Previous Issues Volume 1, Issue 1 - 2018
Ethical Challenges in Intellectual Disability Research
Owen Doody
Department of Nursing and Midwifery, North Bank Campus, University of Limerick, Ireland.
Corresponding Author: Owen Doody, Department of Nursing and Midwifery, North Bank Campus, University of Limerick, Ireland, Tel: +353 61 213367; E-Mail: [email protected]
Received Date: 11 Aug 2018 Accepted Date: 21 Aug 2018 Published Date: 27 Aug 2018
Copyright © 2018 Doody O
Citation: Doody O. (2018). Ethical Challenges in Intellectual Disability Research. Mathews J Nurs. 1(1): 005.
ABSTRACT
Involving individuals with intellectual disability in research can be difficult, researchers often focus on those with a mild/ moderate disability as they are often more accessible. However, there is a drive politically and socially to include and involve all persons with intellectual disability in research. Researchers must address the notions of consent, autonomy and consider best practice rather than a threshold of autonomy to avoid wronging participants and enabling persons with intellectual disability to be involved in research to the best of their ability. Thereby enabling all people with intellectual disability including those least able to participate in research through using creative and imaginative ways to support them through the research process.
Keywords: Ethics; Inclusion; Intellectual disability; Participation; Research.
INTRODUCTION
There has been great strives over the years for individuals with intellectual disability to live in their own community, or move towards least restrictive environments to support inclusion. However, this has resulted in an inconsistent emancipation for individuals with intellectual disability within healthcare and research. This inconsistency is evident in the increased health disparities among individuals with intellectual disability [1, 2] and the fact most research has relied on a proxy voice, with the voice of individuals with intellectual disability less evident [3]. Movement towards self-advocacy promises to empower individuals with intellectual disability to challenge these inequities, particularly around health and wellness goals [3-5]. However, accomplishing these goals requires engagement with individuals with intellectual disability in research, not only for the benefit of findings and outcomes, but also for the emancipatory value of hearing their voice [6]. In so doing, health care professionals, family carers and researchers can be informed of ways to improve health and well-being of individuals with intellectual disability through an increased understanding, knowledge and awareness.
Involving individuals with intellectual disability in research is essential, as health is considered beyond that of a dominant bio-medical cultural paradigm, which adopts freedom from disease and disability as the ideal. This presents a theoretical challenge in contextualising health and wellness as there is an absence of consistent and authentic voices of individuals with intellectual disability. Failing to engage people with intellectual disability in research and using proxy voice assumes that understanding of perceptions, meanings, and indeed the construct of reality are within the range of experience and thought of the proxy. Embedded in this approach, is that knowledge of best practices for personal health and wellness is a nexus situated within the sole possession of proxy that can be shared on behalf of the individual with intellectual disability [6]. Moving beyond proxy voice places the person with intellectual disability in a position of power by enhancing their knowledge and understanding of the world and their place in it, and valuing them as expert witnesses [7]. This article presents ethical aspects of consent, inclusion, and review and access of people with intellectual disability in research.
INTELLECTUAL DISABILITY RESEARCH AND ETHICS
The earliest research ethics code was Prussian, which developed because of dangerous research conducted by doctors on human subjects at the end of the 19th Century [8]. However, during the World War II the Nazi performed horrific experiments in the concentration camps resulting in the Nuremberg trials and development of the Nuremberg Code [9] with its primary function of protecting human subjects. Protection would be maintained through voluntary consent, freedom from coercion and appropriate risk benefit ratio [10]. However, vulnerability and benefit remained an issue for concern as individuals may consent to research if they are vulnerable or do not understand what is happening, or individuals who may benefit may never be able to consent; for example, babies [10]. In response to these concerns the Declaration of Helsinki [11,12] was developed allowing research to be conducted with those who may not have the capacity to consent provided the criteria of; been reviewed by an independent committee, informed rather than voluntary consent were met and the notion of legal guardians was addressed. Building on these codes The Belmont Report [13] introduced the three rights of; respect for autonomy, beneficence and justice. In addition, to protect these three rights the Belmont Report identified the three practices of; informed consent, risk-benefit assessment and fair-selection process.
In the field of intellectual disability, the population has often been seen as 'vulnerable' and this may be due to the long history of institutional care that was often located away from public scrutiny, with an underlying notion that individuals with intellectual disability were to be looked after and cared for. However, the development of the principle of normalisation [14, 15] and its application to service provision saw individuals with intellectual disability gradually becoming visible in society and research. The emphasis on protection of individuals often resulted in exclusion of individual with intellectual disability as a means for ethics committees and researchers to protect individuals perceived as vulnerable [16, 17]. This perceived vulnerability and/or overestimation of vulnerability has often led to the exclusion of people with intellectual disability in research [18, 19]. Due to the concerns regarding vulnerability, where research with people with intellectual disability has occurred it has tended to focus on those with mild to moderate intellectual disability leading to an under representation of a large proportion of the intellectual disability population [4]. This under representation particularly of those with severe to profound level of intellectual disability may be in part due to exclusion and in part due to the hesitancy of ethics committees to grant approval for the intellectual disability population grouping. To engage individuals with intellectual disability in research, ethical approval is required which places an emphasis on research protection and incorporating consent. In response to this issue, the aspect of inclusion in research has arisen for individuals with intellectual disability, facilitated by social model thinking [20]. Early commentators such as Oliver [21] and Zarb [22] argued for an emancipatory model, framing research as an activity decided by intellectual disabled people rather than by professional researchers. Thereby, creating three aspects of research ethics: consent, inclusion, and review and access all of which work for and against the interest of some individuals with intellectual disability.
