Previous Issues Volume 3, Issue 2 - 2018
Mesenchymal Stem Cells
Michel Goldberg*
Professor Emeritus, Faculty of Fundamental and Biomedical Sciences of the Saints Peres. Rene Descartes University, Paris Cite & INSERM UMR-S 1124. 45 rue des Saints Fathers Paris.
Corresponding Author: Michel Goldberg, Professor Emeritus, Faculty of Fundamental and Biomedical Sciences of the Saints Peres. Rene Descartes University, Paris Cite & INSERM UMR-S 1124. 45 rue des Saints Fathers Paris, E-Mail: mgoldod@gmail
Received Date: 09 Nov 2018 Accepted Date: 13 Nov 2018 Published Date: 14 Nov 2018 Copyright © 2018 Goldberg M
Citation: Goldberg M. (2018). Mesenchymal Stem Cells. Mathews J Dentistry. 3(2): 024.
ABSTRACT
Adult stem cells allow to distinguish between mesenchymal stem cells (MSCs) and marrow-derived mesenchymal stem cells (MDMSCs). Embryonic stem cells have enormous potential in the field of tissue engineering and regenerative medicine as they hold the capacity to produce every type of cell and tissue in the body. Stemness is probed through in vivo transplantation experiments. Multipotency may be explored at the single cell level, and self-renewal means reconstitution of a stem cell population identical in phenotype and function to the one originally explanted. Mesenchymal stem cells (MSCs) may differentiate into cells of the osteogenic, chondrogenic, tendonogenic, adipogenic, and myogenic lineages. They express CD105, CD73 and CD90 surface molecules markers, but have depleted expression of CD45, CD34, CD14 or CD11b, CD79a or CD19 and HLA-DR surface molecules. Consequently, they may be used in tissue repair and regeneration.
KEYWORDS
Mesenchymal Stem Cells; Marrow-Derived Mesenchymal Stem Cells; Expression of Surface Molecules; Osteoblasts; Adipocytes; Chondroblasts; Cell Lineages.
INTRODUCTION
Adult stem cells allow to distinguishing between mesenchymal stem cells and marrow-derived mesenchymal stem cells Stem cells are defined as having the capacity for extensive self-renewal and for giving rise to one type of highly differentiated progeny.
Embryonic stem cells (ESCs) have huge potential in the field of tissue engineering and regenerative medicine. They hold the capacity to produce every type of cell and tissue in the body. The treatment of human disease could be transformed by the ability to generate any cell, tissue, or even organ, on 'demand' in the laboratory. Bone and cartilage formation in the embryo, as well as repair and turnover in the adult, involve the progeny of a small number of cells called mesenchymal stem cells. These cells divide, and their progeny become committed to a specific phenotypic pathway, and end-stage cells involved in the fabrication of a unique tissue type, e.g., cartilage or bone.
Adult stem cells are implicated in the development of multicellular organisms. This is accomplished through a series of events that are preprogrammed in the genome. These events encompass cellular proliferation, lineage commitment. There are two categories of precursor stem cells: those which are multipotent, tripotent, bipotent, and unipotent progenitor cells and lineage-uncommitted pluripotent (epiblastic-like, ectodermal, mesodermal, and endodermal). Many studies have led to the discovery that two general categories of precursor cells exist within the body. They are involved in the maintenance and repair of tissues in adults either as lineage-committed progenitor cells, or as lineage-uncommitted pluripotent stem cells (Young & Black, 2004).
Mesenchymal stem cells (MSCs) constitute a population of pluripotent cells within the bone marrow microenvironment, defined by their ability to differentiate into cells of the osteogenic, chondrogenic lineages (Majumdar et al., 1998).
Bone marrow stromal cells (BMSCs) are progenitors of skeletal tissue components such as bone, cartilage. In addition, they may be experimentally induced to undergo unorthodox differentiation, possibly forming neural and myogenic cells.
