Previous Issues Volume 3, Issue 1 - 2018
Periodontal Disease - Cancer Association and the Specific Role of Periodontal Disease in Lung Cancer Pathogenesis
Nikolaos Andreas Chrysanthakopoulos
Dental Surgeon (DDSc), Oncologist, Resident in Maxillofacial and Oral Surgery, 401 General Military Hospital of Athens, Athens, Greece
Corresponding Author: Nikolaos Andreas Chrysanthakopoulos, Dental Surgeon (DDSc), Oncologist, Resident in Maxillofacial and Oral Surgery, 401 General Military Hospital of Athens, Athens, Greece, Tel: +30-2610-225288; E-Mail: nikolaos_c@hotmail
Received Date: 22 Sep 2018 Accepted Date: 24 Sep 2018 Published Date: 28 Sep 2018 Copyright © 2018 Chrysanthakopoulos NA
Citation: Chrysanthakopoulos NA. (2018). Periodontal Disease - Cancer Association and the Specific Role of Periodontal Disease in Lung Cancer Pathogenesis. Mathews J Dentistry. 3(1): 018.
ABSTRACT
Several epidemiological studies have investigated the possible role of periodontal disease as a risk factor for systemic diseases such as cardiovascular disorders, diabetes mellitus, respiratory diseases such as Chronic Obstructive Pulmonary Disease, arterial hypertension, rheumatoid arthritis, endocrine disorders, allergies, osteoporosis, cancer, etc.. In recent years, the interest has focused on the potential role of periodontal disease in the cancer pathogenesis. Several case-control studies have recorded strong associations between several parameters/indices for assessing of periodontal disease, such as tooth loss, alveolar bone loss, probing pocket depth, clinical attachment loss, gingival index, bleeding on probing and oral cancer and those associations were retained after controlling for possible confounders, such as smoking, alcohol consumption and socio-economic status. Associations have also been reported between periodontal disease or its parameters with an increased risk for cancer in locations such as the tongue, oropharynx, breast, esophagus, stomach, kidney, pancreas, hematopoietic system, colon, prostate and uterus, however few studies have investigated the possible association between periodontal disease and lung cancer. Studies in this field show differences in design and methods regarding the conditions of the periodontal tissues, as well as on the collection of information on the systemic diseases that are under investigation.
KEYWORDS
Periodontal Disease; Cancer; Inflammation.
PERIODONTAL DISEASE AND CANCER
Several epidemiological and laboratory studies have recorded that long-term inflammation promotes tumor development, growth and progression [1]. It has confirmed that malignancies can arise from areas that characterized by infection and inflammation as a part of the physiological immune response of the host. This observation suggests that chronic inflammation could be a risk factor for the development of a number of malignancies in humans, in organs such as the stomach, esophagus, liver, colon, oral cavity, head and neck, uterine cervix, ovaries, urinary bladder and lung [2, 3]. Persistent host infections are able to induce chronic inflammation in which leukocytes and others immune system's phagocytes can induce DNA damage in proliferating cells through the production of toxic substances such as Reactive Oxygen Species (ROS) and Reactive Nitrogen Intermediates (RNI) that under normal conditions are produced by those cells for the control of the infection. These species react to the formation of peroxynitrate that is a mutagenic agent. Consequently, a repeated tissue injury and the regeneration of the damaged tissue in the presence of elevated levels of ROS and RNI that are released by inflammatory cells, leads those reactive species to be involved in a oxidative DNA damage in proliferating epithelial cells leading to permanent alterations in the genome, such as point mutations, chromosomal deletions, or rearrangements [4]. (Figure 1)
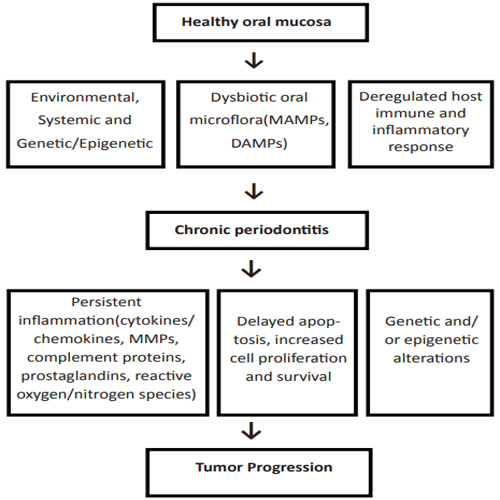
Figure 1: Periodontal disease and cancer
The link between the inflammatory response and cancer has been considered to consist of two mechanisms, an exogenous and an endogenous. According to the exogenous mechanism, a chronic inflammatory response is able to increases the risk of cancer, while in the endogenous, acquired genetic alterations can trigger tumor development and growth [3].
The chronic inflammation can stimulate the development of malignant tumors of epithelial origin due to an indirect mechanism that involves the activation of the environmental inflammatory cells. This process can also lead to the exposure of the proliferating epithelial cells to mutagens factors. Microorganisms' products that related to inflammation are able to activate the host cells, such as the inflammatory response cells, tissue's fibroblasts and epithelial cells to produce a wide spectrum of toxic substances that are able to cause a damage to the epithelial cell DNA.
Chronic inflammatory responses are often associated with the release of large amounts of cells' substances, such as chemokines, growth factors agents, cytokines, and other species that can create a suitable environment for the cellular survival, cells' proliferation and migration, promotion of angiogenesis and inhibition of apoptosis. This environment can contribute the epithelial cells to accumulate mutations and lead those mutant cells to proliferation, migrating and can provide opportunities for the development and growth of those cells [5].
The highest incidence of cancer in individuals with chronic inflammation was the basis for investigating the probability of correlation with periodontitis [6].