CONSENT
Gaining informed consent from persons with intellectual disabilities can be challenging, as there is nothing ordinary about informed consent, either conceptually or procedurally for people who have intellectual disability [23]. Valid consent 'requires a person to appreciate the current situation, possess sufficient information, understand the information given, be able to weigh up the pros and cons, communicate a choice voluntarily and free from coercion' (p.58) [24]. Thereby obtaining consent from participants with intellectual disability presents particular ethical challenges for researchers [25]. Difficulties with attention, memory and ability to transfer recently learned material creates tension between, ensuring people with intellectual disability understand the purpose and implications of their participation in research and at the same time avoiding any coercion [25]. Iacono and Murray (p.49) [26] further emphasis the difficulty and tension that exists when stating 'there is a need to protect potential vulnerable participant groups, while ensuring that demands placed on researchers are not so restrictive as to preclude valuable research'. Thereby there is a concern that to overcome these difficulties researchers may exclude people with an intellectual disability from research or include them without their consent. Generally, consent can be unpacked to reveal three issues for research undertaken in this area; the capacity of the participants to give consent, the value of consent as an indicator for participation, and the discrepancy between expert and lay understandings of what consent actually entails.
To determine the capacity of an individual to freely provide consent, one should focus on a person's ability to engage in everyday decision-making. Consideration must also be given to those areas of functioning where individuals retain competency and the ability to consent should not be presumed [23]. When conducting a study, the researcher should remain focused on other indicators of the clients general well-being, including facial expressions to assist in identifying their capacity to consent [27]. In addition, at various points during data collection the researcher should stop to reconfirm the participants wish to continue, as their initial agreement to participate is insufficient [28] and to acknowledge that consent is not a one-off event [27, 29]. Having family member or staff members well known to participants present during data collection, acting as third parties or validator is important for identifying signs of discomfort or stress should they transpire [27, 29]. Participant should have the capacity to provide consent of their own volition and without coercion [30] and it must be recognised that both the participant and the family or staff member must give consent to participate [31]. However, difficulty arises in reaching a balance between ensuring that people with intellectual disability understand the purpose and consequences of their participation in research and ensuring at the same time they are not coerced to participate [25, 32]. Often proxy consent from a next of kin/family member or a care worker working closely with the person with intellectual disability is used [33, 34].
Jenkinson [35] identify factors that affect an individual's decision making such as; who has control over decisions and the organisational structures that exist in the individual's environment. Others may relate to the researcher's attitude to consent and the significance of ensuring that participation in research is an ongoing practise and not just something that is ascertained at the onset of contact. The greater control the individual with intellectual disability has in each decision point within the research process the less probable it would be that the research infringes on the rights of people with intellectual disability [36]. Thereby careful planning by the researcher on issues such as; access to participants, consent by participants, content and appropriateness of information (written and verbal), nature and duration of data collection, support required by participants, accessibility and transport arrangements need to be considered [37]. The researcher should clearly identify him/herself, establish a good rapport with the participant, use incidental conversation to break the ice before embarking on the data collection proper, thereby encouraging the participant to trust and share accurate information on the topic to be discussed [38]. The researcher should explain the purpose of the research, address and explain terms such as; consent, confidentiality and that there are no right or wrong answers.
What must be considered is that people with intellectual disability are a heterogeneous population and within this population many sub-groups exists [39]. Some individuals with intellectual disability will have few problems understanding the nature of a research project and the implications of their involvement. They will be able to make a decision about their participation and provide or withhold their consent. However, people with the higher degrees of disability and whose disability and associated needs require the highest levels of continual support and care challenge our understanding of how best to support their participation in research. This group are also least equipped to understand their own situation and being able to articulate their sense of self. However, participation should reflect the importance of capacity rather than lack of capacity and should be engaging rather than preventive in nature, thus safeguarding that it complies with relevant constitutional and human rights standards. Finding that a person lacks capacity leads to the restriction or removal of fundamental rights and in this sense, the issues of capacity and rights are intricately interrelated. Thereby, consent should be evaluated from the point of view of research participants, and the possible stress or harm caused to them. This wider more holistic approach to informed consent entails a greater focus on the wellbeing of research participants as the major concern during research and researchers need to plan their practice accordingly and continually evaluate participants' wellbeing [6].
INCLUSION
It was not until the 1980s that people with intellectual disability were involved even as interviewees in research that was about them, or their views sought in evaluations of the services they received [40]. Policy requirements promoting "client involvement" led to a range of clients, including people with mild and moderate intellectual disability participating in health and social care service planning and research [41, 42]. Most people with intellectual disability now live in community settings but are among the most disadvantaged in our society [43, 44]. In addition, the perceptions and viewpoints of people with intellectual disability who lack capacity (and indeed others with cognitive impairments) may therefore be "missing" from research and this in itself is an ethical issue [45]. The benefits of carrying out research with persons with intellectual disability includes; helping others to better understand their reality [30], gain insight into the experiential nature of quality of life [46], understanding the embodied experience of intellectual disability [47], getting the perspectives of those underrepresented in public policy [48], and discovering positive experiences of care [49].
