Information Links
Previous issues
Related Conferences
Previous Issues Volume 4, Issue 2 - 2023
The Adductor Canal Nerve Block: A Simple and Effective Approach for Knee Pain
Girishkumar Modi1,*, Umesh Rawal2
1Specialist Anesthesiologist, Tawam Hospital, UAE
2Vedhasaya Pain and Spine Center, Ahmedabad, India
*Corresponding author: Girishkumar Modi, Specialist Anesthesiologist, Tawam Hospital, UAE, Email: [email protected].
Received Date: July 13, 2023
Published Date: July 26, 2023
Citation: Modi G, et al. (2023). The Adductor Canal Nerve Block: A Simple and Effective Approach for Knee Pain. Mathews J Anesth. 4(2):13.
Copyrights: Modi G, et al. © (2023).
INTRODUCTION
The Adductor Canal, also known as the Hunter Canal, is 8 to 14 cm long and located at the distal two-thirds of the medial thigh. It travels from the apex of the femoral triangle to the adductor hiatus, an aperture in the adductor magnus muscle. The vastus medialis forms the lateral border of the canal, the sartorius forms the medial border, and the adductor longus and magnus muscles form the base. It carries an important structure (saphenous nerve, superficial femoral artery and vein, vastus medialis muscle nerve, and obturator nerve branch) [1] (Figure 1 & 2).
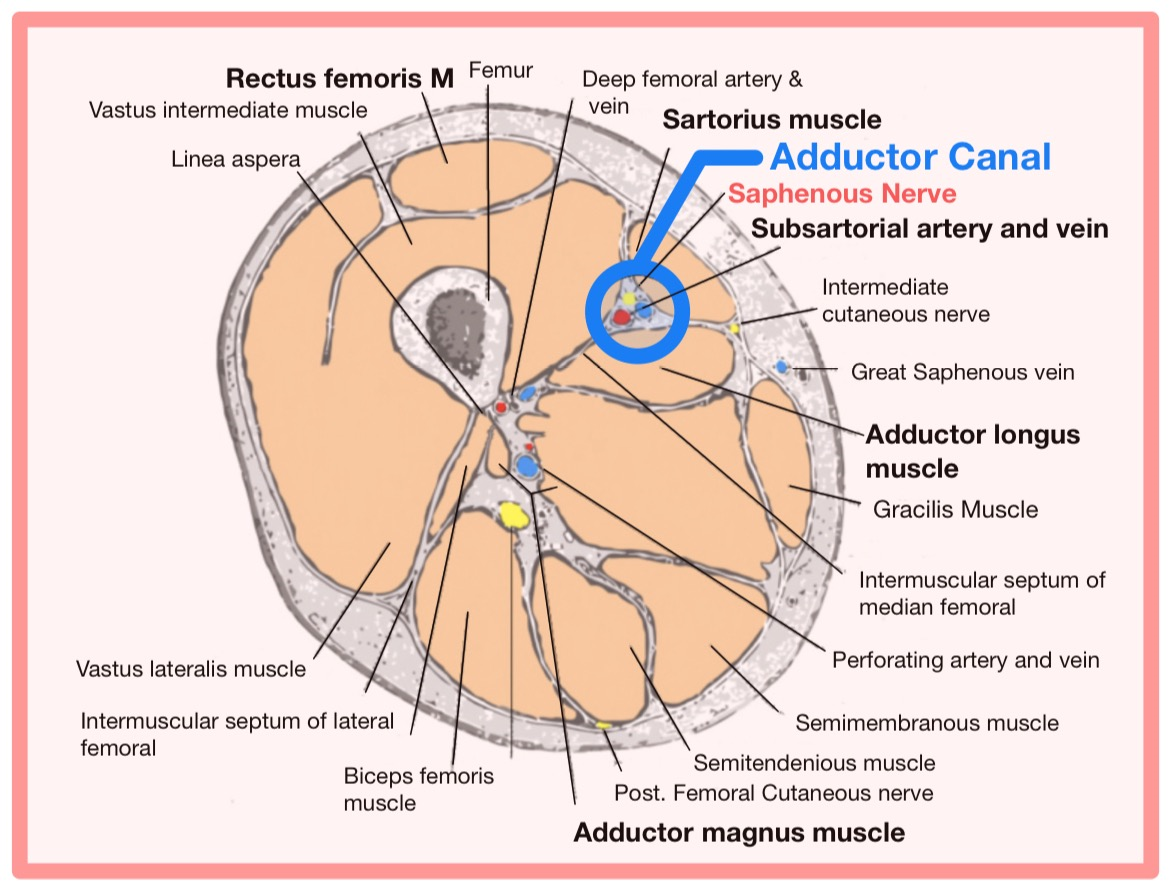
Figure 1. Adductor canal Anatomy through the sagittal section of the thigh. Downloaded from https://en.wikipedia.org/wiki/Adductor_canal#/media/File:Adductor_canal.png