Recently, an association of periodontal disease (PD) with cancer was proposed, based on the fact that the inflammation is a major factor that links PD to cancer. Oral cancer, especially in the area of the gingiva, from squamous cells, imitate the advanced PD regarding the clinical Presentation showing similar clinical signs and symptoms, deep periodontal pockets, bleeding Swelling of the gingiva, tooth mobility, and bone destruction. Therefore, a similar underlying Mechanism may also be responsible for the development PD and cancer [2, 3].
PD as a chronic inflammation is caused by the colonization of Gram-negative bacteria, mainly that induce an inflammatory reaction, which in some individuals leads to the destruction of the connective tissue and the bone around the teeth [7] and is a risk factor for development of several types of cancer [6, 8-14].
The in flammatory response to periodontal pathogens extends beyond the oral cavity and leads to increased levels of circulating inflammatory biomarkers such as C-reactive protein (CRP), fibrinogen, tumor necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), adhesion molecules myeloperoxidase, enzymes, endotoxins, etc. [15]. This observation, as was reported, is confirmed by the higher incidence of cancers in individuals with chronic inflammations [6] and the effectiveness of some anti-inflammatory drugs in prevention of some types of cancer, such as the colorectal cancer [16], however this finding has not been confirmed in all studies [17,18].
The induction of systemic inflammation that results from the PD may therefore provide a pathway through the disease increases the risk for development of several types of cancer. Other mechanisms that have been proposed concern the deflection of the immune system and them production of carcinogenic products by the periodontal tissues pathogens [19]. Alternatively, possible underlying genetic factors may increase the susceptibility to both diseases or may alter the involvement of environmental risk factors, such as smoking, with PD and cancer. The role of those genetic risk factors between both diseases, however, remains unclear, while it is not known if the systemic inflammation, blood pathogenic invasion or the immune response to periodontal infection could affect the overall risk of developing cancer [20].
Recent case-control studies have recorded strong associations between teeth loss and oral cancer even after controlling of smoking and alcohol consumption as potential confounders [21, 22]. A stratified analysis showed that this association was concerned active smokers [23]. A similar case-control study recorded that the alveolar bone loss (ABL) was associated with an increased cancer incidence in the tongue regardless of the age, nationality, race, smoking status, and the number of remaining teeth. More specifically, it was recorded that for each millimeter of ABL this finding was associated with a 5.23- fold increased risk of cancer in the tongue [5]. This relation was not confirmed in a similar report, in which data collection from the medical history was limited regarding tobacco, alcohol consumption and HPV infection, which made the association with PD problematic [8]. The same researchers were reported that each millimeter of ABL was associated with a greater than 4-fold risk of squamous cell carcinoma in the area of head and neck [24]. In both studies, the use of the ABL index as a periodontitis parameter was beneficial in determining the time sequence, indicating that periodontitis is also associated with other types of cancer, such as in colon, pancreas, uterus, prostate, and breast [5, 9, 25]. Important findings were also that periodontitis that was estimated by the ABL index was associated with oro-pharyngeal cancer [26] that is caused by HPV-infection and that chronic PD, as determined by the loss of molars, was statistically significantly associated with breast cancer [5].
In a prospective study of males with a history of PD, a slightly increased total risk of death of about 14% was found in individuals who were non-smokers. In the same study, the participants showed a slightly higher incidence of cancer compared to those who did not have PD at the time of the follow-up and after controlling for smoking status and other well-known risk factors. In particular, it was found that periodontitis was statistically significantly associated with an increased risk of lung, kidney, pancreas and hematopoietic's system cancer. The examined association regarding esophageal cancer was increased but not statistically significantly, while there was no association between PD, melanoma and prostate cancer [10].
The follow-up of NHANES III patients was demonstrated that periodontitis was associated with an increased mortality from respiratory and gastrointestinal cancers, whereas was recorded a trend for an increased risk by increasing of the severity of periodontitis [27].
Recently it was found that PD was associated with a 15% increased risk for all types of cancer. In particular, increased risks for cancer of the digestive, colorectal, pancreas and prostate in males and in uterus in females that was associated with PD, was recorded. That relationship was found to be absent in monozygotic twins but remained in dizygotic twins and the conclusion was that the common genetic risk factors could only partially interpret the relationship between PD and cancer, however it was considered that the contribution of those factors was limited [25]. It has also been reported that a severe PD may be associated with a Cytomegalovirus (CMV) or Epstein-Barr virus (EBV) infection no clear results. EBV consists a risk factor for cancer, nasopharyngeal carcinoma, B-cell and Burkitt's lymphoma and [28].
PD is suggested that increases the risk of gastric non-cardia adenocarcinoma due to alterations in the oral bacterial microflora and the subsequent chronic systemic inflammation [29, 30]. However, previous researches regarding the role of PD in gastric cancer and precancerous gastric lesions have not carried out. Several oral pathogens have been linked with a chronic systemic inflammation which has also been associated with an increased risk of gastric cancer [31, 32].
Tooth loss or poor oral hygiene as markers for assessing of periodontal tissues condition have been associated with a number of cancer cases [33]. In a prospective study with a follow-up time of 16 years was found that individuals with PD and loss of molar showed an increased risk of death from neoplasms [34]. Tooth loss is caused by dental caries and PD but the contribution rate from each condition depends on the age and other factors. Tooth loss in elderly could be attributed to the chronic PD whereas in younger ages, to caries [35]. Therefore, while the loss of teeth can be an indicator of PD, the association between PD and tooth loss is not always strong. Those differences could be attributed to variations in the study design, the patient's identification, and the interpretation of the findings as well as to the inflammatory condition of the periodontium.
The relationship between chronic periodontitis and oral cancer In addition to the known risk factors for the oral squamous cell carcinoma such as the genetic Predisposition, the presence of premalignant lesions, the effect of environmental or carcinogenic factors, such as tobacco and alcohol consumption, it has been reported the role of infection and inflammation with HPV in oropharyngeal carcinomas [36]. It has also been examined the role of chronic periodontitis in the oral cancer development [9, 19]. Indeed, in a recent study was observed that the bone loss as a clinical sign of chronic periodontitis was an independent risk factor for the development of cancer in the oral cavity [24].