The movement towards inclusion in research developed in parallel with academic discourse and culminated with the publication of Nothing About Us Without Us [50] and unified professionals, academics, clinicians and individuals who valued sharing research agendas. Inclusive research encompasses two methodological approaches, participative research and emancipatory research [51, 52]. Participative research enables alliances or partnerships to develop between the researcher and the participants used to differentiate between situations where people with disability participate, but have no control of the research process. Where as emancipatory research enables people with intellectual disability control the whole research process thus leading to empowerment, social change and the emancipation of people with disabilities [37, 40]. The participatory model, to date has been more commonly used promoting partnership working by professionals and clients, while the aim of the emancipatory approach is for clients to have control by been involved in all decisions throughout the process [37].
Walmsley [53] distinguishes between participative and emancipatory approaches, suggesting that participative approaches are concerned with the experiences of people with intellectual disabilities, and are influenced by normalisation theory, phenomenological approaches or the social model of disability. In participatory approaches, researchers work in conjunction with the participants, while employing qualitative methods with the aim of interpreting and explaining the experiences of people with intellectual disability. In contrast, emancipatory approaches are based on the social model of disability and can utilise either qualitative or quantitative methods in the research process where the researchers expertise is available for people with disability. Emancipatory research is dedicated to changing the conditions of the relationship between the researcher and the researched [54]. This approach highlights a shift from doing research on and about populations, to conducting research with populations and involving relevant service-users, carers or their representative groups in the design, conduct, analysis and reporting of research [55]. Through such processes, researchers can be better informed on how to frame their research questions, test the validity and acceptability of the research methodology, and assist in interpretation of the findings. In these ways, inclusive approaches enhance the efficacy of research and in today's research environment many funding agencies require an inclusive approach. In addition, the United Nations (UN) Convention on Rights for Persons with Disabilities challenges researchers to find ways to include people with intellectual disability in the development of research about them and to collect data and statistics which can inform policy and practice [56].
Including people with intellectual disabilities in research about their lives is widely endorsed [57] and progress is evident with the promotion of inclusive research [58, 59]. To support the inclusion of people with intellectual disability in research a variety of approaches and forms of involvement have arisen [60- 62]. Utilisation of supports are evident across the research literature such as; McCleery [63] high-technology devices and the participants used to differentiate between situations where people with disability participate, but have no control of the research process. Where as emancipatory research enables people with intellectual disability control the whole research process thus leading to empowerment, social change and the emancipation of people with disabilities [37, 40]. The participatory model, to date has been more commonly used promoting partnership working by professionals and clients, while the aim of the emancipatory approach is for clients to have control by been involved in all decisions throughout the process [37]. Walmsley [53] distinguishes between participative and emancipatory approaches, suggesting that participative approaches are concerned with the experiences of people with intellectual disabilities, and are influenced by normalisation theory, phenomenological approaches or the social model of disability. In participatory approaches, researchers work in conjunction with the participants, while employing qualitative methods with the aim of interpreting and explaining the experiences of people with intellectual disability. In contrast, emancipatory approaches are based on the social model of disability and can utilise either qualitative or quantitative methods in the research process where the researchers expertise is available for people with disability. Emancipatory research is dedicated to changing the conditions of the relationship between the researcher and the researched [54]. This approach highlights a shift from doing research on and about populations, to conducting research with populations and involving relevant service-users, carers or their representative groups in the design, conduct, analysis and reporting of research [55]. Through such processes, researchers can be better informed on how to frame their research questions, test the validity and acceptability of the research methodology, and assist in interpretation of the findings. In these ways, inclusive approaches enhance the efficacy of research and in today's research environment many funding agencies require an inclusive approach. In addition, the United Nations (UN) Convention on Rights for Persons with Disabilities challenges researchers to find ways to include people with intellectual disability in the development of research about them and to collect data and statistics which can inform policy and practice [56]. Including people with intellectual disabilities in research about their lives is widely endorsed [57] and progress is evident with the promotion of inclusive research [58, 59]. To support the inclusion of people with intellectual disability in research a variety of approaches and forms of involvement have arisen [60- 62]. Utilisation of supports are evident across the research literature such as; McCleery [63] high-technology devices and supports, Manning [64] story-telling, Cannella-Malone et al.,[65] video-recording, Darewych et al., [66] art medium and Akkerman et al.,[67] photovoice. In addition, people with intellectual disability have been involved in; acting as an adviser [68], data collection and analysis [69, 70], provision of research education and training [57,71,72], dissemination of research findings [73], identification of research questions [74], being a member of an ethics committee [75] and being involved at each step of the research process [69,70,76]. Thus the opportunity to take part in research is increasing for many people with intellectual disability [58, 77].
