Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2025
A Rare Posterior Fossa Complication of Spinal Surgery: Case Report
Hajer Kammoun*, Mohamed Dehmani Yedeas, Ridha Chkili, Khaled Radhouen, Sameh Achoura
Department of Neurosurgery, Military Hospital of Tunis, Tunisia
*Corresponding Author: Hajer Kammoun, Department of Neurosurgery, Military Hospital of Tunis, Tunisia, Phone: 99969757, E-mail: [email protected]
Received Date: April 06, 2025
Published Date: June 02, 2025
Citation: Kammoun H, et al. (2025). A Rare Posterior Fossa Complication of Spinal Surgery: Case Report. Mathews J Surg. 8(1):38.
Copyrights: Kammoun H, et al. © (2025).
ABSTRACT
Background: Remote Cerebellar hemorrhage after spinal surgery is rare, but potentially lethal due to the location of the bleeding. The first reported case was in 1981 by Chadduck. Since then, it was described mostly in cases of intraoperative dural tearings with cerebrospinal fluid (CSF) leakage, even those repaired intraoperatively. Case presentation: A 48-year-old patient was admitted to our department for bilateral lumbosciatalgia not responding to analgesics, intermittent radicular claudication and vesicosphincteric disorders. The MRI revealed a lumbar stenosis. He underwent from L3 to L5 laminectomy with fusion, complicated by a dural tear repaired intraoperatively. Nevertheless, the patient presented a CSF leak at the surgical scar and acetazolamide was prescribed. Persistent headache and the onset of a cerebellar syndrome motivated the performance of a brain computed tomography showing a left cerebellar hematoma. Hyperhydration and blood pressure monitoring were maintained and the patient was discharged two weeks after surgery. Conclusion: It is important to consider the possibility of remote cerebellar hemorrhage in patients who exhibit unexplained neurological deterioration after spinal surgery, especially when a large volume of CSF has been lost intraoperatively or postoperatively. Early detection and correct interpretation of the typical bleeding pattern can help avoiding further aggravation of symptoms.
Keywords: Cerebellar Hematoma, Spine Surgery, Dural Tearing, Risk Factors.
INTRODUCTION
Postoperative remote intracranial hemorrhage can occur in supratentorial, cerebellar, epidural, or subdural compartments [1]. Remote Cerebellar hemorrhage (RCH) after spinal surgery is rare, but potentially lethal due to the location of the bleeding [2].
The first reported RCH case was by Chadduck in 1981, occurring after a cervical laminectomy [3]. RCH after spinal surgery was described mostly in cases of intraoperative dural tearings with cerebrospinal fluid (CSF) leakage. In those repaired intraoperatively, this complication was also reported in literature but much rarer [4], leading to diagnosis and treatment delay. Through this case-report, we are pointing out this possible mortal complication of lumbar surgery and reviewing its risk factors aiming to better the handling of such patients.
ILLUSTRATIVE CASE
We report the case of a 48-year-old male patient, with tobacco consumption (20 pack-years), and no medical history, who was admitted to our department for non-systematized bilateral lumbosciatalgia, with no response to analgesics. He presented also intermittent radicular claudication and vesicosphincteric disorders (pollakiuria).
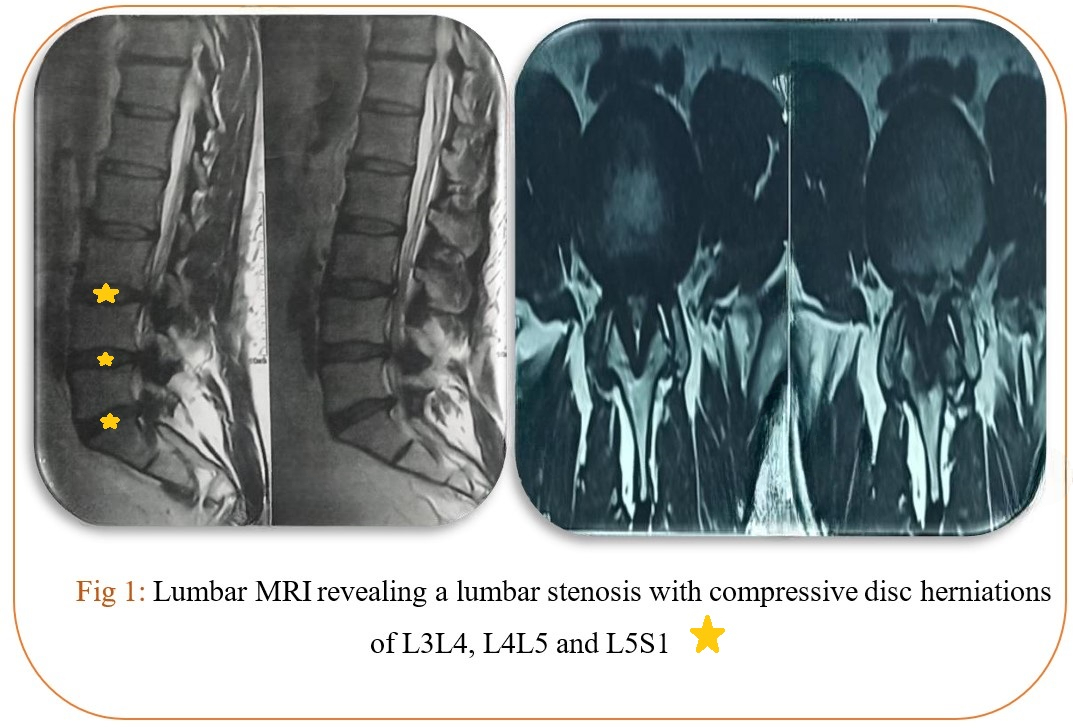
The Lumbar magnetic resonance imaging (MRI) revealed a lumbar stenosis and compressive disc herniations of L3-L4, L4-L5 and L5-S1 (Fig. 1).
