Previous Issues Volume 1, Issue 2 - 2016
The Protocol Study, Multicentre Evaluation of Oral Health in Persons with Schizophrenia: a Cross-Sectional Study
Frederic Denis1, Isabelle Millot7, Nicolas Abello3, Maud Capentier3, Lysiane Jonval3, Corinne Rat1, Souad Maach1, Gerard Milleret1, Thomas Wallenhorst4, Jean-pierre Capitain1, Jean-francois Pelletier6, Benoit Trojak5, Agnes Soudry Faure2
1La Chartreuse Psychiatric Centre, 21033 Dijon, France.
2USMR-Reseau d'aide Methodologiste, University Hospital of Dijon, 21079 Dijon Cedex, France.
3Direction de la Recherche Clinique, University Hospital of Dijon, 21079 Dijon Cedex, France.
4Department of Psychiatry, Robert Morlevat Hospital Center, 21140 Semur-en-Auxois, France.
5Department of Psychiatry and Addictology, University Hospital of Dijon, 21079 Dijon Cedex, France.
6Department of Psychiatry, Montreal University, Yale Program for Recovery and Community Health, 7401 Montreal, Canada.
7Regional forum of education and health promotion, 21000 Dijon, France.
Corresponding Author: Frederic denis, La Chartreuse Psychiatric Centre, Dijon, France, 1, boulevard Chanoine Kir, BP 23314,21033 Dijon Cedex, Tel: +33 3 80 42 52 35; Email: [email protected]
Received Date: 20 Feb 2016 Accepted Date: 23 Mar 2016 Published Date: 29 Mar 2016 Copyright © 2016 Denis F
Citation: Denis F, Millot I, Abello N, Carpentier M, et al. (2016). The Protocol Study, Multicentre Evaluation of Oral Health in Persons With Schizophrenia: a Cross-Sectional Study. Mathews J Dentistry. 1(1): 006.
ABSTRACT
Background:
Schizophrenia is a severe mental disorder that involves 1% of the world's population. It affects 600,000 people in France. Schizophrenic persons have excess mortality (their life expectancy is reduced by 20%) and have excess morbidity. One of the most visible elements of poor oral health is edentulousness, but also a large number of missing or decayed teeth (leading to pain, infection, masticatory and digestive problems) can be noticed. Few data have been published on the subject in France. It is therefore difficult to have a clear idea of the oral health of in- or outpatients. In this context, we hypothesize that the evaluation of oral health of randomly selected schizophrenic persons will be more representative of a population of schizophrenic persons than results obtained to date by prospective ways.
Methods/design
We report the protocol of a cross-sectional study. This study will be conducted in three centres in France. In total, 120 persons of both sexes, aged over 18years and diagnosed with schizophrenia, will be investigated to assess their dental status and oral hygiene, and their perceptions of oral health. We will also evaluate socio-demographic data.
Discussion
In all the published studies, screening is often performed on institutionalized persons and inclusion is prospective without random selection, with occasionally a modest sample size, which limits interpretation of the results. We can therefore assume that the published data only partially reflect the oral health status of these populations. Results from this cross-sectional study will provide a better overview of the level of oral health of these cases in Cote d'Or (France).
KEYWORDS
Dental Health; Oral Health; Schizophrenia; Periodontal; Dental Hygiene; Dental Education.
TRIAL REGISTRATION:
Clinical Trials Gov NCT02512367.
LIST OF ABBREVATIONS
Committee for the Protection of Persons (CPP); International Classification of Disease ten revision (ICD-10); Medical informatics departments (MID); Decayed Missing or Filled Teeth (DMFT); WHO (World Health Organization); University hospital Dijon (UHD); Case Report Form (CRF); Simplified Oral Hygiene Index (OHI-S); Oral Health related Quality of Life (OHRQoL); the Global Oral Health Assessment Index (GOHAI); Standard Deviation (SD); Confidence Interval (CI).
INTRODUCTION
Background:
Schizophrenia is a severe mental disorder that involves 1% of the world's population [1,2]. It affects 600,000 people in France. Schizophrenic patients have excess mortality (their life expectancy is reduced by 20%) and have excess morbidity [3]. Among somatic comorbidities in schizophrenia persons, poor oral health has been reported by many authors and contributes to the overall poor health of these patients [4,5]. Generally, the symptoms of schizophrenia lead to disturbances in the progression of thought, errors in contextual analysis and errors of logic. Often persons with schizophrenia do not recognize their health needs and delay seeking advice or treatment [6].