REVIEW AND ACCESS
The structure and knowledge available to enable the ethical review and approval of proposed research projects varies from country to country. Therefore, it is imperative to draw upon a number of internationally accepted principles to guide the development, ethical review and implementation of research. Consequently, the IASSID have drawn up a statement developed with reference to a number of internationally accepted documents, including: Nuremberg Code [9], Universal Declaration of Human Rights [78], Declaration of Helsinki [11, 12], International Ethical Guidelines for Biomedical Research Involving Humans [79, 80] and the European Union Directive on the Conduct of Clinical Trials [81]. Prior to research proceeding rigorous ethical safeguards must be in place to promote and protect the health, safety and human rights of participants; and to prevent their exploitation. The ethics process involves the researcher explaining to an independent and competent authority what they aim to do; why such an inquiry is important; possible benefits to society; dangers involved; how they intend to proceed; safeguards to protect the participants' rights and safety; and how they will make their findings available. Ethics committee/institutional review board normally consist of men and women, who provide expertise in research processes from different disciplines, as well as lay persons from the general community, and wherever possible people with intellectual disability. In the case of institutional-based ethics committees, there will usually be at least one person who is independent of the institution or the organisation from which the ethics application originates. Ideally, there should be at least one committee member who can represent and advocate for the interests of those persons identified as potential participants for the study. Such representation or advocacy is particularly important where the proposed research involves participants who could be considered vulnerable or disadvantaged in some way or from a cultural background different from that of those proposing the research.
An ethics committee/institutional review board, or equivalent local committee, has the authority to approve, propose modifications or reject an ethics application. Such committees also have a right to request regular progress reports regarding any research activities they have approved and the authority to withdraw approval for research that fails to comply with an agreed protocol or local regulations. When evaluating the ethical merit of a proposed research project, and conducting research involving people with intellectual disability as participants or research that is intended to affect their lives. The three fundamental ethical principles [80] should apply; respect for persons, including their autonomy and right to selfdetermination, and beneficence for participants and the community. Thereby maximizing benefits and minimising risks, and justice, both legally and morally for those involved in research and the communities to which the participants belong.
There is a need for ethics committees to move away from protectionism and acknowledge the empowering potential of inclusive research [82]. To do this it may be helpful to differentiate between procedural ethics (what happens in research design and in research ethics committees) and ethics in practice (what happens in the interactions between researcher and participants and in the way data is interpreted, communicated and used). Ethics in practice is enhanced by procedural ethics and the underlying values are the same [83]. Dalton and McVilly [84] offer a guide for ethics in practice when conducting research with people with intellectual disability (see table 1).
Table 1: Ethics in practice guide [84].
|
|
|
|
|
|
|
|
Gaining access to participants almost always involves going through gatekeepers or facilitators and a hierarchy of gatekeepers [18, 85] or tiers of management [86, 87] can exist. Using gatekeepers usually involves the additional stage of providing the gatekeeper with information about the study and asking them to suggest or contact potential participants. This requires building rapport and trust with the gatekeeper before doing so with potential/actual participants. For gatekeepers to assist, they will need to be convinced of the benefits for the people they often regard as in need of their protection. It is acknowledged that while there is, a need to include individuals with intellectual disability in research there remains a potentially negative outcome (exclusion) for the least able through the over-protection and gatekeeping roles taken by service providers. Gatekeepers are faced with a difficult decision of trying to decide to grant access and may actually block access [49, 88] rendering the person with intellectual disability silent [38] and this protective power can be seen as oppressive [89]. This difficult position placed upon gatekeepers may be alleviated by them having access to the ethics committees review comments and letter of approval to support their decision making and abate their concerns.
Having to negotiate access to the client group's reveals the importance of gatekeepers when it comes to conducting research with people with intellectual disability [90]. The directors of the agency, acts as initial gatekeeper, granting access to their facilities to conduct the study. The second layer of gatekeepers are staff members on whom researchers rely, to approach care recipients and inquire if they are interested in being involved, and to ensure that potential participants understands the researchers explanation of why the researcher wishes to involve them, what the research will involve and that they could withdraw at any point during the process. Gatekeepers may also facilitate access and have a significant role in carefully explaining to participants how research is different from intervention with different purposes and timelines [91]. Moreover, staff are often required to remain with clients during data collection and are often too busy and tired or too suspicious of the research to want to become involved [87, 92]. Although staff members do not have the power to deny permission because the director would already have granted authority, they have 'power to block access' (p.8) to clients [93]. The power of gatekeepers can also be explicit in their ability to make determinations about which clients may be more eligible to participate in the research than others [49, 94]. In addition, self-advocacy organisations supporting people with intellectual disability can become overwhelmed by the increasing volume of opportunities to participate in research and reject approaches from some researchers.
CONCLUSION
Research is conducted to expand knowledge, discover the truth and provide evidence for practitioners, policy-makers and legislators. Research involving people with intellectual disability is important to; uncover relevant issues, inform policy, evaluate programmes and services, and identifying the affects of social and economic change. The importance of research and data related to intellectual disability is recognised in the Convention on the Rights of Persons with Disability [56]. The problem for researchers is whether to follow closely the inclusion and consent requirements for research in intellectual disability at the cost of excluding those unable to meet those requirements. If we do this, the research evidence will not be reflective of the needs of the intellectual disability population. We need to try different methods of communication with different groups so as inclusion and consent do not threaten exclusion of those unable to give an autonomous or ideal consent. While there is a need to protect vulnerable participant groups, researchers also must ensure they are not placing restrictions to preclude valuable research and exclusion of people with intellectual disability [26] or including them without their consent [95]. This article identifies ethical challenges and possible action for the inclusion of people with intellectual disability in research (Figure 1).
