Information Links
Related Conferences
Previous Issues Volume 8, Issue 4 - 2023
Which Bladder Filling Method for Pelvic Ultrasound is best? A Comparison Study of Three Standard Non-Foley-Catheter-Based Bladder Filling Methods (Oral, Intravenous, Oral/IV) in Preparation for Pelvic (Transabdominal) Ultrasound
Amelia Servin1, Amber McPherson2, James Espinosa3,*, Victor Scali4, Alan Lucerna5, Henny Schuitema6
1Department of Emergency Medicine, Providence Centralia Hospital, Centralia, WA, USA
2Department of Emergency Medicine, Willamette Valley Medical Center, McMinnville, OR, USA
3Department of Emergency Medicine, Jefferson NJ, Stratford, NJ, USA
4Director of Problem-Based Learning and Faculty, Rowan-Virtua SOM School of Medicine, Stratford, NJ, USA
5Program Director, Emergency Medicine Residency Program, Jefferson Health-New Jersey Stratford, NJ, USA
6Chief, Department of Emergency Medicine and Associate Chief Medical Officer, Jefferson NJ, USA
*Corresponding Author: James Espinosa MD, Department of Emergency Medicine, Jefferson Health NJ, 18 East Laurel Road, Stratford, NJ 08084; Email: [email protected]
Received Date: June 20, 2023
Publication Date: July 7, 2023
Citation: Servin A, McPherson A, Espinosa J, Scali V, Lucerna A, Schuitema H. (2023). Which Bladder Filling Method for Pelvic Ultrasound is best? A Comparison Study of Three Standard Non-Foley-Catheter-Based Bladder Filling Methods (Oral, Intravenous, Oral/IV) in Preparation for Pelvic (Transabdominal) Ultrasound. Mathews J Emergency Med. 8(4):61.
Copyright: Servin A, et al. © (2023)
ABSTRACT
Background: Pelvic ultrasound is generally performed in two parts, transabdominal ultrasound and transvaginal ultrasound. In order to obtain the best images and the greatest chance at a diagnosis, the consensus appears to be that patients must have a full bladder prior to undergoing pelvic ultrasound. A commonly used operational definition of a full bladder is 250 to 300 cc. Patients can be given fluids by mouth, or intravenously (as an IV bolus). Both approaches can be used. Some scenarios (nausea, pre-operative status, etc) may favor one approach over another. It is also possible to fill the bladder with a Foley catheter which remains in place for the duration of the study. Materials and Methods/Research Design and Methods: The purpose of this study was to determine which of the current non-Foley catheter-based methods of bladder-filling (IV bolus, oral fluid intake, or a combination of both) most rapidly produces an adequately filled (> 250 cc) bladder volume for pelvic ultrasound. The setting was three community hospital/university-affiliated emergency departments.
The design was prospective with subjects randomly assigned to one of three treatment groups: 1) 1,000 cc normal saline bolus administered IV over 1 hour, 2) Oral ingestion of 32 ounces water (with ice in cup) with or without added flavoring (e.g. Crystal Light) per patient preference 3) Bladder to be filled through combination of the above methods performed simultaneously (i.e. 1L NS IVF bolus and 32 oz. water). Results: The fastest filling was with the oral route. The slowest was with the IV route. The difference in filling (in the direction of faster filling) was highly statistically significant in reference to the oral vs. the IV route. (p=0.001) There was no statistical significance in reference to the comparison of the combined route (IV/PO) vs oral or IV, and hence no advantage seen for the combined routes in reference to filling speed. The greatest change in volume was seen with the oral route and the slowest was with the IV route. The oral route showed a statistically significant difference, in the direction of a larger filling delta, with oral route in comparison to both the IV route (p=0.001) as well as in comparison to the combined (IV/PO) route (p=0.03). There was no statistically significant difference noted in comparison of the various routes in reference to time to US. Discussion: The fastest filling was with the oral route. The slowest was with the IV route. There was no statistically significant difference noted in comparison of the various routes in reference to time to ultrasound. Time to ultrasound is affected by system properties that are more complex than time to filling. Conclusions: The fastest filling was with the oral route. The slowest was with the IV route. There was no statistically significant difference noted in comparison of the various routes in reference to time to ultrasound. Time to ultrasound is affected by system properties that are more complex than time to filling. Future research might show the advantage of optimizing ultrasound cycle time by coordinating ultrasound acquisition in the ED setting with a full bladder.