The investigation was focused on the development of several cancer types and in their associations with the inflammation and also to the underlying pathophysiological mechanisms that could lead to malignant cellular transformation [32]. An important factor in inflammation associated cancer is NF-?B transcription factor. In addition to its function as a basic regulator of the innate inflammation and immunity through an activated expression of inflammatory biomarkers such as cytokines, chemokines, adhesion molecules, proteolytic enzymes, angiogenic factors and a wide spectrum of toxic metabolic cellular substances, it has been identified as an endogenous tumor promoter [37], while it participates substantially in the inflammatory reaction in chronic periodontitis [38].
An association between oral cancer and the chronic mechanical injury has been reported, indicating that inflammation, regardless of its cause, can predispose to cancer development [39]. Thus, the malignant transformation of the oral epithelial cells could be a consequence of an immune response via the release of activated T-cells substances, such as cytokines IL-1, IL-8 and TNF-a [37].
That association is biologically possible and could be interpreted on the basis of the following mechanisms [40]:
- The disrupted mucosal barrier in cases of PD and a consequent enhanced carcinogen penetration, such as smoking and alcohol,
- Through an increased cell load in the blood vessels and the connective tissue in case of a chronic inflammatory response. The relationship between chronic inflammation and cancer is associated with the development of a chronic diffuse hyperplasia of the epithelial cells that is considered as a common precursor of the intraepithelial neoplasia,
- Through an immunosuppression as a common mechanism that leads to PD and oral cancer,
- Through the presence of viruses such as HPV and HSV1 or the fungus Candida Albicans as they have been isolated in both oral cancer and PD,
- Through a bacterial overgrowth in poor oral hygiene patients that can lead to an increase in the in the percentage of metabolites with a potential carcinogenic effect,
- Through the common genetic risk factors, such as in dizygotic twins, the classic PD leads to a significantly increased risk for cancer development, whereas in onozygotic twins this association was significantly impaired [25].
Recent studies were reported that some viruses such as HP, CM and EB have been implicated in oral cancer etiology and has been reported that are present in periodontal pockets and in dental plaque [41, 42].
Chronic periodontitis as a risk factor for cancer in pancreas
Pancreatic cancer is a severe and rapidly lethal type of cancer. Smoking consists the only documented risk modifier factor, however it has been suggested that diabetes mellitus, insulin resistance and obesity are also risk factors, whereas alcohol consumption is not a documented risk factor for pancreatic cancer. However, a strong association between alcohol consumption and chronic pancreatitis has been recorded and, in turn, chronic pancreatitis has been linked with an increased risk for pancreatic cancer development. It has been suggested that viral infections have been strongly associated with the development of several types of cancer, a great number of bacteria are able to initiate or promote an abnormal cell growth by skipping the immune system or by suppressing the apoptosis .Since periodontitis consists a chronic infection that is caused by oral bacterial, few investigators have proposed a possible positive link between both diseases. Chronic periodontitis can promote carcinogenesis in pancreas through a systemic inflammatory response or alternatively through an increased production of carcinogens substances, such as nitrosamines. Nitrosamines and gastric acidity have been considered as factors that play an important role in pancreatic carcinogenesis. The endogenous production of nitrosamines in the oral cavity in poor oral hygiene individuals could be attributed to high concentrations of oral bacteria including H. pylori that can eliminate the nitrates. The relationship between H.pylori infection and pancreatic cancer development has been investigated, however that relationship was not confirmed [9].
In a recent research was recorded a positive association between periodontitis and the pancreatic cancer risk. Two enzymes, myeloperoxidase and superoxide dismutase contribute to the regulation of the inflammation and those enzymes have been found in elevated levels in periodontitis, whereas the polymorphisms of those genes have been linked with an increased risk for pancreatic cancer [9, 10].
Chronic periodontitis as a risk factor for cancer in pancreas H.Pylori infections are widespread and could contribute to major medical disorders, such as gastritis, gastric cancer or lymphoma. Previous studies have recorded that H. pylori is present in the dental plaque, in a small number and in different locations in the same mouth. A link between H. pylori and peptic ulcers and gastric cancer development has been recorded, whereas it has been isolated from the sub-gingival biofilm structure in individuals that were suffered from with chronic periodontitis and characterized by poor oral hygiene [43]. (Figure 3) H. pylori infection role in the progressive cellhistological differentiation that is linked with gastric cancer has been determined through the pathways that can lead to the production of substances that are able to cause oxidative stress and molecular damage in DNA in conjunction with endogenous and exogenous mechanisms, such as ROS production and other DNA oxidative factors [44].
Periodontitis as an inflammatory disease contributes to continuous low grade systemic inflammation with elevated circulating inflammatory indicator levels [15, 45]. Specifically recognized inflammation markers, including pro-inflammatory plasma cytokines, peripheral leukocytes, prostanoids, proteases and in particular Matrix Metalloproteinases (MMPs) and acute inflammation's phase proteins [32,45] are produced by the immune system in response to the periodontal tissue pathogens. The type of the chronic inflammation that is induced by the periodontal pathogens can lead to disturbance of the normal control of cell growth and to potential carcinogenesis [6].
Alternatively, the immune system in an individual with chronic PD may be deficient in surveillance process for the tumor development. Therefore, periodontitis is considered as an indicator of the immune system function that has potential effects on the tumor's development and progression. Another mechanism by which the above suggestions could be explained is the increased production of carcinogenic nitrosamines. The formation of the endogenous carcinogenic nitrosamines in the oral cavity could be attributed to the microorganisms that colonize it, while its levels grow because of the poor oral hygiene, PD, smoking and nutritional factors [46, 47].