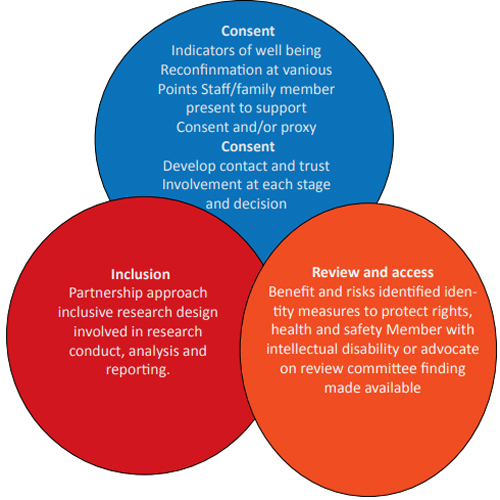
Figure 1: Ethical challenges and possible action for the inclusion of people with intellectual disability in research.
The omission of people with intellectual disability results in skewed sampling and the decision to include people with intellectual disability is influenced by those who have control over decisions and the organisational structures that exist in the individual's environment [35]. Others relate to the researcher's attitude to consent and the necessity to ensure that participation in research is an ongoing process and is not something established only at the beginning of contact. Researchers need to adopt a research approach that involves people with intellectual disability at each stage of the research process, including the development of research agendas, commissioning, overseeing, conducting and evaluating research as well as supporting the use of the emerging evidence base in policy and practice. The influences of normalisation theory and the social model of disability have been key influencers in changing the research environment for people with intellectual disability [53]. However, a number of challenges exist regarding the inclusion of people with intellectual disability been included in mainstream research affecting their lives [96]. The challenges include; attitudes of professionals, diversity and complexity of lay groups, knowledge, power relationships, resources (both personal and financial), and values [97].
One way in which ethics committees and researchers have protected people perceived as vulnerable is by excluding them from research [32]. However, people with intellectual disability should not be excluded (discriminated against) as potential participants in research and every effort should be made to include their perspectives, priorities and needs in research activities. Tuffrey-Wijne et al., [88] argues that it is unethical to exclude people with more severe intellectual disability from studies that could provide insight into their experiences and help to shape sensitive care in the future. A positive development with many funding bodies is that they now insist on the participation of people with intellectual disability as a condition of research funding [53, 97].
REFERENCES
- McCarron M, Swinburne J, Burke E, McGlinchey E, et al. (2013). Patterns of multimorbidity in an older population of persons with an intellectual disability: Results from the intellectual disability supplement to the Irish longitudinal study on again (IDS-TILDA). Research in Developmental Disabilities. 34(1): 521-527.
- Morin D, Merineau-Cote J, Ouellette-Kuntz H, Tasse M, et al. (2012). A comparison of the prevalence of chronic disease among individuals with and without intellectual disability. American Journal on Intellectual and Developmental Disabilities. 117(6): 455-463.
- Fujiura GT, Andersen E, Cardinal BJ, Drum CE, et al. (2012). Self-reported health of people with intellectual disability. Intellectual and Developmental Disabilities. 50(4): 352- 369.
- Feldman MA, Owen F, Andrews A, Hamelin J, et al. (2013). Health selfadvocacy training for persons with intellectual disabilities. Journal of Intellectual Disability Research. 56(11): 1110-1121.
- Brolan CE, Boyle FM, Dean JH, Taylor Gomez M, et al. (2012). Health advocacy: A vital step in attaining human rights for adults with intellectual disability. Journal of Intellectual Disability Research. 56(11): 1087-1097.
- Mietola R, Miettinen S and Vehmas S. (2017). Voiceless subjects: Research ethics and persons with profound intellectual disabilities. International Journal of Social Research Methodology. 20(3): 263-274.
- Atkinson D. (2004). Research and empowerment: involving people with learning difficulties in oral and life history research. Disability and Society. 19(7): 691-702.
- Vollmann J and Winau R. (1996). Informed consent in human experimentation before the Nuremberg code. British Medical Journal. 313(7070): 1445-1447.
- Nuremberg Code. (1947). Trials of war criminals before the Nuremberg Military Tribunals under Control Council Law No. 10 Vol. 2. Washington, DC: US Government Printing Office. 181-182.
- Doody O and Noonan M. (2016). Nursing research ethics, guidance and application in practice. British Journal of Nursing. 25(14): 803-807.
- World Medical Association. (1964). The Helsinki Declaration: Ethical principles for medical research involving human subjects. Helsinki, Finland: 18th World Medical Association General Assembly.
- World Medical Association. (2013). The Helsinki Declaration: Ethical principles for medical research involving human subjects. Fortaleza, Brazil: 64th World Medical Association General Assembly.
- United States Department Health, Education and Welfare. (1979). Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research, National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. Washington: United States Department Health, Education and Welfare Publication No. (OS) 78-0014.