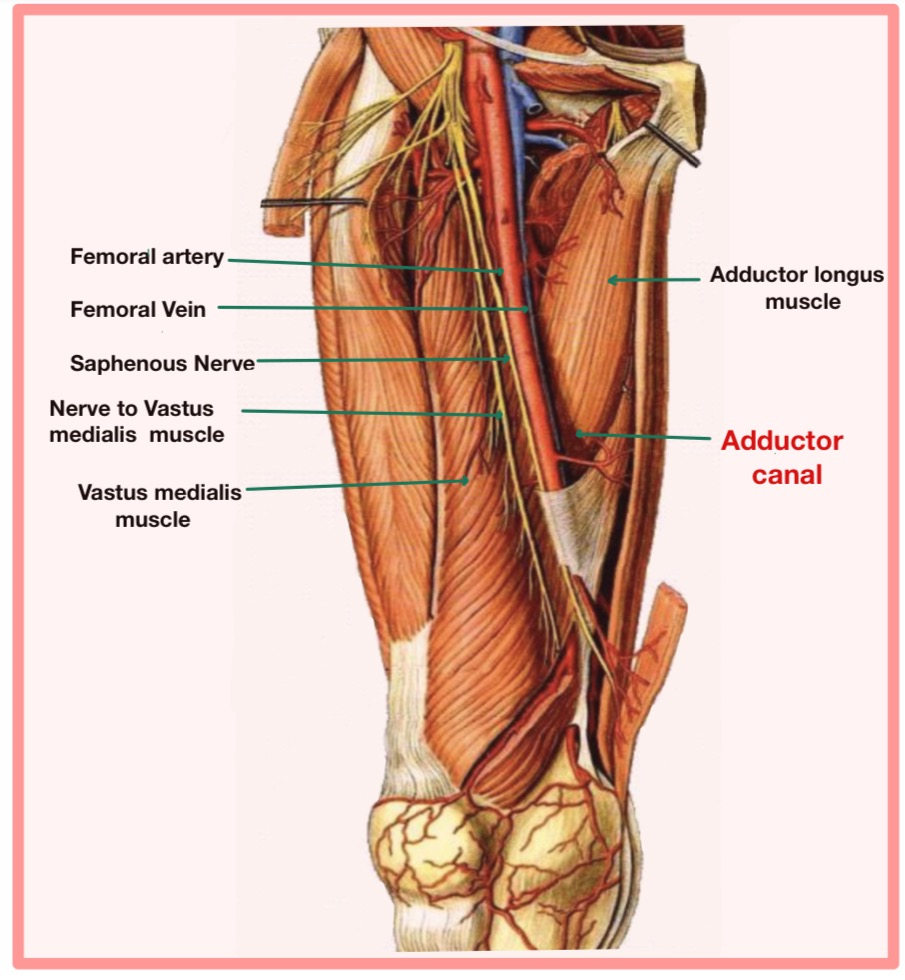
Figure 2. Structures Contained within The Adductor Canal.
In ACNB, we focused on the saphenous nerve, a sensory leading branch of the femoral nerve that supply the skin of the medial, posteromedial, and anteromedial aspects of the lower leg from the distal thigh to the medial malleolus [2]. The main advantage of a saphenous nerve block over a femoral nerve block is that it causes less muscle weakness while providing comparable pain control. This means that, when compared to a femoral nerve block [3], it retains quadriceps motor strength and promotes early mobilization. It splits off from the femoral nerve in the upper third of the thigh, goes down next to the femoral sheath in the adductor canal, crosses in front of the femoral artery, and comes out of the canal with the saphenous branch of the descending genicular artery.
ACNB is used to provide anesthesia and analgesia for knee, medial lower leg, and ankle surgery [4]. It is an alternative approach to femoral nerve block for pain control after various knee procedures, especially knee arthroplasty and arthroscopy [5]. It is quite easy and simple to perform by injecting LA agent deep into the sartorius muscle in the adductor canal, and it is a reliable nerve block in terms of pain relief.