HYPOTHESES ON THE RELATIONSHIP BETWEEN PD AND CANCER
A. Alteration in oral microflora
It has been proposed that PD metabolic products that may act as carcinogenic could interpret the association between the two diseases. The mechanism that could increase the risk for gastric cancer could be attributed to the production of nitrosamines in increased levels in individuals with poor oral hygiene and that those products may function as gastro- intestinal special carcinogens that are able to increase the risk for cancer development in the stomach and esophagus. An inflammation that is caused by H. pylori infection has been associated with an abnormal DNA-Methylation in gastric epithelial cells and it increases the risk of gastric cancer development.
From a periodontal point of view, a wide variety of oral microorganisms, oral bacteria and their metabolic products such as endotoxins, enzymes, that are toxic to the surrounding cells and tissues may directly induce mutations in tumor suppressor genes and proto-oncogenes or are able to alter cellular signaling pathways that affect the epithelial cells survival or the cellular proliferation [47,48]. (Figure 2, 3)
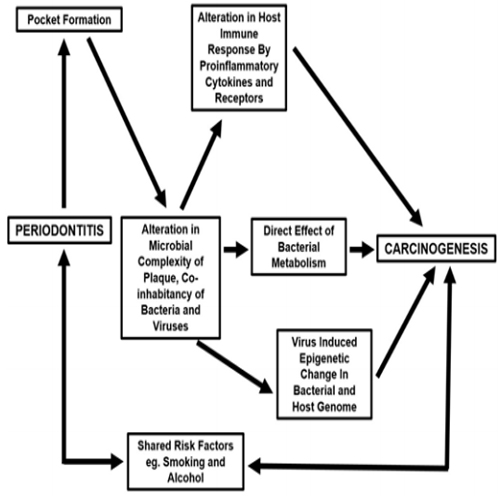
Figure 2: Periodontitis and Carcinogenesis.
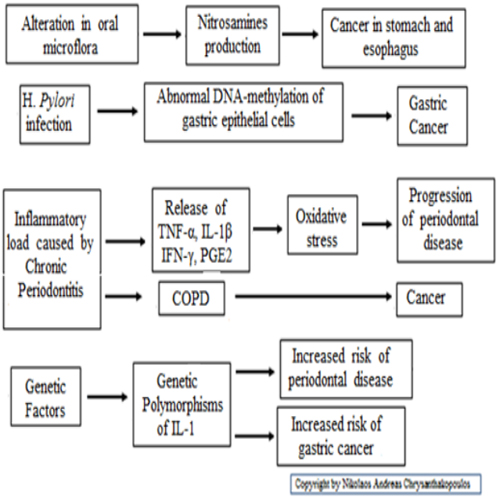
Figure 3: Mechanisms of periodontal disease that cause cancer.
B. Chronic periodontitis, inflammatory load and predisposition for carcinogenesis
Chronic periodontitis that affects the periodontal tissue leads to the release of cytokines, chemokines, prostaglandins (PGs), bacterial toxins , endotoxins and enzymes from the host's cells and have destructive effects on tissues, leading to periodontal pocket formation that can lead to the alveolar bone destruction [7]. Pro-inflammatory cytokines such as TNF-α, IL-1β, IFN-? and PGE2 are present in elevated levels in chronic periodontitis. The periodontal tissue can also act as a refreshment tank for the leakage of those mediators that enter the blood circulation and can cause systemic effects [49].
A link between PD and pancreatic cancer has been recorded in a population of health professionals and the conclusion was that the mechanisms that are associated with the inflammatory load due to systemic inflammation and the increased concentrations of carcinogenic products in response to the oral pathogens due to subsequent inflammatory processes, could contribute to the development of cancer [9].
In general, in those studies, parameters such as tobacco and alcohol consumption and nutrition factors, stress, socio-economic level, condition of immune system and body mass index (BMI) make difficult to find out independent associations. A large inflammatory load attributable to PD could be associated with the risk of cancer through the mechanisms that are involved and lead to oxidative stress that can cause damage to periodontal tissues. The oxidative stress induces mechanisms in the progression of PD and cancer. Several types of PD are characterized by considerable inflammatory load that are able to affect the progression of systemic diseases, including carcinogenesis. The link between chronic periodontitis and cancer was investigated in a follow-up study of 11,328 individuals aged 25-74 years and it was found that individuals with periodontitis showed significantly higher risk of death from cancer. More significant association was found for the cases with lung cancer while there was some evidence of association with cancer in prostate, breast and pancreas. In cases the results were concerned nonsmokers no relationship was found between both diseases. Gingivitis that reflects an index of inflammatory load in individuals without artificial denture showed elevated risk levels of death from lung cancer. In this study, the estimation of the relationship between periodontal tissues condition and lung cancer was estimated using the Cox analog model and the assessment was concerned whether individuals with gingival, periodontal inflammation or with out natural teeth showed a higher risk for lethal malignant neoplastic alteration in the bronchi and lung compared to individuals with healthy periodontal tissue for a period of 10 years. Periodontitis may be a substitute indicator for the effects of smoking and therefore could provide a relationship with lung cancer. It is relevant that cigarette smoking is responsible for the oxidative stress and activates processes that could contribute to epithelial cell transformation whereas the degree of the periodontal inflammatory load would be an important factor with a systemic effect in the case of periodontitis and other systematic associations [8]. (Figure 2, 3)
C. Genetic factors Common underlying genetic factors may increase the host's susceptibility to both conditions or may alter the relationship of the environmental factors, such as smoking, with PD and cancer. However, the common genetic risk factors role between the two situations, remains unclear. Predetermined factors such as genetic polymorphisms could be involved to the sensitivity of the disease. As has already reported the inflammatory response may play a role in some cancers and it is possible that the genetic polymorphisms that are related to an increased PD risk are also of a vital importance in cancer development [6,11]. An example consists the presence of genetic polymorphisms in IL-1that have been linked with an elevated risk of gastric cancer [50]. For the time being, the relationship between genetic polymorphisms of cytokines and other factors for cancer development are unclear and therefore it is not possible to identify specific genetic factors that may be etiologically related to PD and specific types of cancer [51]. (Figure 2, 3).