These cells may be found within the tissue or in other tissues that serve as stem cell reservoirs. The adult bone marrow also contains mesenchymal stem cells (MSCs), which contribute to the regeneration of mesenchymal tissues (Pittenger et al. 1999).
Human mesenchymal stem cells (MSCs) are multipotent cells present in adult marrow. They may replicate as undifferentiated cells. They have the potential to differentiate into lineages of mesenchymal tissues. The adult bone marrow contains mesenchymal stem cells (MSCs) contributing to the regeneration of mesenchymal tissues (Caplan 1991).
Conceptually, an "MSC" is capable of generating a complete heterotopic bone / bone marrow organ in vivo, including a compartment of perivascular stromal cells with similar phenotype and properties as the originally explanted cell (Bianco et al., 2013).
Adult marrow-derived mesenchymal stem cells (MDMSCs) may divide and their progeny differentiate into one of several mesenchymal phenotypes.
They are called "multipotent stromal cell" keeping the same ac-ronym "MSC" as mesenchymal stem cells. Several studies have demonstrated that MSCs can be isolated from multiple tissues.
Medicinal Signaling Cell constitutes another adequate terminology (Caplan 2017). Bone marrow stem cells do not contribute to the formation of blood cells and they do not express the hematopoietic stem cell marker CD34. Non-marrow tissues such as placenta and the dental pulp of deciduous teeth are characterized by a small cell body, with a few cell processes that are long and thin.
Physico-chemical properties of bone marrow (mesenchymal) stem cells Stem cell plasticity refers to the ability of adult stem cells to acquire mature phenotypes that are different from their tissue of origin. Adult bone marrow cells (BMCs) include two populations of bone marrow stem cells (BMCs):
- hematopoietic stem cells (HSCs), giving rise to all lineages of blood, and
- mesenchymal stem cells (MSCs). These later may differentiate into bone, cartilage, and fat (Grove et al., 2004).
Mesenchymal stem cells (MSCs) adhere to plastic in vitro and expand in tissue culture with a finite lifespan of 15-50 cell doublings. Under appropriate stimuli, MSCs differentiate in vitro and in vitro.
Every cell in the body has a lifespan ranging from 20 minutes to many years, depending on the cell. Some circulating blood cells expire in 20 minutes after forming, while neurons exist for many years.
Reverse transcriptase-polymerase chain reaction (RT-PCR) was used to amplify the transcripts expressed by multiple genes whose expression is restricted to the adipocytic (PPARg2 and aP2), chondrocytic (type II and IX collagens), or osteocytic (osteopontin and alkaline phosphatase) lineages.
Mesenchymal stem cells (MSCs) have been isolated from bone marrow, periosteum, trabecular bone, adipose tissue, skeletal muscle and deciduous teeth. These cells have the capacity to differentiate into cells of connective tissue, including bone, fat, cartilage and muscle.
Mesenchymal stem cells (MSCs), which reside within the stromal compartment of bone marrow were identified in the pioneering studies of Friedenstein and Petrakova (1966), who isolated bone-forming progenitor cells from rat marrow. They differentiate into cells of connective tissue lineages. MSCs represent a very small fraction, 0.001-0.01% of the total population of nucleated cells in marrow (Pittenger et al., 1999 ) These attached mesenchymal cells were expanded and uniformly positive for SH2, SH3, CD29, CD44, CD71, CD90, CD106, CD120a, CD124, and other surface proteins (Caplan, 2005, 2007. 2008 ; Kundrotas 2012).
Adipogenic differentiation was induced in the mesenchymal cell cultures by treatment with 1-methyl-3-isobutylxanthine, dexamethasone, insulin, and indomethacin.
To promote chondrogenic differentiation, the isolated mesenchymal cells were centrifuged to form a pelleted micromass and cultured without serum and with transforming growth factor- β3.