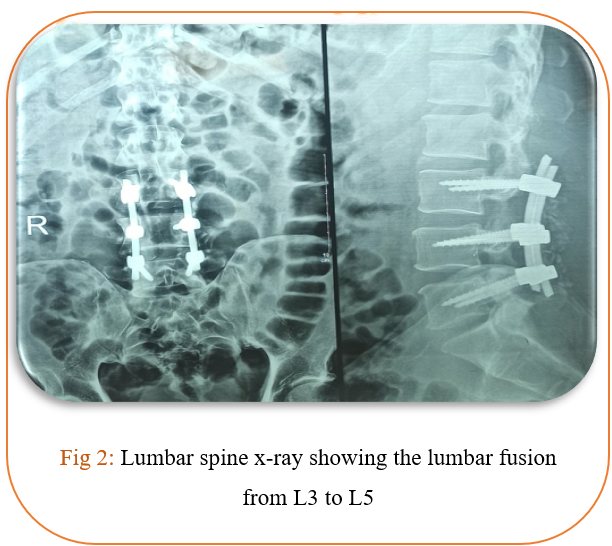
After he gave an informed consent, the patient underwent laminectomy from L3 to L5 with fusion (Fig.2).
The laminectomy was complicated per operatively by a posterior median dural tear which was sutured and on which fat was placed with a subaponeurotic drain (siphoning).
The patient sought care for lower back pain and paresthesia of the left leg immediately after the operation. The surgical drain brought back an important amount of clear colorless watery fluid (around 700 ml) made of blood and CSF.
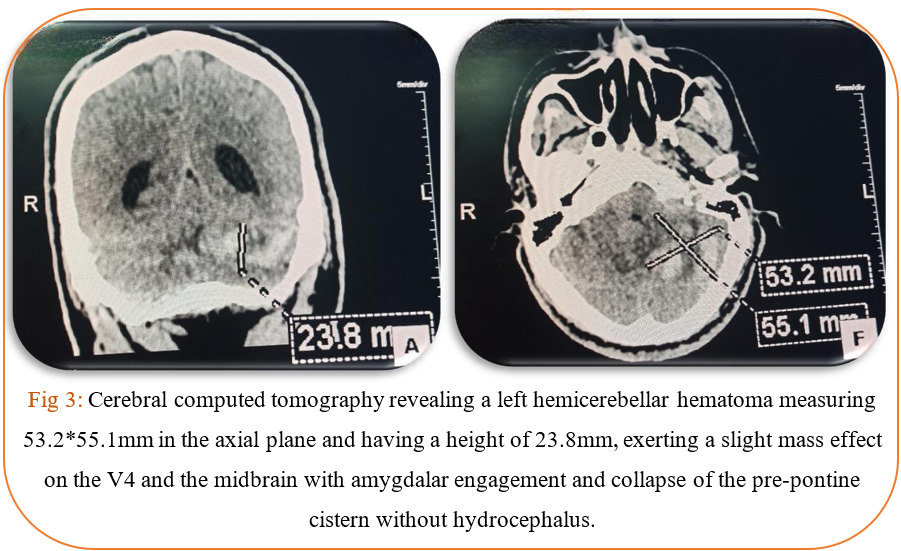
After removal of the drain (48 hours after the operation), we noticed that the patient presented a CSF leak from the surgical scar and acetazolamide was prescribed. He presented then a headache. An intracranial hypotension syndrome was suspected and the patient received hyperhydration. In front of a persistent headache and the onset of kinetic and static left cerebellar syndrome, brain computed tomography (CT) was performed, showing a left cerebellar hematoma (Fig.3).
Hyperhydration and blood pressure monitoring were maintained. On day 12 after the surgical procedure, the cerebellar syndrome, headache and dizziness regressed and the radiological control showed regression of the hematoma. The patient was discharged two weeks after surgery.
DISCUSSION
According to literature, there are several theories on the pathological mechanisms of RCH.
Most claims are related with the involvement of venous system [5-8]. They suggest that the cerebellar sag resulting from intraoperative or postoperative cerebrospinal fluid (CSF) drainage might stretch and occlude the bridging cerebellar veins leading to hemorrhagic venous infarction. This can be followed by reperfusion hemorrhage or venous bleeding secondary to increased venous pressure. This theory is still a matter of debate.