The specific role of periodontal disease in lung cancer pathogenesis There have been serious indications that poor oral hygiene could be a predatory factor for respiratory disorders, particularly in high risk patients. The oral cavity coincides with the trachea and consists a gate for colonization by respiratory pathogens. Similarly, respiratory pathogens are able to colonize the dental plaque that are inhaled from the oropharynx to the upper airways and then are able to approach the lower airway and adhere to the alveolar or bronchial epithelial cells [52, 53].
Chronic PD has been found to be associated with chronic lung disease [54, 55]. In another report was observed that pulmonary function in COPD patients decreases with increasing CAL, whereas in the same study, a relationship between poor oral hygiene and COPD after controlling for potential confounders, such as smoking, gender, age and socio-economic level, was found [56]. A relevant case-control study was recorded that individuals with poor oral and periodontal health and the lack of a regular dental and oral follow-up were associated with an increased risk of developing COPD [57]. In a 25-year prospective study, it was observed that ABL was an independent risk factor for COPD development, and individuals with severe alveolar bone loss showed a higher risk for COPD development developing during their follow-up [58].
An epidemiological systemic review found that poor periodontal condition was an independent predictor for COPD after adjustment for smoking, while periodontitis could be a co-worker for COPD [59]. A threefold increase in COPD among smokers that were suffered from severe periodontitis and the fact that smoking should be seen as an effect modifier in each relationship between periodontitis and COPD have also been observed [60]. The investigation of the examined relation in individuals 70-79 years of age showed an association between periodontitis and COPD in former smokers, but not in never smokers, whereas no link was observed among current smokers, however the assessing of all periodontal indices were at increased levels in current smokers independently from their pulmonary health condition [61].
In a relevant case-control study was observed that probing pocket depth, clinical attachment loss, bleeding on probing as indices for periodontal disease severity and assessing, and smoking were statistically significantly associated with the risk of developing lung cancer. The mentioned association regarding probing pocket depth and the risk for lung cancer development was remained after adjusting for known confounders, such as smoking and dental follow-up [14]. Similar studies have not confirmed such findings. In a similar case-control report in a hospital Population, after adjustment for smoking, no significant relationship between periodontitis and COPD, was observed [57],while a weak relationship between oral health and COPD was recorded in another study [62].
The relationship between COPD and lung cancer is considered as documented epidemiologically [63-65]. Cigarette smoking is the most important risk factor for developing COPD [66] and lung cancer [63, 64, 68]. Smokers with COPD are at a higher risk for developing cancer, suggesting that a link exists between the processes that cause COPD and those that cause lung cancer [69, 70]. However, the majority of smokers do not develop COPD or lung cancer despite the fact that the accumulated smoking history increases the risk of developing PD and cancer [69, 71, 72]. Smokers show also a significantly elevated risk for developing chronic periodontitis [73-75] than non-smokers [76,77].
The contribution of smoking to PD development requires other factors such as poor oral hygiene while in cases of established PD smoking accelerates its progression. Similarly, smoking consists an important risk factor for lung cancer development, however does not cause the disease to all smokers, current or former. [77].
The association between PD and lung cancer may be mediated by a pre-existing chronic pulmonary disease such as COPD, idiopathic pulmonary fibrosis and tuberculosis that are in relation with an increased possibility of lung cancer [64]. There has been a limited exploration between COPD and lung cancer risk, especially in non-smokers as they develop COPD rarely. In a study with females that were exposed to pollutants, it was found that COPD, mainly in the form of bronchial asthma and in non-smokers, was found to be associated with an increased risk of lung cancer [78].
In a prospective study in males with a PD history, a slightly increased overall risk of death was found, approximately 14% in non-smokers. In the same study, the participants showed a slightly higher cancer incidence compared to those who did not have PD at the time of the study initiation and after controlling for known risk factors. It was also found that PD was statistically significantly associated with an increased risk for lung cancer. Specifically, regarding lung cancer, a strong association was observed in individuals with a small number of remaining teeth and it was remained strong among nonsmokers although it was weaker and statistically insignificant. In the study many limitations were existed especially the selfreported assessment of PD [10].
An increased risk of death from all types of cancer was also recorded in the case the assessment of PD was based on other indicators. Specifically, it was found a significantly increased risk of lung cancer, however it was not confirmed in nonsmokers. It was suggested that periodontitis could include an unlimited percentage of smoking history, and therefore its relationship with the lung cancer was invalid. In the same study, gingivitis that reflects the presence of inflammatory load, in individuals with natural teeth showed increased risk levels of death from lung cancer. Chronic periodontitis could be a substitute indicator for the effects of cigarette smoking and consequently it provides a link to lung cancer [8].
The follow-up of NHANES III patients was shown that periodontitis was associated with an increased mortality from respiratory cancers. There was an increased risk tendency in relation to periodontitis severity [25].
?n addition to the suspected effect of COPD and smoking on the interpretation of the association between PD and the risk for developing of lung cancer, the mechanisms that could link the two diseases have not been elucidated. Therefore, future studies are required, and they could be based on the overall association between chronic inflammation and the risk of cancer development. The inflammatory response to periodontal infection can extend beyond the oral cavity and leads to increased levels of circulating inflammatory biomarkers, such as cytokines, chemokines, enzymes etc. [15,45], an observation that is confirmed from the highest incidence of cancer cases in individuals with chronic inflammatory diseases [12] and the efficacy of anti-inflammatory drugs in the prevention of certain types of cancer [24], however that finding has not been confirmed in all studies [33,34], nor in lung cancer.