The osteogenic differentiation of cultured human mesenchymal cells derived from adult bone marrow has been characterized. The isolated mesenchymal cells formed aggregates or nodules and increased their expression of alkaline phosphatase. RT-PCR was used to amplify the transcripts expressed from multiple genes whose expression is restricted to the adipocytic (PPAR ? 2 and aP2), chondrocytic (type II and IX collagens), or osteocytic (osteopontin and alkaline phosphatase) lineage.
Wnt/β-catenin signaling has been implicated in cell-fate determination and stem cell expansion, To directly test whether Wnt signaling is critical to self-renewing proliferation of hESCs, two soluble Wnt antagonists were used : the secreted Frizzled-Related Protein 2 (sFRP2) and Dickoppf-1 (Dkk-1), which block the binding of Wnt to its receptors Frizzled and the coreceptors Low-Density Lipoprotein Receptor Related Protein (LRP)-5 or LRP-6, respectively. Both antagonists were used previously to block diverse functions of the Wnt signaling in vivo or in vitro (Dravid et al., 2010 ; Rodriguez-Lozano 2012).
Is the term of mesenchymal stem cell appropriate Questions have been raised related to the usage of the term "mesenchymal stem cells" (Barry & Murphy 2004). First, the original naming as mesenchymal was based on the hypothesis that multiple tissues beyond skeletal lineages could be generated by postnatal MSCs (Caplan, 2005 , 2007, 2008).
Second, during prenatal organogenesis, the series of tissues was generated by a system of progenitors, rather than from a common ancestor. In fact, bone as a tissue develops from neuro ectodermal progenitors (craniofacial bones) or from axial and lateral specifications of the mesoderm. In addition, postnatal progenitors (and MSCs) have a distinct origin.
- Stemness is probed through in vivo transplantation experiments,
- Multipotency can only be probed at the single cell level,
- Self-renewal means reconstitution of a stem cell population identical in phenotype and function to the one originally explanted.
The « skeletal stem cell « concept describes the difference between the two concepts and is presented in the following figure.
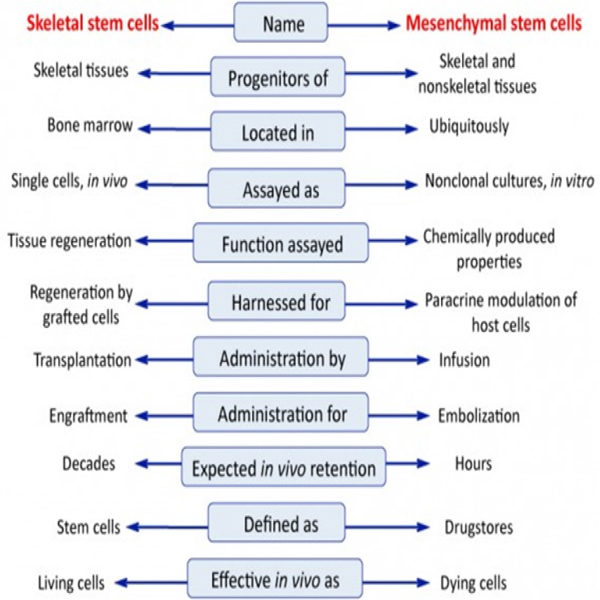
Adapted and modified from Bianco et al. 2013.
Are all the Perivascular Mesenchymal Cells pericytes ? A subpopulation of human perivascular cells express both pericyte and mesenchymal stem cell (MSC) markers in situ. The isolated population can expand and is clonally multipotent in culture, establishing that MSCs found throughout fetal and adult tissues are members of the pericyte family of cells.
Cells with MSC markers also express pericyte markers. The pericytes do not differentiate into hematopoietic phenotypes in adults. The vascular/perivascular location of hematopoietic and neural stem cells implies that other stem cells inhabit the perivascular niche. This documents that not all pericytes are MSCs.