In fact, RCH involves area larger than the territory of a single vein and usually does not demonstrate edema or cerebellar swelling, which is not concordant with the cerebellar sag theory [9].
The latter explains our case though and can be supported by the fact that hemorrhage was located in the upper vermis and cerebellar sulci, where the cerebellar draining veins are located, drawing with the layering of streaky pattern of hyperdense blood, intermixed with cerebellar parenchyma, the classic “zebra sign” [10].
The leakage of a large amount of CSF in a short period of time, like in our case, may also be required for cerebellar hemorrhage to occur because RCH is, although possible, extremely rare after lumbar puncture [11].
Nevertheless, some cases of RCH following uncomplicated lumbar spinal decompression and fusion were reported [12].
Studying the risk factors, looking for predictive elements of this complication, no correlations between RCH and age, sex, pathology operated, or type of interventions performed were retained [13,14].
The possible factors mentioned were preexisting coagulopathy, hypertension and obstruction of jugular vein by extreme head rotation. In fact, patient positioning is another factor that is widely suspected to contribute to RCH [15], but the relevance of this in spinal surgery is still unclear.
CONCLUSION
It is important to consider the possibility of RCH in patients who exhibit unexplained neurological deterioration after spinal surgery, especially when a large volume of CSF has been lost intraoperatively or postoperatively, even if the dural tear was repaired. Such patients should undergo immediate neurological imaging. Early detection and correct interpretation of the typical bleeding pattern can help avoiding further aggravation of symptoms.
DISCLOSURES
No sources of support/funding.
No conflict of interest for any of the authors related to the manuscript or its subject matter.
ACKNOWLEDGMENTS
Not applicable.
REFERENCES
- Liu F, Li D, Yang T, Li C, Luo X, Li M, et al. (2022). Remote cerebellar hemorrhage after supratentorial craniotomy: illustrative cases. J Neurosurg Case Lessons. 3(14):CASE21687.
- Nam TK, Park SW, Min BK, Hwang SN. (2009). Remote cerebellar hemorrhage after lumbar spinal surgery. J Korean Neurosurg Soc. 46(5):501-504.
- Chadduck WM. (1981). Cerebellar hemorrhage complicating cervical laminectomy. Neurosurgery. 9(2):185-189.
- Sturiale CL, Rossetto M, Ermani M, Baro V, Volpin F, Milanese L, et al. (2016). Remote cerebellar hemorrhage after spinal procedures (part 2): a systematic review. Neurosurg Rev. 39(3):369-376.
- Friedman JA, Ecker RD, Piepgras DG, Duke DA. (2002). Cerebellar hemorrhage after spinal surgery: report of two cases and literature review. Neurosurgery. 50(6):1363-1364.
- Honegger J, Zentner J, Spreer J, Carmona H, Schulze-Bonhage A. (2002). Cerebellar hemorrhage arising postoperatively as a complication of supratentorial surgery: a retrospective study. J Neurosurg. 96(2):248-254.
- Toczek MT, Morrell MJ, Silverberg GA, Lowe GM. (1996). Cerebellar hemorrhage complicating temporal lobectomy. Report of four cases. J Neurosurg. 85(4):718-722.
- Yoshida S, Yonekawa Y, Yamashita K, Ihara I, Morooka Y. (1990). Cerebellar hemorrhage after supratentorial craniotomy--report of three cases. Neurol Med Chir (Tokyo). 30(10):738-743.
- Calisaneller T, Yilmaz C, Ozger O, Caner H, Altinors N. (2007). Remote cerebellar haemorrhage after spinal surgery. Can J Neurol Sci. 34(4):483-484.
- Brockmann MA, Nowak G, Reusche E, Russlies M, Petersen D. (2005). Zebra sign: cerebellar bleeding pattern characteristic of cerebrospinal fluid loss. Case report. J Neurosurg. 102(6):1159-1162.
- Bernal-García LM, Cabezudo-Artero JM, Ortega-Martínez M, Fernández-Portales I, Ugarriza-Echebarrieta LF, Pineda-Palomo M, et al. (2008). Hematomas de cerebelo como complicación de drenaje lumbar. Presentación de dos casos y revisión de la literatura [Remote cerebellar hemorrhage after lumbar spinal fluid drainage. Report of two cases and literature review]. Neurocirugia (Astur). 19(5):440-445.
- Hofler RC, Wemhoff MP, Johans SJ, Nockels RP. (2019). Cerebellar Hemorrhage Following an Uncomplicated Lumbar Spine Surgery: Case Report. J Stroke Cerebrovasc Dis. 28(7):e104-e105.
- Hempelmann RG, Mater E. (2012). Remote intracranial parenchymal haematomas as complications of spinal surgery: presentation of three cases with minor or untypical symptoms. Eur Spine J. 21(Suppl 4):S564-S568.
- Konya D, Ozgen S, Pamir MN. (2006). Cerebellar hemorrhage after spinal surgery: case report and review of the literature. Eur Spine J. 15(1):95-99.
- König A, Laas R, Herrmann HD. (1987). Cerebellar haemorrhage as a complication after supratentorial craniotomy. Acta Neurochir (Wien). 88(3-4):104-108.