This is the case for all related somatic disorders that, by lack of analysis due to this pathology, prevent the persons recognising the condition or causes him not to make the right decisions to solve problems independently. Moreover, difficult relations with professional careers (fear of mental illness, lack of training) and the health system in general (difficulties in accessing the private practice, environment, cost ...) are additional obstacles contributing to a deficient somatic care [7].
Poor dietary behaviours affect the level of oral health. For example, vitamin C is essential for the formation and maintenance of intracellular material which forms the dental supporting tissue. Chronic or severe vitamin C deficiency in may lead to tooth loss [11-14]. In psychiatric populations, the effects of smoking, chronic alcoholism and poly-medication may combine to decrease the intestinal absorption of vitamin C.
An unbalanced diet is often the cause of vitamin C deficiency [15]. The prevalence of vitamin C deficiency is around 11% in the general population in France [16].
Vitamin C deficiency in persons with schizophrenia may contribute to poor oral health. The prevalence of vitamin C deficiency in schizophrenic persons should be evaluated.
International data confirm that oral health is poor in schizophrenic persons. Dental caries and periodontal measurement indexes are often twice the level found in the general population [5,17-20]. Data are available for inpatients (most marked by the disease). Today, 90% of schizophrenic persons are not hospitalized to monitor their condition and the available studies that include schizophrenic persons do not use random selection [21].
Thus, in order to implement public health programs, it is necessary to have objective data on the situation of persons followed as inpatients and outpatients. A good knowledge of the determinants of oral health in schizophrenic persons, and the social and environmental perceptions of oral health quality will better meet these populations' preventive care needs in the department of Cote d'Or.
AIMS:
The principal objective of this study is to evaluate oral health level of schizophrenic persons in outpatient and inpatient facilities in Cote d'Or (550 000 people), with a quantitative evaluation (dental caries index and oral hygiene index) and a qualitative evaluation on the participants' perceptions of their Oral Health Related Quality of Life (OHRQoL).
We hypothesize that the evaluation of oral health of randomly selected schizophrenic persons matched to the characteristics of the population of Cote d'Or with schizophrenia will provide representative data compared with prospective studies. In addition we will seek to identify associated variables (age, sex, smoking, comorbidity, treatment, the level of oral hygiene), the need for treatment and to evaluate vitamin C deficiency in patients with schizophrenia.
METHODS/DESIGN
Overview:
This is a multicentre cross-sectional study (Figure1). This study aims to recruit 120 persons with schizophrenia by random selection matched to the characteristics of the schizophrenic population of the Cote d'Or department during a six-month period. This study has been approved by the Committee for the Protection of Persons (CPP) number II of Eastern France (registration number: 2014-A00358-39). After providing participants with a complete description of the study, written informed consent will be obtained from each participant.
Inclusion Criteria
Persons eligible to be enrolled in this trial are: (1) Persons who have provided consent, (2) Persons of either sex over 18 years of age, (3) who meet the diagnosis of schizophrenia (Diagnosis: F20-F29) defined in the International Classification Disorders-ten edition (ICD 10), (4) and receiving care in hospital (in- or outpatient) in one of the hospitals taking part in the study [21].
Exclusion Criteria
Persons will be excluded if are, at the inclusion visit, in any of the following categories: (1) Persons not covered by national health insurance, (2) Pregnant or breast-feeding women, (3) Persons not stabilized from a psychiatric viewpoint, (4) Persons experiencing an acute psychiatric episode, (5) Cannot understand or have a poor understanding of French.
Study Process
The study will conducted three phases: (Figure1)
1) During the first phase, the persons will be included from out- or in-patients in three psychiatric hospitals. The active files of persons and background characteristics were extracted from the administrative databases of the three psychiatric hospitals: The hospital centre La Chartreuse, the hospital centre Robert Morlevat de Semur-en-Auxois and the University Hospital Centre (UHC) of Dijon. A random draw will be implemented to select persons to be informed of the study and the objectives of the research.