The following question is related to the identity of MSCs pericytes. All pericytes are not MSCs, since both large and small vessels are surrounded by perivascular cells with highly differentiated functions quite separate from the activities associated to the osteo-, chondro-, or adipogenic progeny of MSCs. Adult bone marrow contains rare, yet powerful multipotent progenitor cells. These cells have two important capacities :
- First, MSCs can differentiate into distinct end-stage cell types,
- Second, MSCs secrete a broad spectrum of bioactive macromolecules that are both immunoregulatory and serve to structure regenerative microenvironments in the broad fields of tissue injury (Caplan, 2008).
Identification of MSCs by monoclonal antibodies Recent studies suggest that the use of CD10, CD26, CD106, CD146 and ITGA11 could be helpful for the discrimination of MSCs from fibroblasts.
First, MSCs must be plastic-adherent when maintained in the standard culture conditions.
Second, several monoclonal antibodies have been raised in an effort to provide reagents for the characterization and isolation of human MSCs. MSCs must express CD105, CD73 and CD90, and lack expression of CD45, CD34, CD14 or CD11b, CD79a or CD19 and HLA-DR surface molecules.
Third, MSCs must differentiate into osteoblasts, adipocytes and chondroblasts in vitro.
The results of recent studies suggest that the use of CD10, CD26, CD106, CD146 and ITGA11 could be helpful for the discrimination of human bone marrow MSCs from human dermal fibroblasts (Kundrotas 2012).
For instance,
1. Stro-1 was identified as an antibody that reacts with nonhaematopoietic progenitor bone marrow stromal cells.
2.The SB-10 antibody was shown to be reactive with an antigen present on undifferentiated MSCs, which disappeared once the cells embarked upon the osteogenic pathway and began to express cell surface alkaline phosphatase.
The specific SB-10 antigen was identified as CD166 (activated leukocytecell adhesion molecule, ALCAM) which may play a role in the progression of osteogenic differentiation.
3.The SH-2 antibody (also raised against human MSCs), reacts with an epitope present on the transforming growth factorbeta (TGF-β), and receptor endoglin (CD105).
This antibody has been used in immunomagnetic selection methods for human MSCs although CD105 is dominantly associated with endothelial cells.
4. Both the SH-3 and SH-4 antibodies apparently recognize distinct epitopes on the membrane-bound ecto-5' -nucleotidase (CD73).
The fundamental principle of stem cell therapy is that undifferentiated cells under the influence of local signals, will differentiate to cells of the appropriate phenotype. These differentiated cells contribute to the repair of the injured tissue. There is evidence to indicate that this is the case, but there are little or no data concerning the specific signals that give rise to differentiation in situ.
Repair and regeneration of damaged tissues MSCs are positioned for a broader spectrum of clinical applications. MSC regenerate damaged tissue and treat inflammation. Chondrocytes are positive for CD73, CD90 and CD105 but negative for CD11b, CD14, CD34, CD45, CD79a and HLA-DR surface markers. MSC secretes cytokines and growth factors that are antiapoptotic, proangiogenic and have the potential to reduce scarring and inflammation (Ankrum & Kartp, 2010).
Mesenchymal stem cells are multipotent cells found in several adult tissues. The concept emerged that there may be a mesenchymal stem cell (MSC) (Caplan, 2007). These vascularassociated mesenchymal cells are referred to as pericytes, smooth muscle cells, vascular support cells, etc. When isolated and assayed in culture, these cells have MSC-like characteristics (Caplan, 1991).
CHONDROCYTES
A discrete set of expressional stages or lineage states, comprising dividing, maturing, and hypertrophic chondrocytes, is apparent in embryonic limb tissue, cell culture, and in the growth plate. Eventually, the hypertrophic cartilage is eroded by vascular, marrow, and phagocytic cells and replaced by bone. For example, hypertrophic chondrocytes synthesize a unique small collagen, type X, and a unique proteoglycan. None of these molecules is synthesized by mature chondrocytes. Several factors contribute to conversion of mature chondrocytes to hypertrophic chondrocytes
First, embryonic mesenchymal stem cells in the limb which give rise to cartilage and bone in vivo can be influenced in vitro.
