Previous Issues Volume 1, Issue 1 - 2016
Adoption of Multi-class Fixed Dose Combination Once-daily Single Tablet HIV Regimen in Europe
Siva Narayanan1
1SVP and Global Head, Global Evidence, Value and Access, Ipsos Healthcare, Washington, USA.
Corresponding Author: Narayanan S, SVP and Global Head, Global Evidence, Value and Access, Ipsos Healthcare, 2020 K Street NW, Suite 410, Washington, DC, 20006, USA. Tel: +1 203-297-1208; E-Mail: [email protected]
Received Date: 03 May 2016 Accepted Date: 27 May 2016 Published Date: 03 Jun 2016
Copyright © 2016 Narayanan S
Citation: Narayanan S. (2016). Adoption of Multi-class Fi xed Dose Combination Once-daily Single Tablet HIV Regimen in Europe.Mathews J HIV AIDS. 1(1): 005.
ABSTRACT
Background and Aims
Once-daily multi-class fixed dose combination (FDC) once-daily single tablet regimen (STR) is critical part of antiretroviral treatment armamentarium to manage patients with human immunodeficiency virus (HIV). Multi-wave retrospective medical chart reviews of HIV patients were conducted in Europe (5EU: UK/France/Germany/Italy/Spain) between 1Q2009 and 1Q2015 among patients initiating or switching HIV regimen. Over 1Q2009-1Q2015, 200 physicians abstracted an average of 3000 patient charts per quarter. STR prescribing trends increased in 5EU over the years: 1Q2009- 17%, 1Q2010/1Q2011-23%, 1Q2012-24%, 1Q2013-30%, 1Q2014-44%, 1Q2015-53%. The top reasons for switching from conventional antiretroviral regimen dosing to an STR in 1Q2009/1Q2015 were simplification (74%/64%), tolerability (14%/19%), and patient decision (12%/18%). These observed trends may emphasize the importance HIV providers have given towards maintaining HIV patients on a simple and yet tolerable regimen with the hope to achieve optimal adherence and clinical outcomes over the longer term.
KEYWORDS
HIV; Single Tablet Regimen; STR, Fixed Dose Combination; FDC, Europe.
INTRODUCTION
Human Immunodeficiency Virus (HIV) continues to be a major global public health issue, having claimed more than 34 million lives so far. In 2014, approximately 1.2 million people died from HIV-related causes globally [1]. There is no cure for HIV infection. However, effective antiretroviral (ARV) drugs can serve as effective treatment to control disease progression among those with HIV, as well as to help prevent transmission so that people with HIV, and those at substantial risk, can have healthy and productive lives [1]. The World Health Organization (WHO) has advised countries to consider in-country combination ARV therapy costs and has encouraged implementation of public health approaches to scaling up quality HIV care and treatment and simplifying and standardizing ARV regimens [2, 3]. Single tablet regimens (STR) incorporate fixed dose combinations (FDC) of multi-class drugs into a single dosing unit that is administered once daily. Studies have suggested that HIV patients treated with once-daily fixed dose STRs are more adherent compared to patients on = 2 pills per day regimens, higher perceived quality of life (QoL) and lower costs to healthcare system, while STRs may also provide long-term durability, allowing for continued immunological recovery and increased life expectancy [4-12]. A number of STRs are already being marketed globally and a few new ones are under development [13, 14]. As new STRs become available, examining how STR prescribing trends have evolved in key markets and what has motivated physicians to switch HIV patients from conventional ARV regimen dosing to STRs could inform future evidence generation and messaging needs and corresponding positioning of STRs to benefit patients and other healthcare stakeholders.