A possible mechanism could be supported according to the basis of the PD pathogenesis and is characterized by a wide spectrum of oral bacteria and microorganisms, and their products such as metabolic toxic substances, endotoxins, enzymes and products that are toxic to surrounding tissues and cells and could directly induce mutations in tumor suppressor and proto-oncogenes or are able to alter cellular signaling pathways that affect epithelial cell survival and/or cell proliferation [47,48].
Other mechanisms that have been proposed include the immune system deflection and the production of carcinogenic products by periodontal tissues pathogens [35]. In addition, underlying genetic factors may increase the sensitivity in both situations or may alter the relationship of environmental risk factors such as smoking, with PD and cancer. The common genetic risk factors role between the two conditions, however, remains unclear. Predetermined factors such as genetic polymorphisms could be influence the host's sensitivity to the disease, however that issue also need to be investigated [6, 11].
Another possible mechanism could be attributed to the large inflammatory load caused by the PD and could be associated with the risk of lung cancer through the mechanisms that are involved and lead to oxidative stress that causes injury to the tissues. The oxidative stress induces mechanisms that are involved in the progression of PD and cancer. Various types of PD are characterized by significant inflammation load that could affect the evolution of systematic conditions, including carcinogenesis in the lung [8]. (Figure 3).
It should be noted that the research regarding the possible association of PD with cancer is limited by the problems of controlling of confounders such as smoking and the socioeconomic level. Smoking seems to be the main confounding factor in studies that examine cancer, such as lung cancer. Other possible confounders are gender, age, nationality, diabetes mellitus and genetic factors. The definition of periodontitis in a number of large epidemiological studies was based on substitute indicators [25]. However, despite several limitations, chronic periodontitis has been identified as a potential risk factor for gastrointestinal, respiratory and pancreatic cancer and possibly for cancer in other organs [79]. Therefore, it exists an obvious need for further investigation.
REFERENCES
- Balkwill F and Mantovani A. (2001). Inflammation and cancer: back to Virchow? Lancet. 357(9255): 539-545.
- Kuper H, Adami HO and Trichopoulos D. (2000). Infections as a major preventable cause of human cancer. J Intern Med. 248(3): 171-183.
- Shacter E and Weitzman SA. (2002). Chronic inflammation and cancer. Oncology. 16(2): 217-226.
- Maeda H and Akaike T. (1998). Nitric oxide and oxygen radicals in infection, inflammation, and Cancer. Biochem. 63(7): 854-865.
- Soder B, Yakob M, Meurman JH, Andersson LC, et al. (2011). Periodontal disease may Associate with breast cancer. Breast Canc Res Treatm. 127(2): 497-502.
- Coussens LM and Werb Z. (2002). Inflammation and cancer: Nature. 420(6917): 860-867.
- Pihlstrom BL, Michalowics BS and Johnson NW. (2005). Periodontal diseases. Lancet. 366(9499): 1809- 1820.
- Hujoel PP, Drangsholt M, Spiekerman C and Weiss N. (2003). An exploration of the periodontitis cancer association. Ann Epidemiol. 13(5): 312-316.
- Michaud DS, Joshipura K, Giovannucci E and Fuchs CS. (2007). A prospective study of Periodontal disease and pancreatic cancer in US male health professionals. J Natl Cancer Inst. 99(2) :171-175.
- Michaud DS, Liu Y, Meyer M, Giovannucci E, et al. (2008). Periodontal disease, tooth loss, and cancer risk in male health professionals: a prospective cohort study. Lancet Oncol. 9(6): 550-558.
- Marx J. (2004). Cancer research. Inflammation and cancer: the link grows stronger. Science. 306(5698) : 966-968.
- Erlinger TP, Platz EA, Rifai N and Helzlsouer KJ. (2004). Creactive protein and the risk of incident colorectal cancer. J Am Med Assoc. 291(5): 585-590.
- Heikkila K, Harris R, Lowe G and Rumley A. (2009). Association of circulating C-reactive protein and interleukin-6 with cancer risk: findings from two prospective cohorts and a meta-analysis. Canc Caus Control. 20(1): 15-26.
- Chrysanthakopoulos NA (2016). Correlation between Periodontal Disease Indices and Lung Cancer in Greek Adults: a Case - Control study. Experim Oncol. 38(1): 49- 53.
- Amabile N, Susini G, Pettenati-Soubayroux I, Bonello L, et al. (2008). Severity of periodontal disease correlates to inflammatory systemic status and independently predicts the presence and angiographic extent of stable coronary artery disease. J Intern Med. 263(6): 644-652.
- Baron JA, Cole BF, Sandler RS, Haile RW, et al. (2003). A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med. 348: 891-899.
- Cook NR, Lee IM, Gaziano JM, Gordon D, et al. (2005). Low-dose aspirin in the primary prevention of cancer: the Women's Health Study: a randomized controlled trial. J Am Med Assoc. 294(1): 47-55.
- Marshall SF, Bernstein L, Anton-Culver H, Deapen D, et al. (2005). Non-steroidal anti-inflammatory drug use and breast cancer risk by stage and hormone receptor status. J Natl Canc Inst. 97(11): 805-812.
- Meyer MS, Joshipura K, Giovannucci E and Michaud DS (2008). A review of the relationship between tooth loss, periodontal disease, and cancer. Cancer Causes Control. 19(9): 895-907.
- Renvert S, Lindahl C, Roos-Jansaker AM and Lessemi J (2009). Short-term effects of an anti-inflammatory treatment on clinical parameters and serum levels of C - reactive protein and pro-inflammatory cytokines in subjects with periodontitis. J Periodontol. 80(6): 892-900.