Second, these cells have a lineage progression of separate, individual steps, whether it is the chondrogenic or osteogenic pathway.
Third, protein factors are responsible for providing positional information and causing lineage progression. Cell culture conditions provide control of tissue size and function.
Fourth, although chondrocytes and osteoblasts are derived from a common mesenchymal cell, the conditions for their initial differentiation and progression through the individual steps of their lineages are different. For example, osteogenesis is dependent on proximity to vasculature whereas chondrogenesis requires the complete absence of vasculature.
Fifth, bone forms from mesenchymal stem cells in a cartilageindependent manner with vasculature providing a determinative discriminator between these two tissues. Embryonic cartilage is not replaced by bone, but rather by vasculature and marrow.
Sixth, we can demonstrate that three tissue sites are tightly linked to mesenchyma1 stem cells: marrow, periosteum, and muscle connective tissue.
Fibrocytes arise from CD14+ CD34+ CD45+ peripheral blood mononuclear cells and account for between 0.1% and 0.5% of circulating leukocytes. Following their expansion in vitro, fibrocytes express markers of haematopoietic stem cells (CD34, CD105), of leukocytes (CD45, LSP-1), monocytes (CD11a, CD11b, CD13, CD32, CD64), Fc? receptors (CD16, CD32a, CD32b, CD32c), cell surface molecules involved in antigen presentation (MHC Class I, II, CD40, CD54, CD80 and CD86) and integrins (CD18, CD29, CD49a, CD49b, CD49e, CD61). Fibrocytes also express several receptors and secrete a range of extracellular matrix (ECM) proteins (Collagens I, III, IV and V, fibronectin, vimentin, tenascin, a-smooth muscle actin (a-SMA), matrix metalloproteinase- 9 (MMP-9)) and glycosaminoglycans (perlecan, versican, hyaluronan, decorin and biglycan) (Browne et al., 2013).
MSCs are essential for tissue morphogenesis during development, haematopoiesis throughout life, and the orchestration of tissue repair following acute and chronic injuries. Their involvement in such diverse biological activities are in large part attributable to their ability to undergo trans-differentiation to and from epithelial cells.
In summary, MSC are thought to have at least five primary roles in vivo as progenitor cells for bone formation during bone remodelling or repair, cartilage formation, vascular support, haematopoietic support, and progenitors for adipocytes. Proliferation in the "aged"MSC cultures began to decline and growth curve reached a plateau. In contrast, cultures derived from "adult" donors continued to proliferate (Stolzing et al., 2008).
MSCs are called "multipotent stromal cell", keeping the same ac-ronym "MSC" as mesenchymal stem cells. Several studies have demonstrated that MSCs are implicated in the repair and regeneration of damaged tissues. Bone remodelling and repair, cartilage formation, progenitors for adipocytes, vascular and hematopoietic support can be manipulated. MSC are found in many tissues including bone marrow, and they play an essential role in tissue morphogenesis.
Many studies have led to the discovery that two general categories of reserve precursor cells exist within the body. They are involved in the maintenance and repair of tissues in adults either as lineage-committed progenitor cells, or as lineage-uncommitted pluripotent stem cells.
The adult bone marrow also contains mesenchymal stem cells (MSCs). MSC are able to secrete cytokines and growth factors that are antiapoptotic, proangiogenic and reduce scarring and inflammation. MSCs provide new tools contributing actively to tissue repair and regeneration. Deciphering the biology of innate MSCs may have important positive consequences for the therapeutic use of these cells (Murray & Peault 2015). A number of fundamental questions need to be resolved before mesenchymal progenitors can be used for clinical applications in the context of both cell and gene therapies (Minguell et al., 2001). The controlled activation of MSCs in their native environment constitutes an important future therapeutic approach.