Keywords: Pelvic ultrasound; Bladder filling method; Bladder volume; Transabdominal ultrasound
INTRODUCTION
Ultrasound first emerged as a diagnostic imaging tool in the 1950’s, although its earliest form was so crude as to have limited utility. As technology has improved, ultrasound has become a routinely used and vital tool within the practice of medicine. One area in which ultrasound has assumed a particularly important role is in the field of obstetrics and gynecology [1,2]. Ultrasound, now readily available in most EDs, is the imaging modality of choice for these patients. Pelvic ultrasound is generally performed in two parts, transabdominal ultrasound and transvaginal ultrasound. The transabdominal ultrasound is generally more successful if the patient has what is referred to as a “full bladder” as this helps to clear bowel and bowel gas from the field and aid transmission of the ultrasound signal to the more posterior pelvic organs (i.e. the uterus and ovaries). The transvaginal approach does not require a full bladder and has the advantage of closer proximity, and therefore frequently better visualization, of the pelvic organs. However, transvaginal ultrasound has limited range and may not be able to visualize pathology associated with those areas of the uterus or pelvis most distal to the probe. Therefore, most radiologists prefer that both approaches be included for a full evaluation of the pelvic organs. Furthermore, not all patients will tolerate or agree to transvaginal imaging, leaving transabdominal ultrasound as the only option in some cases. In order to obtain the best images and the greatest chance at a diagnosis, the consensus appears to be that patients must have a full bladder prior to undergoing pelvic ultrasound [3].
The literature shows that there has been some intermittent challenge to this premise, but it appears that a full bladder protocol for an optimal study is the general practice currently [4].
A very important issue then is the operational definition of a full bladder. A commonly used operational definition of a full bladder is 250 to 300 cc. It is intuitively obvious that there are several possible approaches to bladder filling. Patients can be given fluids by mouth, or intravenously (as an IV bolus). Both approaches can be used. Some scenarios (nausea, pre-operative status, etc.) may favor one approach over another. It is also possible to fill the bladder with a Foley catheter which remains in place for the duration of the study.
Which of the three standard non-Foley-catheter-based methods is best? A review of the literature (PubMed) does not appear to return an answer to this rather practical question. The purpose of this study is to determine which of the current non-Foley used methods of bladder-filling (IV bolus, oral fluid intake, or a combination of both) most rapidly produces an adequately filled bladder for pelvic ultrasound.
MATERIALS AND METHODS
The purpose of this study was to determine which of the current non-Foley catheter-based methods of bladder-filling (IV bolus, oral fluid intake, or a combination of both) most rapidly produces an adequately filled (> 250 cc) bladder volume for pelvic ultrasound. The setting was three community hospital/university-affiliated emergency departments.
The design was prospective with subjects randomly assigned to one of three treatment groups: 1) 1,000 cc normal saline bolus administered IV over 1 hour, 2) Oral ingestion of 32 ounces water (with ice in cup) with or without added flavoring (e.g. Crystal Light) per patient preference 3) Bladder to be filled through combination of the above methods performed simultaneously (i.e. 1L NS IVF bolus and 32 oz. water). The study was IRB approved and written consent was obtained from all participants.
Prior to beginning any filling method, the patient had a bladder scan to assess initial bladder volume. Patients with a starting volume >200 cc were excluded.
The patients then had additional bladder scans at 20 minute intervals, with additional scans for patient’s self-reported sensation of fullness, until a volume >250 cc is achieved.
The sample size was 10 subjects minimum in each of the three groups, for a total 30 subjects minimum. .Inclusion criteria included female patient between the ages of 18 and 65 year old, who were hemodynamically stable and, in the ordinary course of their treatment, would require a pelvic ultrasound for evaluation of complaints of vaginal bleeding, vaginal bleeding in pregnancy, lower abdominal pain, or pelvic pain. Patients will be excluded who are less than 18 years old, greater than 65 years old, or are hemodynamically unstable. Also, patients will be excluded who have an initial bladder volume >200 cc as well as patients with vomiting not adequately controlled with medication.