2) The second phase will consist of a dental examination to be evaluated and to check their eligibility to the study. 120 persons will have to be psychically stabile according to the inclusion and exclusion criteria and will have to sign an informant consent form.
3) Thirdly, clinical, biological and OHRQoL assessment will be performed.
The Random Draw and Data-Management
Random selection will be performed with SAS version 9.3 (SAS Institute Inc) by the team of statisticians of the Methodological Support Unit, Direction of Clinical Research, UHD, France. Persons screened for the studies will be identified using a random adjusted stratified sampling method depending of their age, sex or residential area (urban/rural area) according to the population characteristics of schizophrenic person in Cote d'Or. A person who refuses to participate in this study will be replaced by a person having the same characteristics.
All data of included person will be saved in an electronic Case Report Form (CRF), created with the software CleanWeb™. Real-time likelihood and coherency tests will be implemented to check data entry with predefined rules in collaboration with the investigator. Periodically, coherency reports will be sent to investigators in the aim of correcting all errors highlighted. The data-base will be frozen only when all the errors have been corrected and when no more are found.
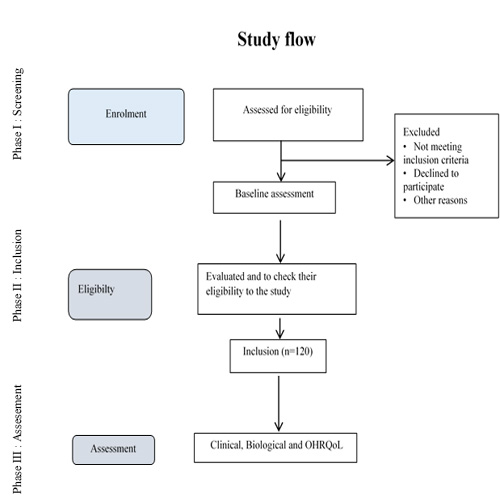
Figure. 1: Study flow diagram
Each participants will be ask to complete the Global Oral Heath Assessment Index (GOHAI) questionnaire and to respond to other questions relating to their socio-economic status (SES) (age, sex, level of education, residential area), health status (duration of mental illness), dental attendance and oral behaviours (smoking habits, tooth brushing frequency) [22]. Finally, persons will be questioned about their perceived satisfaction with their oral health.
The same day, each person will be underwent a clinical oral examination using portable dental equipment and blood sampling for assay of vitamin C. Pre-packaged and disposable instruments will be used. Caries experience will be assessed at the dentinal (D3) level using the DMFT index [23]. Dental plaque and calculus will be evaluated using the Simplified Oral Hygiene Index (OHI-S) [24].
The blood sample will be centrifuged in time and heparin plasma will be frozen at -20°C, away from light (tube wrapped in foil). The laboratory transport to University Hospital of Dijon (UHD) will be provided in a refrigerated container and protected from light. The assays will be carried out by the laboratory of UHD.
This investigation will require half an hour for each person who agrees to participate in the study.
Outcomes
Our primary end point will be carious experience (DMFT). Caries will be assessed at the dentinal (D3) level and the Decayed, Missing, or Filled Teeth (DMFT) index, based on 28 teeth, calculated as recommended by WHO (World Health Organization) [23].
The secondary end point will be the hygiene index. Dental plaque and calculus were evaluated on six teeth using the Simplified Oral Hygiene Index (OHI-S) [24].
The other secondary end point will include the OHRQoL from the GOHAI. The GOHAI is a self-assessment oral health index, which has been initially validated for use in elderly North Americans [22]. A French version has been validated in France in a sample of middle aged adults [25]. The questionnaire consists of 12 questions, phrased positively or negatively for the French version. The modalities of answer are based on a Likert scale with scores varying from 1 to 5 [26]. The GOHAI score is the sum of the answers to the 12 questions so that a high score (Maximum=60) means a satisfactory oral health.
Sample Size Calculation
The literature highlights a mean DMFT of 24.5±8.1 [27-30]. Assuming sample power so that the 95% confidence interval (CI) will be of 95% CI= [23-26], and taking in account a rate of missing data up to 10%, we will need to include 120 persons [27].