MATERIALS AND METHOD
The study was a multi-country, multi-wave, multi-center retrospective medical chart review of adult (= 18 years) HIV patients conducted in the 5EU. Data was collected every quarter (Q) of the year since 2005. Physicians were sampled in each of the countries using online physician panels to attain a geographically representative sample in respective regions. Invitations to participate in research were sent to a random set of physicians in the existing online physician panels. The physicians representing both hospital-based and private practices in each geography, personally responsible for choosing and prescribing ARV treatment for patients with HIV, and treating a minimum of 15 HIV patients per month and having 3-35 years of clinical practice experience were screened for study participation. Each physician reported de-identified anonymous data on patients who recently initiated or switched ARVs as part of usual care within the defined study observation windows (for each wave/Q). An electronic data collection form was used to collect the following data elements from eligible HIV patient charts: patient demographics, comorbidities laboratory values (e.g., Viral Load and CD4+ cell count), HIV treatment patterns/dynamics and reasons for therapy initiation/change. Only de-identified anonymous data was collected from the patient charts by the treating physicians. This mode of data collection method met the criteria for local ethics review exemption per the respective physician/site requirements in the EU5. Study data analysis focused on STR prescribing trends between 1Q2009 and 1Q2015. A specific assessment of 1Q2009 and 1Q2015 was conducted to portray the changes in patient characteristics and the reason for ARV change (among the subset of patients having a HIV therapy change). Descriptive statistics were utilized to analyze the data.
RESULTS AND DISCUSSION
Approximately 200 physicians abstracted an average of 3000 eligible HIV patient charts in each of the study waves between 2009 and 2015. A total of 3132 and 3006 HIV patient charts were evaluated specifically in 1Q2009 and 1Q2015 respectively. Patient demographics were similar between the cohorts evaluated in 1Q2009 and 1Q2015, while the proportion of HIV patients with no comorbidities was lower in 1Q2015. The mean VL and CD4 count at initiation of ARV regimen were both higher among the 1Q2015 cohort (Table 1). None of the observed differences were statistically significant.
Table 1: Patient Demographic and Clinical Characteristics.
| 1Q2009 | 1Q2015 | |
|---|---|---|
| Age | n = 3125 | n = 2995 |
| Mean, years | 41 | 40 |
| Gender | n = 3132 | n = 3006 |
| Male, % | 69 | 71 |
| Female, % | 30 | 28 |
| Transgender, % | 1 | 1 |
| Ethnicity | n = 3028 | n = 2984 |
| Caucasian, % | 75 | 77 |
| African/Afro-Caribbean, % | 19 | 15 |
| Other, % | 6 | 8 |
| Route of Infection | n = 2977 | n = 2919 |
| Homosexual/bisexual, % | 41 | 47 |
| Heterosexual contact, % | 42 | 41 |
| IV drug user, % | 13 | 10 |
| Vertical transmission, % | 1 | 1 |
| Other/undetermined, % | 3 | 1 |
| Key Comorbidities | n = 3132 | n = 3006 |
| Chronic Hepatitis B, % | 7 | 4 |
| Depression/anxiety, % | 18 | 15 |
| Fat accumulation, % | 4 | 2 |
| Hepatitis C, % | 16 | 10 |
| Hyperlipidemia, % | 12 | 6 |
| Lipoatrophy, % | 8 | 3 |
| No concomitant condition, % | 39 | 49 |
| Viral Load at Initiation | n = 2262 | n = 2836 |
| Mean Count, copies/mL | 169,231,000 | 174,811,000 |
| CD4 Count at Initiation | n = 2704 | N = 2691 |
| Mean Count, cells/µL 2 | 262.4 | 327.9 |
Atripla, Eviplera, Stribild and Triumeq were the four STRs prescribed among the study cohorts. Proportion of HIV patients prescribed an STR increased in 5EU from 17% in 1Q2009 (UK: 29%, France: 1%, Germany: 12%, Italy: 16%, Spain: 29%) to 53% in 1Q2015 (UK: 50%, France: 47%, Germany: 77%, Italy: 41%, Spain: 51%) (Figures 1, 2). In 1Q2015, Out of the 53% on STRs, 11% were on Atripla, 23% on Eviplera, 15% on Stribild and 5% on Triumeq.
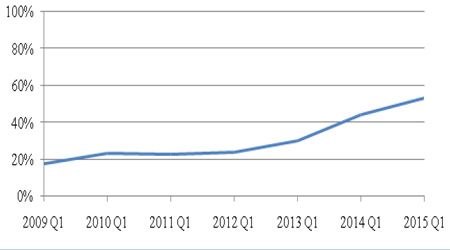
Figure 1: Percentage of Patients Initiated on STRs in 5EU.
Note5EU refers to the big-5 European countries, namely, the UK, France, Germany, Italy and Spain.