REFERENCES
- Young HE and Black AC Jr. (2004). Adult stem cells. Anat Rec Part A. 276(1) : 75-102.
- Majumdar MK, Thiede MA, Mosca JD, Moorman M, et al. (1998). Phenotypic and functional compatison of cultures of marrow-derived mesenchymal stem cells (MSCs) and stromal cells. J Cell Physiol. 176(1): 57-66.
- Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, et al. (1999). Multilineage potential of adult human mesenchymal stem cells Science. 284(5411): 143-147.
- Caplan AI. (1991). Mesenchymal stem cells J Orthopaedic Research. 9(5): 641-650.
- Bianco P, Cao X, Frenette PS, Mao JJ, et al. (2013). The meaning, the sense and significance: translating the science of mesenchymal stem cells into medicine. Nat Med. 19 (1): 35-42.
- Caplan AL. (2017). Mesenchymal stem cells: time to change the name. STEM CELLS TRANSLATIONAL MEDICINE. 6(6): 1445- 1451.
- Grove JE, Bruscia E and Krause DS. (2004). Plasticity of bone marrow-derived stem cells STEM CELLS 2004; 22(4): 487-500.
- Friedenstein AJ, Piatetzky-Shapiro II and Peterkova KY. (1966). Osteogenesis in transplants of bone marrow cell. J Embryol exp Morph. 16(3): 381-390.
- Caplan AI. (2005). Review: Mesenchymal stem cells: Cellbased reconstructive therapy in orthopedics. Tissue Eng. 11(7-8): 1198-1211.
- Dravid G, Ye Z, Hammond H, Chen G, et al. (2005). Defining the role of Wnt/β-Catenin signaling in the survival, proliferation, and self-renewal of human embryonic stem cells. STEM CELLS. 23(10): 1489-1501.
- Barry FP and Murphy JM. (2004). Mesenchymal stem cells: clinical applications and biological characterization. Int J Biochem & Cell Biology. 36(4): 568-584
- Rodriguez-Lozano F-J, Inausti C-L, Iniesta F, Blanquer M, et al. (2012). Mesenchymal dental stem cells in regenerative dentistry. Med Oral Patol Oral Cir Bucal. 17(6): e1062- e1067.
- Caplan AI. (2007). Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. J Cellular Physiology. 213(2) : 341-347.
- Caplan AI. (2008). All MSCs are pericytes? Cell Stem Cell. 3(3): 229-230.
- Kundrotas G. (2012). Surface markers distinguishing mesenchyme stem cells from fibroblasts. Acta medica lituanica. 19(2): 75-79.
- Ankrum J and Karp JM. (2010). Mesenchymal stem cell therapy: two steps foreward, one step back. Trends Mol. 16(5): 203-209.
- Caplan AI. (2007). Adult mesenchyme stem cells for tissue engineering versus regenerative medicine. J Cell Physiol. 213(2): 341-347.
- Caplan AI. (1991). Mesenchymal stem cells J Orthopaedic Research. 9(5) : 641-650.
- Browne CM, Chung T-L and Atkinson. (2013). The biology of mesenchymal stem cells in health and disease and its relevance to MSC-based cell deliveriy therapies. Chapter 4 in « Chase LG, Vemuri MC (eds) Mesenchymal stem cell therapy Humana Press. Springer Science Business Media, New York 2013. 63- 86.
- Stolzing A, Jones E, McGolagle D and Scott A. (2008). Agerelated changes in human bone marrow-derived mesenchymal stem cells : consequences for cell therapies. Mechanisms of aging and development. 129: 163-173.
- Murray IR and Peault B. (2015). Mesenchymal stem cellswhere do they come from and is it important? BMC Biology. 13: 99.
- Minguell JJ, Reices A and Conget P. (2001). Mesenchymal stem cells. Exp Biol Med. 226(6): 507-520.