Absolute contraindications for nerve blocks include patient refusal, an allergy to Local Anesthetic (LA) agents, and an infection or contamination at the point of injection. Relative contraindications include coagulopathy and neuropathy [6]. However, it is important for patients to understand the procedure, its benefits, and its potential risks before consenting to a nerve block. Patients should be aware that while nerve blocks can provide effective pain relief, there is a small risk of complications such as nerve damage or infection [7]. Standard fasting recommendations ought to be adhered to, just like general anesthesia. Additionally, obtaining intravenous access is necessary because of the potential for adverse effects like vasovagal syncope and local anesthetic toxicity [7].
Apply standard monitoring in accordance with AAGBI guideline, and keep emergency drugs and an airway trolley on hand to handle any potential local anesthetic toxicity [8]. The patient will lie supine with the leg slightly abducted and externally rotated. The most suitable place for the provider to stand is on the same side of the nerve block and adjusts the patient’s bed height as per the provider's comfort.
Turn on the ultrasound machine and tweak the controls to suit your needs (e.g., depth, gain, and focus). Skin disinfectant should be used to clean the area around the adductor canal nerve block site (typically the medial aspect of the knee) to prevent infection. After applying sterile ultrasound gel, the high-frequency linear probe is positioned transversely perpendicular to the long axis of the leg, just above the medial aspect of the knee, where the saphenous nerve is anticipated to be (Figure 3 & 4).
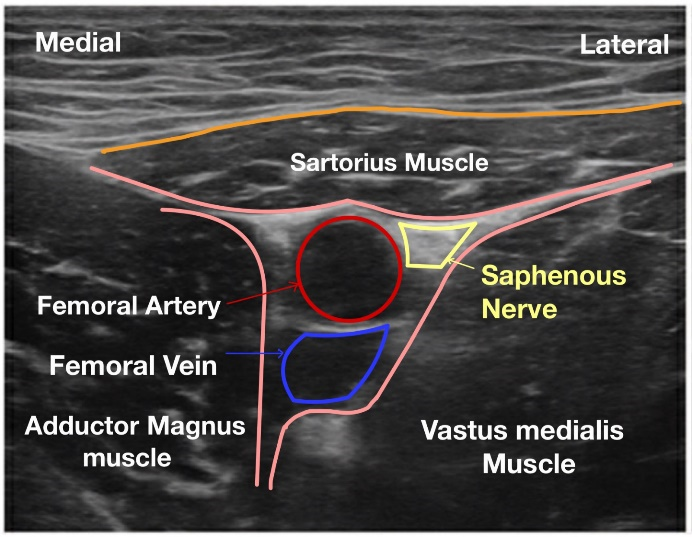
Figure 3. Ultrasound image of the Adductor canal Nerve block.
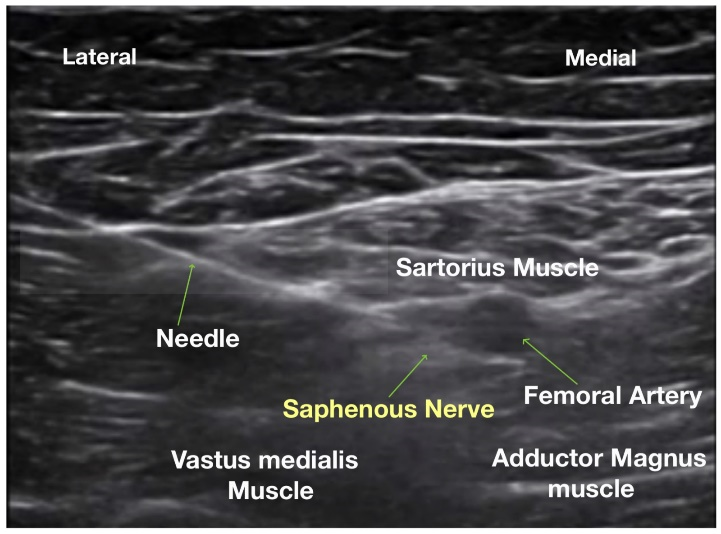
Figure 4. Local anesthetic agent infiltration around the saphenous nerve under USG.
As you scan, you should see several structures, including adductor magnus, vastus medialis, sartorius, and the adductor canal. The Adductor canal is triangular space between these muscles, situated beneath the sartorius muscle. Therefore, it is also called Sub-Sartorial canal.