- Nirje B. (1969). The normalization principle and its human management implications. In: Kugel, R. and Wolfensberger, W. Changing patterns in residential services for the mentally retarded. Washington DC: President's Committee on Mental Retardation. 1(2): 179-195.
- Wolfensberger W. (1972). The principle of normalization in human services. Toronto: National Institute on Mental Retardation.
- McDonald KE. (2012). 'We want respect': Adults with intellectual and developmental disabilities address respect in research. American Journal on Intellectual and Developmental Disabilities. 117(4): 263-274.
- Cleaver S, Ouellette-Kuntz H and Sakar A. (2010). Participation in intellectual disability research: A review of 20 years of studies. Journal of Intellectual Disability Research. 54(3): 187-193.
- Goldsmith L and Skirton H. (2015). Research involving people with a learning disability: Methodological challenges and ethical considerations. Journal of Research in Nursing. 20: 435-446.
- Jepson M. (2015). Applying the Mental Capacity Act to research with people with learning disabilities. British Journal of Learning Disabilities. 43(2): 128-134.
- Barnes C. and Mercer G. (2010). Exploring Disability. 2nd Edition, Cambridge: Polity Press.
- Oliver M. (1992). Changing the social relations of research production. Disability and Society. 7: 101-114.
- Zarb G. (1992). On the road to Damascus: first steps towards changing the relations of disability research production. Disability and Society. 7: 125-138.
- Thompson SA. (2002). My research friend, My friend the researcher, My friend, my researcher, Mis/Informed consent and people with developmental disabilities. In: van den Hoonaard, W.C. Walking the tightrope: Ethical issues for qualitative researchers. Toronto, Canada: University of Toronto Press. pp. 95-106.
- Dean E, Turner S, Cash J and Winterbottom P. (1998). Assessing the capacity to give consent. Nursing Times. 94: 58-59.
- Cameron L and Murphy J. (2006). Obtaining consent to participate in research: the issues involved in including people with a range of learning and communication disabilities. British Journal of Learning Disabilities. 35: 113- 120.
- Iacono T and Murray V. (2003). Issues of informed consent in conducting medical research involving people with intellectual disabilities. Journal of Applied Research Intellectual Disability. 16: 41-52.
- Dewing J. (2007). Participatory research: A method for process consent with persons who have dementia. Dementia. 6: 11-25.
- Sigelman C, Budd E, Spenhel and Schoenrock C. (1981). When in doubt, say yes: Acquiescence in interviews with mentally retarded persons. Mental Retardation. 19(2): 53-58.
- Lloyd V, Gatherer A and Kalsy S. (2006). Conducting qualitative interview research with people with expressive language difficulties. Qualitative Health Research. 16(10): 1386-1404.
- Holmes D, Kennedy S and Perron A. (2004). The mentally ill and social exclusion: A critical examination of the use of seclusion from the patient's perspective. Issues in Mental Health Nursing. 25(6): 559-578.
- Oliver-Africano P, Ahmed Z, Bouras N, Cooray S, et al. (2009). Overcoming the barriers experienced in conducting a medication trial in adults with aggressive challenging behaviour and intellectual disabilities. Journal of Intellectual Disability Research. 54(1): 17-25.
- Nicholson L, Colyer M and Cooper SA. (2013). Recruitment to intellectual disability research: a qualitative study. Journal of Intellectual Disability Research. 57(7): 647-656.
- Clement T and Bigby C. (2013). Ethical challenges in researching in group homes for people with severe learning disabilities: shifting the balance of power. Disability and Society. 28(4): 486-499.
- Nind M. (2008). Conducting qualitative research with people with learning, communication and other disabilities: Methodological challenges. National Centre for Research Method, NCRM/012.
- Jenkinson J. (1993). Who shall decide: The relevance of theory and research to decision making by people with and intellectual disability. Disability and Society. 8(3): 361-375.
- Swain J, Heyman B and Gillman M. (1998). Public research, private concerns: ethical issues in the use of open-ended interviews with people who have learning difficulties. Disability and Society. 13(1): 21-36.
- Walmsley J. (2004). Involving users with learning difficulties in health improvement: lessons from inclusive learning disability research. Nursing Inquiry. 11(1): 54-64.
- Witham G, Beddow A and Haigh C. (2015). Reflections on access: too vulnerable to research. Journal of Research in Nursing. 20: 28-37.
- Lewis A and Porter J. (2004). Interviewing children and young people with learning disabilities: guidelines for researchers and multi-professional practice. British Journal of Learning Disabilities. 32(4): 191-197.
- Kiernan C. (1999). Participation in research by people with learning disability: origins and issues. British Journal of Learning Disabilities. 27(2): 43-47.
- Boxall K, Carson I and Docherty D. (2004). Room at the academy: People with learning difficulties and higher education. Disability and Society. 19(2) 99-112.
- Boxall K, Warren L and Chau R. (2007). User Involvement. In: Hodgson, S. and Irving, Z. Policy reconsidered: Meanings, politics and practices. Bristol: The Policy Press. 155- 172.
- Emerson E, Malam S, Davies I and Spencer K. (2005). Adults with learning difficulties in England 2003/4. Leeds: Health and Social Care Information Centre.