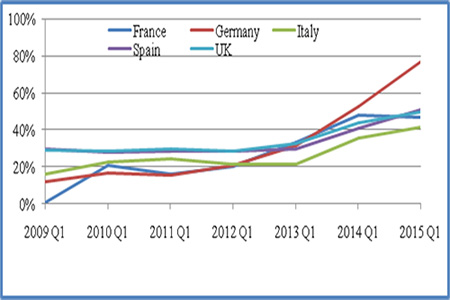
Figure 2: Percentage of Patients Initiated on STRs in the Individual European Countries.
Among the subset of patients who switched ARV drugs, 74%, 14% and 12% respectively switched from the conventional ARV combination drugs to an STR in 1Q2009 (across 5EU) due to simplification, tolerability and patient decision; 64%, 19% and 18% respectively switched to an STR in 1Q2015 (across 5EU) due to simplification, tolerability and patient decision (Figure 3).
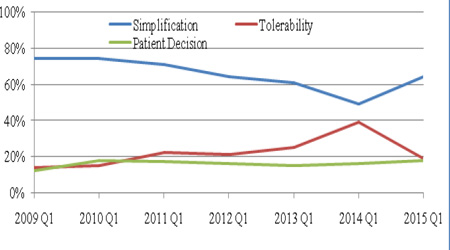
Figure 3: Reasons for STR Initiation: Percentage of Patients Initiated on STRs due to Simplification, Tolerability or Patient Decision.
The primary aim of ARV regimen is the prevention of the mortality and morbidity associated with chronic HIV infection at low cost of drug toxicity, with an additional aim of reducing the risk of sexual transmission of HIV [15]. STRs have been demonstrated to improve adherence, which is critical to not only better health but also to improved QoL, HIV prevention, HIV viral load suppression, drug resistance prevention, and ultimately survival [2, 5, 7, 9, 11, 16-21]. A recent literature review and meta-analysis comparing STRs to multi-tablet regimen confirmed the benefits of STRs associated with clinical, economic and humanistic outcomes [4]. Various international and national guidelines (in Europe) have hence recommended the use of STRs to treat HIV-infected individuals [15, 17, 22-25]. These factors may have influenced the positive trends in adoption of STRs in the 5EU observed in this research. The exponential increase in STR use in Germany and France, in comparison to the UK, Italy and Spain may be a function of differences in healthcare delivery dynamics within these countries. Evaluation of the reasons for initiation of STRs indicated a consistent pattern of emphasis on regimen‘simplification’. ‘Patient decision’ favoring STR initiation saw the most increase during the study period, complementing a slight decrease in the proportion reporting ‘regimen simplification’, indicating a gradual increase in patient involvement in treatment decisions. Proportion indicating ‘tolerability’ as the reason for STR initiation increased over the same time period slightly, aligned with the STR product profiles reported in the literature [4, 13] The real-world outcomes (such as changes in viral load and CD4 counts over time, and treatment adherence) were not assessed in this study. Such outcomes associated with the use of individual STRs observed in this study cohort could shed more light into the effectiveness of this utilization patterns, while such evolving evidence (if they were positive) might in-turn have fueled the progression of the observed practice patterns. Further research on this topic is warranted to discriminate therapeutic choices for optimal patient outcomes and foster best practices. Although physicians were randomly recruited for this study in respective geographies, the findings represent only the participating physician practices, and may vary from those of non-participating physician practices.
CONCLUSION
The adoption of STRs increased over the study period of 1Q2009 to 1Q2015, indicating a definite shift towards simple regimen that is more tolerable. There was a change in impetus to switch to STRs from simplification goal to an increasing focus on patient decision and tolerability. These observed trends may emphasize the importance HIV providers increasingly give towards maintaining HIV patients on a simple and yet tolerable regimen to achieve optimal adherence and clinical outcomes over the longer term. Evaluation of real-world comparative-effectiveness of these STRs is warranted to foster best practices.
CONFLICTS OF INTERESTS The author declares that there is no conflict of interest.
Acknowledgments
The author would like to acknowledge the contributions from Samantha Fernando and Sarah Brown for their efforts with coordinating data collection and analysis. A part of the results depicted in this research article was presented in the form of an abstract at 31st International Conference on Pharmacoepidemiology & Therapeutic Risk Management, August 2015, Boston, USA.
REFERENCES
- World Health Organization. HIV/AIDS Factsheet Number 360. 2014.
- World Health Organization. (2010). Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach – 2010 revision.
- World Health Organization. (2010). Antiretroviral treatment working group treatment white paper. 2010a.