- Garrote LF, Herrero R, Reyes RM, Vaccarella S, et al. (2001). Risk factors for cancer of the oral cavity and oropharynx in Cuba. Br J Cancer. 85(1): 46-54.
- Rosenquist K. (2005). Risk factors in oral and oropharyngeal squamous cell carcinoma: a population-based case-control study in southern Sweden. Swed Dent J Suppl. 179: 1-66.
- Tezal M, Grossi SG and Genco RJ (2005). Is periodontitis associated with oral neoplasms? J Periodontol. 76(3): 406-410.
- Tezal M, Sullivan MA, Hyland A, Marshall JR, et al. (2009). Chronic periodontitis and the incidence of head and neck squamous cell carcinoma. Cancer epidemiology biomarkers and prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 18(9): 2406-2412.
- Arora M, Weuve J, Fall K, Pedersen NL, et al. (2010). An exploration of shared genetic risk factors between periodontal disease and cancers: a prospective co-twin study. Amer J Epidemoil. 171(2): 253-259.
- Tezal M, Scannapieco FA, Wactawski-Wende J, Hyland A, et al. (2012). Local inflammation and human papillomavirus status of head and neckcancers. Arch Otolaryngol Head Neck Surg. 138(7): 669-675.
- Ahn J, Segers S and Hayes RB (2012). Periodontal disease, Porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis. 33(5): 1055- 1058.
- Buchmann R, Muller RE, Heinecke A, Lange DE. (2000). Actinobacillus actinomycetem-comitans in destructive periodontal disease. Three-year follow-up results. J Clin Periodontol. 71(3): 444-453.
- Abnet CC, Qiao YL, Mark SD, Dong ZW, et al. (2001). Prospective study of tooth loss and incident esophageal and gastric cancers in China. Cancer Cause Control. 12(9): 847-854.
- Abnet CC, Kamangar F, Dawsey SM, Stolzenberg-Solomon RZ, et al. (2005). Tooth loss is associated with increased risk of gastric non-cardia adenoma in a cohort of Finnish mokers. Scand J Gastroenterol 40(6): 681-687.
- Loos BG. (2005). Systemic markers of inflammation in periodontitis. J Periodontol 76. (11 Suppl): 2106-2115.
- Moss SF and Blaser MJ. (2005). Mechanisms of disease: inflammation and the origins of cancer Nat Clin Pract Oncol. 2(2): 90-97.
- Fitzpatrick SG and Katz J. (2010). The association between periodontal disease and cancer. A review of the literature. J Dent. 38(2): 83-95.
- Soder B, Jin LJ, Klinge B and Soder PO. (2007). Periodontitis and premature death: a 16-year longitudinal study in a Swedish urban population. JPeriodontal Res. 42(4): 361-366.
- Chrysanthakopoulos NA and Vlassi C. (2013). Reasons for Extraction of Permanent Teeth and Risk Indicators in a General Dental Practice in Greece. Int J Med Dent. 3: 315-321.
- Tezal M, Nasca MS, Stoler DL, Melendy T, et al. (2009). Chronic periodontitis-human papillomavirus synergy in base of tongue cancers. Arch Otolaryngol. 135(4): 391- 396.
- Karin M. (2006). Nuclear factor-kappa B in cancer development and progression. Nature. 441(7092): 431-436.
- Nagahama Y, Obama T, Usui M, Kanazawa Y, et al. (2011). Oxidized low-density lipoprotein induced periodontal inflammation is associated with the up-regulation of cyclooxygenase-2 and microsomal prostaglandin synthase 1 in human gingival epithelial cells. Biochem Biophys Res Commun. 413(4): 566-571.
- Piemonte ED, Lazoa JP and Brunotto M. (2010). Relationship between chronic trauma of the oral mucosa, oral potentially malignant disorders and oral cancer. J Oral Pathol Medic. 39(7): 513-517.
- Tezal M, Sullivan M, Reid M, Marshall JR, et al. (2007). Chronic periodontitis and the risk of tongue cancer. Arch Otolaryngol Head Neck Surg. 133(5): 450-454.
- Hormia M, Willberg J, Ruokonen H, Syrjanen S. (2005). Marginal periodontium as a potential reservoir of human papillomavirus in oral mucosa. J Periodontol. 76(3): 358-363.
- Saygun I, Kubar A, Ozdemir A, Slots J. (2005). Periodontitis lesions are a source of salivary cytomegalovirus and Epstein-Barr virus. J Periodontal Res. 40(2): 187-191.
- Gebara ECE, Pannuti C, Faria CM, Chehter L, et al. (2004). Prevalence of Helicobacterpylori detected by polymerase chain reaction in the oral cavity of periodontitis patients. Oral Microbiol Immunol. 19(4): 277-820.
- Farinati F, Cardin R, Cassaro M, Bortolami M, et al. (2008). Helicobacter pylori inflammation, oxidative damage and gastric cancer: a morphological, biological and molecular pathway. Eur J Cancer Prev. 17(3): 195-200.
- Moutsopoulos NM and Madianos PN. (2006). Low grade inflammation in chronic infectious diseases: paradigm of periodontal infections. Ann NY Acad Sci. 1088: 251-264.
- Nair J, Ohsima H, Nair UJ and Bartsch H. (1996). Endogenous formation of nitrosamines and oxidative DNAdamaging agents in tobacco users. Crit Rev Toxicol. 26(2): 149-161.
- Abnet CC, Qiao YL, Dawsey SM, Dong ZW, et al. (2005). Tooth loss is associated with increased risk of total death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int J Epidemiol. 34(2): 467-474.
- Zaris S, Bojic B, Jankovic L, Dapcevic B, et al. (2009). Periodontal therapy improves gastric Helicobacter pylori eradication. J Dent Res. 88(10): 946-950.
- Page RC. (1998). The pathobiology of periodontal diseases may affect systemic diseases: inversion of a paradigm. Ann Periodontol. 3(1): 108-120.