- Emerson E, Vick B, Rechel B, Munoz-Baell I, et al. (2012). Health inequalities and people with disabilities in Europe, social exclusion, vulnerability and disadvantage task group background paper 5. Copenhagen: European Regional Office of the World Health Organization.
- Boxall K and Ralph S. (2009). Research ethics and the use of visual images in research with people with intellectual disability. Journal of Intellectual and Developmental Disability. 34(1): 45-54.
- Marquis R and Jackson R. (2000). Quality of life and quality of service relationships: Experiences of people with disabilities. Disability and Society. 15(3): 411-425.
- Pothier D and Devlin R. (2006). Introduction: Toward a critical theory of dis-citizenship. In: Pothier D. and Devlin, R. Critical disability theory: Essays in philosophy, politics, policy, and law. Vancouver, Canada: University of British Columbia Press. 1-24.
- Racino JA. (1999). Policy, program evaluation, and research in disability: Community support for all. New York: Haworth.
- Morrisey B. (2012). Ethics and research among persons with disabilities in long-term care. Qualitative Health Research. 22: 1284-97.
- Charlton J. (2000). Nothing about us without us: Disability oppression and empowerment. Berkley, CA: University of California Press.
- Walmsley J and Johnson K. (2003). Inclusive research with people with intellectual disabilities: Past, present and futures. London: Jessica Kingsley Publishing.
- Chappell A. (2000). Emergence of participatory methodology in learning difficulty research: Understanding the context. British Journal of Learning Disabilities. 28(1): 38- 43.
- Walmsley J. (2001). Normalisation, emancipatory research and inclusive research in learning disability. Disability and Society. 16(2): 187-205.
- Oliver M. (1997). Emancipatory research: Realistic goal or impossible dream. In: Barnes, C. and Mercer, G. Doing disability research. Leeds: The Disability Press. 15-31.
- Department of Health. (2005). Research governance framework for health and social care. 2nd Edition. Stationary Office, London: Department of Health.
- United Nations. (2006). General assembly: Convention on the rights of persons with disabilities, Optional protocol to the Convention. New York: United Nations.
- Carey E, Salmon N and Higgins A. (2014) Research active programme: Views of service users. Learning Disability Practice. 17: 22-28.
- Bane G, Deely M, Donohoe B, Dooher M, et al. (2012). Relationships of people with learning disabilities in Ireland. British Journal of Learning Disabilities. 40(2): 109-122.
- Johnson K. (2009). No longer researching about us without us: A researcher's reflection on rights and inclusive research in Ireland. British Journal of Learning Disabilities. 37(2): 250-256.
- Bigby C, Frawley P and Ramcharan P. (2014). Conceptualizing inclusive research with people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities. 27(1): 3-12.
- Garcia-Iriarte E, O'Brien P, McConkey R, Wolfe M. et al. (2014). Identifying the key concerns of Irish persons with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities. 27(6): 564-575.
- O'Brien P, McConkey R and Garcia-Iriarte E. (2014). Coresearching with people who have intellectual disabilities: Insights from a national survey. Journal of Applied Research in Intellectual Disabilities. 27(1): 65-75.
- McCleery JP. (2015). Comment on technology-based intervention research for individuals on the autism spectrum. Journal of Autism Developmental Disorder. 45(12): 3832-3835.
- Manning C. (2009). 'My Memory's Back!' inclusive learning disability research using ethics, oral history and digital storytelling. British Journal of Learning Disabilities. 38(3): 160-167.
- Cannella-Malone, Helen I, Brooks, David G, et al. (2013). Using self-directed video prompting to teach students with intellectual disabilities. Journal of Behavioural Education. 22(3): 169-189.
- Darewych OH, Carlton NR and Wayne K. (2015). Digital technology use in art therapy with adults with developmental disabilities. Journal on Developmental Disabilities 21(2): 95-102.
- Akkerman A, Janssen CG, Kef S and Meininger H P. (2014). Perspectives of employees with intellectual disabilities on themes relevant to their job satisfaction an explorative study using photovoice. Journal of Applied Research in Intellectual Disabilities. 27(6): 542-554.
- Nind M and Vinha H. (2012). Doing research inclusively: Bridges to multiple possibilities in inclusive research. British Journal of Learning Disabilities. 42(2): 102-109.
- Kramer J, Kramer JC, Garcia-Iriarte E and Hammel J. (2011). Following through to the end: The use of inclusive strategies to analyse and interpret data in participatory action research with individuals with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities. 24(3): 263-273.
- Bigby C and Frawley P. (2010). Reflections on doing inclusive research in the 'making life good in the community' study. Journal of Intellectual and Developmental Disability. 35(2): 53-61.
- Salmon N and Carey E. (2013). Research active programme: An inclusive research module in 3rd level education. British Journal of Learning Disabilities. 41(3): 244.
- Salmon N, Carey E and Hunt A. (2014). Research skills for people with intellectual disabilities. Learning Disability Practice. 17(3): 27-35.
- Goodley D and Moore M. (2000). Doing disability research: Activist lives and the academy. Disability and Society. 15(6): 86-88.
- Garbutt R, Tattersall J, Dunn J and Boycott-Garnett R. (2009). Accessible article: Involving people with learning disabilities in research. British Journal of Learning Disabilities. 38(1): 21-34.