Statistical Analysis
Results for qualitative covariates were expressed as proportions. Quantitative variables were expressed as means ± standard deviation (SD) when normally distributed, but each person underwent a clinical oral as median and range. Comparison of persons' characteristics between a group of interest and the general population of schizophrenic person in Cote d'Or will be performed using Student's t-test, analysis of variance, Kruskal-Wallis non-parametric tests, Pearson's chisquare (chi2) or Fisher's Exact tests when appropriate. A value of p < 0.05 was considered statistically significant. All analyses will be performed using SAS version 9.3 (SAS Institute INC.).
DISCUSSION
The poor oral health of persons with schizophrenia and the resulting pathologies are rarely mentioned yet the data on the subject show that the oral health of these persons is poor and the consequences are major [5,28]. They impact physical health, in particular by exposing the persons to the risk of cardiovascular disease, and alter their quality of life, their well-being, and their social functioning [29]. Most of the selected studies were conducted among hospitalized persons. It is therefore difficult to have a clear idea of the oral health of in- or out-patients.
A major bias of our study could be the ability of schizophrenic persons to participate in a study focused on oral health. Persons who do not agree to participate in this kind of study may be less likely to agree to a dental examination because of their poor oral health. Selection bias may also exist in other published studies [19,30]. We can therefore assume that the published data only partially reflect the oral health status of these populations. Persons who do not agree to participate in these studies may so decide because of their poor oral health [31]. Moreover, most of the studies are conducted with hospitalized persons while most persons with schizophrenia are in outpatient care such studies report on oral health for just a portion of the population with schizophrenia [32].
Assessment of perception of OHRQoL of schizophrenics is studied here for the first time, including the prevalence of vitamin C deficiency .We aims to investigate the oral health of all the schizophrenics in Cote d'Or, not just those in hospital. To improve the oral health of schizophrenics involves identifying appropriate health promoting programmes for this population. This requires the acquisition of objective and representative quantitative and qualitative data.
Trial Status
Enrolment for this study began in September 2014. At the time of submission, we have enrolled 60 participants.
Competing Interests
The authors declare that they have no competing interests.
Authors' Contributions
FD, BT, GM, TW and JPC conceived and designed the study protocol, and wrote the manuscript. ASF, SM, LJ participated in the conception of the study, helped to draft the manuscript, and are responsible for the statistical analyses. MC and NA sought ethical approval, participated in the design and the coordination of the study, and carried out financial and all materiel needs.
CR and CA participated in the review of the literature, manuscript writing and the revision.
The authors are the coordinators of the clinical centres that will enrol the trial participants.
The corresponding author had final responsibility for the decision to submit for publication.
All authors read and approved the final version of the manuscript.
ACKNOWLEDGMENTS
The authors would like to thank Professor Paul Riordan for his help with English language correction, and are grateful to the Regional Health Agency of Bourgogne (Agence Regionale de Sante de Bourgogne) and the University Hospital of Dijon for the financial support given to the study.
REFERENCES
- Hafner H and an der Heiden W. (1997). Epidemiology of schizophrenia. Can J Psychiatry Rev Can Psychiatr. 42, 139-151.
- Jablensky A. (2000). Epidemiology of schizophrenia: the global burden of disease and disability. Eur Arch Psychiatry Clin Neurosci. 250(6), 274-285.
- Wildgust HJ, Hodgson R and Beary M. (2010). The paradox of premature mortality in schizophrenia: new research questions. J Psychopharmacol Oxf Engl. 24, 9-15.
- Denis F. (2014). The oral health of patients in psychiatric institutions and related comorbidities. Soins Psychiatr. 40-44.
- Wey MC, Loh S, Doss JG, Abu Bakar AK, et al. (2015). The oral health of people with chronic schizophrenia: A neglected public health burden. Aust NZJ Psychiatry. pii: 0004867415615947. [Epub ahead of print].
- Grisso T and Appelbaum PS. (1995). Comparison of standards for assessing patients' capacities to make treatment decisions. Am J Psychiatry. 152, 1033-1037.
- Casadebaig F and Quemada N. (1989). Mortality in psychiatric inpatients. Acta Psychiatr Scand. 79, 257-264.
- Saravane D, Feve B, Frances Y, Corruble E, et al. (2009). Drawing up guidelines for the attendance of physical health of patients with severe mental illness. L'Encephale. 35, 330-339.
- Citrome L and Yeomans D. (2005). Do guidelines for severe mental illness promote physical health and well-being? J Psychopharmacol Oxf Engl. 19, 102-109.