- El-Omar EM, Carrington M, Chon WH, McColl KE, et al. (2000). Interleukin-1 polymorphisms associated with increased risk of gastric cancer. Nature. 404(6776): 398- 402.
- Kamangar F, Cheng C, Abnet CC and Rabkin CS. (2006). Interleukin-1B polymorphisms and gastric cancer risk- a meta-analysis. Cancer Epidemiol Biomarkers Prev. 15(10): 1920-1928.
- Didilescu AC, Skaug N, Marica C and Didilescu C. (2005). Respiratory pathogens in dental plaque of hospitalized patients with chronic lung diseases. Clin Oral Investig. 9(3): 141-147.
- Scannapieco FA. (1999). Role of oral bacteria in respiratory infection. J Periodontol. 70(7):793- 802.
- Deo V, Bhongade ML, Ansari S and Chavan RS. (2009). Periodontitis as a potential risk factor for chronic obstructive pulmonary disease: a retrospective study. Indian J Dent Res. 20(4): 466-470.
- Sharma N and Shamsuddin H. (2011). Association between respiratory disease in hospitalized patients and periodontal disease: a cross-sectional study. J Periodontol. 82(8): 1155-1160.
- Scannapieco FA and Ho AW. (2002). Potential associations between chronic obstructive pulmonary disease and periodontal disease: analysis of National Health and Nutrition Examination Survey III. J Periodontol. 72(1): 50-56.
- Wang Z, Zhou X, Zhang J, Zhang L, et al. (2009). Periodontal health, oral health behaviours, and chronic obstructive pulmonary disease. J Clin Periodontol. 36(9): 750-755.
- Hayes C, Sparrow D, Cohen M, Vokonas PS, et al. (1998). The association between alveolar bone loss and pulmonary function: the VA Dental Longitudinal Study. Ann Periodontol. 3(1): 257-261.
- Garcia RI, Nunn ME and Vokonas PS. (2001). Epidemiologic associations between periodontal disease and chronic obstructive pulmonary disease. Ann Periodontol. 6(1): 71-77.
- Hyman JJ and Reid BC. (2004). Cigarette smoking, periodontal disease, and chronic obstructive pulmonary disease. J Periodontol. 75(1): 9-15.
- Katancil JA, Kritchevsky S, Weyant RJ, Corby P, et al. (2005). Periodontitis and airway obstruction. J Periodontol. 76(11 Suppl): 2161-2167.
- Azarpazhooh A and Leake JL. (2006). Systematic review of the association between respiratory diseases and oral health. J Periodontol. 77(9): 1465-1482.
- Alberg AJ and Samet JM. (2003). Epidemiology of Lung Cancer. Chest. 123(1 Suppl): 21S-49S.
- Thun MJ, Henley SJ, Burns D, Jemal A, et al. (2006). Lung cancer death rates in lifelong non-smokers. J Nat Canc Inst. 98(10): 691-699.
- Burcham PC. (1998). Genotoxic lipid peroxidation products: Their DNA damaging pro-perties and role in formation of endogenous DNA adducts. Mutagenesis. 13(3): 287-305.
- Waldner MJ and Neurath MF. (2009). Colitis-associated cancer: the role of T cells in tumor development. Semin. Immunopathol. 31(2): 249-256.
- Carmella SG, Hans S, Fristad A, Yang Y, et al. (2003). Analysis of total 4-(methylnitrosamino)-1-(3-pyridyl)-1-butano (NNAL) in human urine. Cancer Epidemiol Biomarkers Prev. 12: 1257-1261.
- Ezzati M and Lopez AD. (2003). Estimates of global mortality attributable to smoking in 2010. Lancet. 362(9387): 847-852.
- Mannino DM, Aguayo SM, Petty TL and Redd CS. (2003). Low lung function and incident lung cancer in the United States: data from the First National Health and Nutrition Examination Survey follow-up. Arch. Intern Med. 163(12): 1475-1480.
- Lange P, Nyboe J, Appleyard M, Jensen J, et al. (1990). Ventilatory function and chronic mucus hyper-secretion as predictors of death from lung cancer. Am Rev Respir Dis. 141(13): 613-617.
- Prendergast GC. (2008). Inflammatory mediators in cancer etiology and targets for therapy and prevention. Can Rev Onl. 9: 17-18.
- Taraseviciene-Stewart L and Voelkel NF. (2008). Molecular pathogenesis of emphysema. J Clin Invest. 118(2): 394- 402.
- Albandar JM. (2005). Epidemiology and risk factors of periodontal disease. Dent Clin North Am. 49(3): 517-532.
- Haubek D, Ennibi OK, Abdellaoui L, Benzarti N, et al. (2002). Attachment loss in Moroccan early onset periodontitis patients and infection with the JP2-type of Actinobacillus actinomycetemcomitans. J Clin Periodontol. 29(7): 657-660.
- Carranza FA. Chapter 26. (2006). Environmental and behavioural factors in chronic periodontitis In: Newman, Takei, Carranza, editors. Text book of Carranza's clinical periodontology. 10th ed St Louis: Missouri Saunders. Elsevier. 401.
- Grossi SG, Zambon JJ, Ho AW, Koch G, et al. (1994). Assessment of risk for periodontal disease. Risk Indicators for attachment loss. J Periodontol. 65(3): 260-267.
- Tomar SL and Asma S. (2000). Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol. 71(5): 743-751.
- Danaei G, Vander Hoom S, Lopez AD, Murray CJ, et al. (2005). Causes of cancer in the world: comparative risk assessment of nine behavioural and environmental risk factors. Lancet. 366(9499): 1784-1793.
- Milasin J, Jakoba NN, Stefanovic D, Sopta J, et al. (2011). Periodontal Inflammation as Risk Factor for Pancreatic Diseases. 131-156.