- McDonald KE and Kidney CA. (2012). What is Right: Ethics in intellectual disabilities research. Journal of Policy and Practice in Intellectual Disabilities. 9(1): 27-39.
- Tuffrey-Wijne I and Butler G. (2010). Co-Researching with people with learning disabilities; an experience of involvement in qualitative data analysis. Health Expectations. 13(2): 174-184.
- Roberts A, Greenhill B, Talbot A and Cuzak M. (2011). Standing up for my human rights': A group's journey beyond consultation towards co-production. British Journal of Learning Disabilities. 40(4): 292-301.
- United Nations. (1948). Universal Declaration of Human Rights, United Nations General Assembly. Palais de Chaillot, Paris: United Nations.
- Council for International Organizations of Medical Sciences. (1993). International ethical guidelines for biomedical research involving human subjects. Geneva, Switzerland: World Health Organization.
- Council for International Organizations of Medical Sciences. (2002). International ethical guidelines for biomedical research involving human subjects. Geneva, Switzerland: World Health Organization.
- European Parliament. (2001). Directive 2001/20/EC of the European Parliament and of the Council. Official Journal of the European Communities L121/34 (accessed May 20, 2017).
- Boote J, Telford R and Cooper C. (2002). Consumer involvement in health research: a review and research agenda. Health Policy. 61(2): 213-236.
- Guillemin M and Gillam L. (2004). Ethics, Reflexivity, and "Ethically Important Moments" in Research'. Qualitative Inquiry. 10(2): 261-280.
- Dalton AJ and McVilly KR. (2004). Ethics guidelines for international, multicenter research involving people with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities. 1(2): 57-70.
- Hellstrom I, Nolan M, Nordenfelt L and Lundh U. (2007). Ethical and methodological issues in interviewing persons with dementia. Nursing Ethics. 14(5): 608-619.
- McKeown J, Clarke A, Ingleton C and Reeper J. (2010). Actively involving people with dementia in qualitative research. Journal of Clinical Nursing. 19(13-14): 1935-1943.
- Lennox N, Taylor M, Rey-Conde T, Boyle F, et al. (2005). Beating the barriers: recruitment of people with intellectual disability to participate in research. Journal of Intellectual Disability Research. 49(4): 296-305.
- Tuffrey-Wijne I, Bernal J and Hollins S. (2008). Doing research on people with learning disabilities, cancer and dying: ethics, possibilities and pitfalls. British Journal of Learning Disabilities. 36(3): 185-190.
- Tew J. (2011). Social approaches to mental distress. Basingstoke: Palgrave Macmillan.
- Peel NM and Wilson C. (2008). Frail older people as participants in research. Educational Gerontology. 34(5): 407-417.
- Mumford M D, Connelly S, Brown RP, Devenport LD, et al. (2008). A sensemaking approach to ethics training for scientists: preliminary evidence of training effectiveness. Ethics and Behaviour. 18(4): 315-339.
- Oye C, Sorensen NO and Glasdam S. (2015). Qualitative research ethics on the spot. Nursing Ethics. 23(4): 455- 464.
- Stalker K. (1998). Some ethical and methodological issues in research with people with learning difficulties. Disability and Society. 13(1): 5-19.
- Wadenstein B and Ahlstrom G. (2009). Ethical values in personal assistance: Narratives of people with disabilities. Nursing Ethics. 16(6): 759-774.
- Cambridge P and Forrester-Jones R. (2003). Using individualised communication for interviewing people with intellectual disability: A case study of user-centred research. Journal of Intellectual and Developmental Disability. 28(1): 5-23.
- Baxter L, Thorne L and Mitchell A. (2001). Small voices big noises. Lay involvement in health research: Lessons from other fields. Exeter, Folk.us Programme, University of Exeter.
- Gilbert T. (2004). Involving people with learning disabilities in research: issues and possibilities. Health and Social Care in the Community. 12(4): 298-308.
- Owen F, Griffiths D and Murphy J. (2009). Historical and theoretical foundations of the rights of people with intellectual disabilities: setting the stage. In: Owen F. and Griffiths, D. Challenges to the human rights of people with intellectual disabilities. London: Jessica Kingsley Publishers. 23-42.
- Welch MJ, Lally R, Miller JE, Pittman S, et al. (2015). The ethics and regulatory landscape of including vulnerable populations in pragmatic clinical trials. Clinical Trials. 12(5): 503-510.
- Brooker K, van Dooren K, Tseng CH, McPherson L, et al. (2014). Out of sight, out of mind: The inclusion and identification of people with intellectual disability in public health research. Perspectives in Public Health. 135: 204- 211.
- Northway R. (2014). To include or not to include: That is the ethical question. Journal of Intellectual Disabilities. 18: 209-210.
- Ollerton J. (2012). IPAR, an inclusive disability research methodology with accessible analytical tools. International Practice Development Journal. 2(3): 1-20.
- Frankena TK, Naaldenberg J, Cardol M, Meijering JV, et al. (2016). Exploring academics' views on designs, methods, characteristics and outcomes of inclusive health research with people with intellectual disabilities: a modified Delphi study. BMJ Open. 6(8): e011861.