- Clay P, Nag S, Graham C, Narayanan S, et al. (2015). Meta- Analysis of Studies Comparing Single and Multi-Tablet Fixed Dose Combination HIV Treatment Regimens. Medicine (Baltimore). 94(42), e1677.
- Astuti N and Maggiolo F. (2014). Single-Tablet Regimens in HIV Therapy. Infect Dis Ther. 3(1), 1-17.
- Aldir, I, Horta A and Serrado M. (2014). Single-tablet regimens in HIV: Does it really make a difference? Current Medical Research and Opinion. 30(1), 89-97.
- Cohen CJ, Meyers JL and Davis KL. (2013). Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US medicaid population with HIV. BMJ Open. 3(8), e003028.
- Buscher A, Hartman C, Kallen MA and Giordano TP. (2012). Impact of Antiretroviral Dosing Frequency and Pill Burden on Adherence among Newly Diagnosed, HAART Naïve, HIV Patients. Int J STD AIDS. 23(5), 351-355.
- Cohen C, Elion R, Ruane P, Shamblaw D, et al. (2011). Randomized, phase 2 evaluation of two single-tablet regimens elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate versus efavirenz/emtricitabine/ tenofovir disoproxil fumarate for the initial treatment of HIV infection. AIDS. 25(6), F7-12.
- Juday T, Gupta S, Grimm K, Wagner S, et al. (2011). Factors associated with complete adherence to HIV combination antiretroviral therapy. HIV Clinical Trials. 12(2), 71-78.
- Nachega JB, Mugavero MJ, Zeier M, Vitória M, et al. (2011). Treatment simplification in HIV-infected adults as a strategy to prevent toxicity, improve adherence, quality of life and decrease healthcare costs. Patient Prefer Adherence. 5, 357-367.
- Deeks ED and Perry CM. (2010). Efavirenz/emtricitabine/ tenofovir disoproxil fumarate single-tablet regimen (Atripla): A review of its use in the management of HIV infection. Drugs. 70(17), 2315-2338.
- Truong WR, Schafer JJ and Short WR. (2015). Once-Daily, Single-Tablet Regimens for the Treatment of HIV-1 Infection. P T. 40(1), 44-55.
- Graham B. (2015). Upcoming Novel HIV Single Tablet Regimens. December 1.
- British HIV Association (BHIVA) guidelines for the treatment of HIV-1 positive adults with antiretroviral therapy 2015, September 2015.
- Nachega JB, Parienti JJ, Uthman OA, Gross R, et al. (2014). Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: A meta-analysis of randomized controlled trials. Clin Infect Dis. 58(9), 1297-1307.
- Department of Health and Human Services (DHHS). Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents, 28 Jan 2016.
- Molassiotis A, Nahas-Lopez V, Chung WY, Lam SW, et al. (2002). Factors associated with adherence to antiretroviral medication in HIV-infected patients. Int J STD AIDS. 13(5), 301-310.
- Chesney MA. (2006). The elusive gold standard. Future perspectives for HIV adherence assessment and intervention. J Acquir Immune Defic Syndr. 43(Suppl 1), S149-155.
- Cohen MS, Chen YQ, McCauley M, Gamble T, et al. (2011). Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 365(6), 493-505.
- Vitoria M, Ford N, Doherty M and Flexner C. (2014). Simplification of antiretroviral therapy: a necessary step in the public health response to HIV/AIDS in resource-limited settings. Antiviral Therapy. 19(Suppl 3), 31-37.
- European AIDS Clinical Society (EACS). (2016). Guidelines, version 8.0, October 2015.
- Hoen B, Bonnet F, Delaugerre C, Delobel P, et al. (2013). French HIV expert group. French 2013 guidelines for antiretroviral therapy of HIV-1 infection in adults. J Int AIDS Soc. 17, 19034.
- GeSIDA/National AIDS Plan: Consensus document on antiretroviral therapy in adults infected by the human immunodeficiency virus (Updated January 2015). (2015). Enferm Infecc Microbiol Clin. 33(8), 543.e1-43.
- Antinori A, Marcotullio S, Andreoni M, Ammassari A, et al. (2015). Italian HIV Guidelines Working Group. Italian guidelines for the use of antiretroviral agents and the diagnostic- clinical management of HIV-1 infected persons. Update December 2014. New Microbiol. 38(3), 299-328.