The saphenous nerve is located within the adductor canal, and it runs adjacent to the adductor longus muscle and the femoral artery. The saphenous nerve is visible as an oval or circular hypoechoic (darker) structure close to the femoral artery; use color doppler to identify the artery if required. After identifying the saphenous nerve, switch the ultrasound probe to the long-axis view to guide needle insertion. After local infiltration at site of injection, insert an 80 mm or 100 mm pujunk needle in an in-plane approach with the ultrasound going from the lateral to the medial side of the thigh. Advance the needle tip just lateral to the femoral artery and underneath to the sartorius muscle. After correct needle placement next to the saphenous nerve after piercing vaso-adductor membrane, a negative aspiration is performed to prevent arterial injection. Inject the local anesthetic (0.5 % ropivacaine, 15-20 ml) incrementally around the saphenous nerve, ensuring that the LA agent spreads to completely cover the nerve [2,9]. Finally, remove the needle and apply gentle pressure and a sterile dressing to the injection site. The patient should experience sensory loss in the medial leg and foot following the block. This block can be performed both pre- and post-operatively. Following the procedure, it is critical to monitor the patient's vitals and look for any complications.
Complications of adductor canal nerve blocks include nerve injury, which can cause temporary or permanent sensory or motor deficits in the affected area, infection, bleeding, or hematoma, allergic reactions, local anesthetic toxicity, and block failure [8].
Adductor canal nerve block can be given continuously using a catheter or as a single shot. Some studies have compared the clinical outcomes of continuous adductor canal block (C-ACB) and Single shot adductor canal block (SACB) after TKA. A meta-analysis of 8 randomized controlled trials involving 702 knees found that C-ACB can achieve better postoperative pain relief at 24 and 48 hours both at rest and after mobilization, a lower amount of opioid consumption at 72 hours, a shorter length of hospital stay, and a larger range of motion than SACB [10]. However, there was no discernible finding among the two methods in terms of quadriceps strength, mobility, and incidence of complications.
To summarize, the adductor canal nerve block is a straightforward, quick, and simple procedure. ACNB represent a novel and efficient form of nerve block that targets the saphenous nerve, a sensory branch of the femoral nerve at the mid-thigh level in the adductor canal for post-operative pain management, particularly in knee surgeries (Knee arthroplasty, knee arthroscopy, and ligament repairs) and assists the patient in early mobilization by preserving quadriceps muscle strength.
ABBREVIATION
ACNB: Adductor Canal Nerve Block; LA: Local Anesthetic; USG: Ultrasonography; C-ACB: Continuous Adductor Canal Block; SACB: Single Shot Adductor Canal Block.
CONFLICT OF INTEREST
None.
FUNDING
None.
REFERENCES
- Steven LO, Barrington M. (2023). Anatomy for the Adductor Canal Block: Does Location Really Matter? Anesth Analg. 136(3):455-457.
- Manickam B, Perlas A, Duggan E, Brull R, Chan VW, Ramlogan R. (2009). Feasibility, and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. Reg Anesth Pain Med. 34(6):578-580.
- El-Ghandour AM, Mohamed AS, Abosief EMK, El‑Fattah Ghoneim MMA, Ahmad AHM, et al. (2022). Saphenous Nerve Block Versus Femoral Nerve Block in Enhanced Recovery After Knee Replacement Surgery Under Spinal Anaesthesia. Ain-Shams Journal of Anesthesiology. 14(1):56.
- Serkan T, Selvi O. (2018). Ultrasound Guided Distal Adductor Canal Block Provides Effective Postoperative Analgesia in Lower Leg Surgery. J Clin Anesth. 45:51.
- Vora MU, Nicholas TA, Kassel CA, Grant SA. (2016). Adductor Canal Block for Knee Surgical Procedures: Review Article. J Clin Anesth. 35:295-303.
- Koşucu M, Beşir A, Eroğlu A, et al. (2013). Peripheral Nerve Block to the Lower Extremity Despite Relative Contraindication (Two Cases). Journal of Anesthesiology and Clinical Science. 2(1):29.
- Chang A, Dua A, Singh K, White BA. (2022). Peripheral Nerve Blocks. StatPearls, NCBI Bookshelf. Peripheral Nerve Blocks-StatPearls. Available at: www.ncbi.nlm.nih.gov/books/NBK459210.
- Amundson AW, Johnson RL. Adductor canal block procedure guide. In Maniker R, Crowley M, editors. USA: UpToDate. Available at: https://www.uptodate.com/contents/adductor-canal-block-procedure-guide/contributors.
- Saad AH, El-Rab NAG, Aly MG, Said HG, et al. (2018). Review Article: Ultrasound-Guided Adductor Canal Block for Post-Operative Analgesia in Knee Arthroscopy. Med J Cairo Univ. 86(9):2141-2148.
- Sun C, Zhang X, Song F, Zhao Z, Du R, Wu S, et al. (2020). Is continuous catheter adductor canal block better than single-shot canal adductor canal block in primary total knee arthroplasty? A GRADE analysis of the evidence through a systematic review and meta-analysis. Medicine (Baltimore). 99(20):e20320.