- Scannapieco FA and Genco RJ. (1999). Association of periodontal infections with atherosclerotic and pulmonary diseases. J Periodontal Res. 34, 340-345.
- Van der Velden U, Kuzmanova D and Chapple ILC. (2011). Micronutritional approaches to periodontal therapy. J Clin Periodontol. 38, 142-158.
- Franceschi RT, Iyer BS and Cui Y. (1994). Effects of ascorbic acid on collagen matrix formation and osteoblast differentiation in murine MC3T3-E1 cells. J Bone Miner Res. 9, 843-854.
- Ishikawa S, Iwasaki K, Komaki M, Ishikawa I, et al. (2004). Role of Ascorbic Acid in Periodontal Ligament Cell Differentiation. J Periodontol. 75(5), 709-716.
- Touyz LZ. (1984). Vitamin C, oral scurvy and periodontal disease. South Afr Med J Suid-Afr Tydskr Vir Geneeskd. 65, 838-842.
- Khonsari H, Grandiere-Perez L and Caumes E. (2005). Scurvy, a re-emerging disease. Rev Medecine Interne. 26(11), 885-890.
- Fain O. (2004). Carences en vitamine C. Rev Medecine Interne. 25, 872-880.
- Eltas A, Kartalci S, Eltas SD, Dundar S, et al. (2013). An assessment of periodontal health in patients with schizophrenia and taking antipsychotic medication. Int J Dent Hyg. 11(2), 78-83.
- Arnaiz A, Zumarraga M, Diez-Altuna I, Uriarte JJ, et al. (2011). Oral health and the symptoms of schizophrenia. Psychiatry Res. 188, 24-28.
- Thomas A, Lavrentzou E, Karouzos C, Kontis C, et al. (1996). Factors which influence the oral condition of chronic schizophrenia patients. Spec Care Dent Off Publ Am Assoc Hosp Dent Acad Dent Handicap Am Soc Geriatr Dent. 16(2), 84-86.
- Tani H, Uchida H, Suzuki T, Shibuya Y, et al. (2012). Dental conditions in inpatients with schizophrenia: a large-scale multi-site survey. BMC Oral Health. 12, 32.
- OMS Classification CIM-10 des troubles mentaux et des troubles du comportement [Internet]. WHO. [cited 2015 Oct 11]. Available from : http://www.who.int.com
- Atchison KA and Dolan TA. (1990). Development of the Geriatric Oral Health Assessment Index. J Dent Educ. 54, 680-687.
- Caries Process and Prevention Strategies: Epidemiology Continuing Education Course.
- Oral Hygiene Index (Greene and Vermilion, 1960) [Internet]. (2010).
- Tubert-Jeannin S, Riordan PJ, Morel-Papernot A, Porcheray S, et al. (2003). Validation of an oral health quality of life index (GOHAI) in France. Community Dent Oral Epidemiol. 31, 275-284.
- Cohen LK and Jago JD. (1976). Towards the formulation of sociodental indicators. Int J Health Serv Plan Adm Eval. 6(4), 681-698.
- Schwartz D. [Methodes statistiques a l'usage des medecins biologistes]. Population.1964; 19, 1004.
- Kisely S, Sawyer E, Robinson G, Siskind D, et al. (2015). A systematic review and meta-analysis of the effect of depot antipsychotic frequency on compliance and outcome. Schizophr Res. 166, 178-186.
- Moore S, Shiers D, Daly B, Mitchell AJ, et al. (2015). Promoting physical health for people with schizophrenia by reducing disparities in medical and dental care. Acta Psychiatr Scand. 132, 109-121.
- Nielsen J, Munk-Jorgensen P, Skadhede S, Correll CU, et al. (2011). Determinants of poor dental care in patients with schizophrenia: a historical, prospective database study. J Clin Psychiatry. 72, 140-143.
- Bertaud-Gounot V, Kovess-Masfety V, Perrus C, Trohel G, et al. (2013). Oral health status and treatment needs among psychiatric inpatients in Rennes, France: a cross-sectional study. BMC Psychiatry. 13, 227.
- Levolution des dispostif de soins psychitriques en Allemagne, Angleterre, France et Italie: similitudes et divergences-Qes180.pdf.