominal pain. This pain was intermittent and without hematochezia. Computed tomography of the abdomen and pelvis showed mild circumferential thickening of the sigmoid colon without surrounding fat stranding. Colonoscopy was recommended to exclude an underlying mass lesion and diverticulitis, along with tandem esophagogastroduodenoscopy in the setting of pain. Esophagogastroduodenoscopy demonstrated Roux-en-Y gastric bypass anatomy and mild gastritis of the gastro-jejunal anastomosis. Colonoscopy revealed a 10mm pedunculated erythematous lesion (Figure 1) which was resected in toto via cold snare polypectomy. While endoscopic findings suggested tubulovillous adenoma, pathology revealed the polyp as a sessile serrated adenoma with no evidence of dysplasia, carcinoma, or endometriosis (Figure 2A and 2B). Interestingly, one month later at follow-up, her abdominal pain had fully resolved.

Figure 1: Endoscopic images: (A) Erythematous polypoid lesion within the mid-sigmoid; (B) Lifted cold snare resection; (C) Complete resection without defect or bleed.
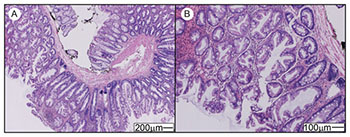
Figure 2: (A) Low resolution and (B) high resolution hematoxylin and eosin stain demonstrating typical characteristics of a sessile serrated adenoma including basal dilation of the crypts, crypt serration, horizontal crypts and crypt branching without evidence of high grade dysplasia or carcinoma.
DISCUSSION
In 2002 the Paris classification of superficial neoplastic lesions was released to aid in the morphologic classification of lesions in the esophagus, stomach, and colon [5]. Within the Paris classification for the large bowel, type 0 lesions are defined as superficial lesions which either do not invade the lamina propria or have invasion of the lamina propria, but a depth of penetration limited to the submucosa [5]. These lesions are further subdivided into polypoid and non-polypoid categorizations based upon whether or not the lesion protrudes above the surrounding surface on endoscopy. Polypoid lesions are given the classification of 0-I and non-polypoid lesions are classified as 0-II. The polypoid subcategory is further divided into sessile (0-Is) and pedunculated (0-Ip), based upon the diameter at the base of the polyp compared with the diameter at the top of the polyp [5]. In sessile polyps (0-Is) the base and the top of the lesion have the same diameter. In pedunculated polyps (0-Ip) the base has a narrower diameter than the top of the lesion. Sessile serrated adenomas are pre-malignant lesions which can be challenging to detect endoscopically. These lesions have several classical features which are commonly present: flat morphology, right-sided location“mucus cap”, and are under study regarding narrow-band imaging. In previous work by Tadepalli et al examining SSA morphology, these lesions were typically class 0-IIa (98.1% of SSAs were flat, with the vast majority of these lesions being class 0-IIa by Paris classification) [1]. The remaining 1.9% of lesions in their study were Paris classification 0-Is (protruding, sessile). Here, we reported a lesion which was superficial, polypoid, and pedunculated, and thus Paris classification 0-Ip. Furthermore, the classic location of SSA is within the right colon; here, we present a lesion which was obtained from the sigmoid colon. While our lesion did not vary in regards to narrow band imaging or vascular pattern, it was atypical both due to its location and its morphology by Paris classification. To our knowledge, this demonstration has rarely been observed for this entity and it should be considered by endoscopists when encountering a similar lesion given the pre-malignant potential.
REFERENCES
- Tadepalli US, Feihei D and Miller KM. (2011). “A morphologic analysis of sessile serrated polyps observed during routine colonoscopy (with video)."Gastrointestinal Endoscopy. 74(6), 1360-1368.
- Saito S. (2015).“Serrated Polyps of the Colon and Rectum: Endoscopic Features including Image Enhanced Endoscopy.”WJGE World Journal of Gastrointestinal Endoscopy. 7(9), 860- 871.
- Bettington ML and Chetty R. (2015). “Traditional Serrated Adenoma: An Update.” Human Pathology. 46(7), 933-938.
- Yamashina T and Takeuchi Y. (2015). “Diagnostic features of sessile serrated adenoma/polyps on magnifying narrow band imaging: A prospective study of diagnostic accuracy.” J Gastroenterology and Hepatology. 30(1), 117-123.
- Participants in the Paris Workshop.“The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon"November 30 to December 1, 2002.