STATISTICAL ANALYSIS
Groups will be compared using Student's T test.
RESULTS
The results for filling rates in cc/min are noted below (Tables 1, 2 and Figure 1).
The fastest filling was with the oral route. The slowest filling was with the IV route. The difference in filling (in the direction of faster filling) was highly statistically significant in reference to the oral vs. the IV route. (p=0.001) There was no statistical significance in reference to the comparison of the combined route (IV/PO) vs oral or IV, and hence no advantage seen for the combined routes in reference to filling speed.
The results for total change in volume in cc/min are noted below (Tables 3, 4, and Figure 2). The greatest change was seen with the oral route and the slowest was with the IV route. The oral route was showed a statistically significant difference, in the direction of a larger filling delta, with oral route in comparison to both the IV route (p=0.001) as well as in comparison to the combined PO/IV route (p=0.03)
The times to ultrasound for each route are summarized below (Tables 5,6 and Figure 3). There was no statistically significant difference noted in comparison of the various routes in reference to time to US.
Descriptive Statistics: cc/min
Table 1
|
Variable |
Route_3 |
Mean |
StDev |
Median |
|
cc/min |
IV |
3.058 |
1.431 |
3.050 |
|
oral |
5.850 |
2.046 |
5.595 |
|
|
oral and IV |
4.89 |
3.47 |
3.79 |
Table 2
|
cc/min |
|
|
Oral vs IV |
0.001 |
|
Oral vs PO/IV combined |
NS |
|
IV vs PO/IV combined |
NS |
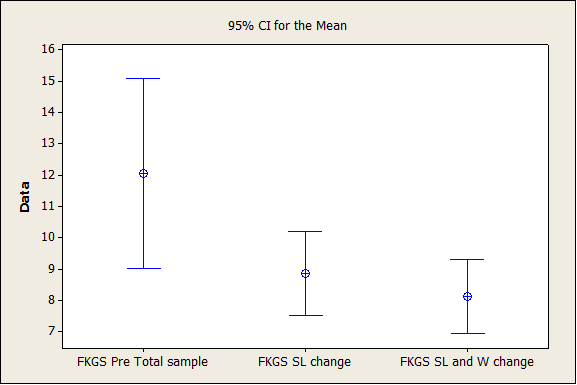
Figure 1
Descriptive Statistics: delta volume
Statistics
Table 3
|
Variable |
Route_3 |
Mean |
StDev |
Median |
|
delta volume |
IV |
176.7 |
78.0 |
173.0 |
|
oral |
352.9 |
124.6 |
389.5 |
|
|
oral and IV |
242.5 |
109.4 |
228.0 |
Table 4
|
delta filling |
|
|
Oral vs IV |
0.001 |
|
Oral vs PO/IV combined |
0.03 |
|
IV vs PO/IV combined |
NS |
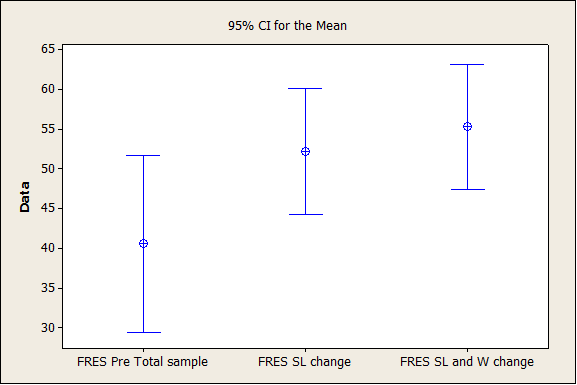
Figure 2
Descriptive Statistics: minutes to US
Statistics
Table 5
|
Variable |
Route_3 |
Mean |
StDev |
Median |
|
minutes to US |
IV |
68.5 |
41.6 |
60.0 |
|
oral |
63.00 |
18.89 |
62.00 |
|
|
oral and IV |
61.17 |
31.06 |
60.50 |
Table 6
|
Time to US (minutes) |
|
|
Oral vs IV |
NS |
|
Oral vs PO/IV combined |
NS |
|
IV vs PO/IV combined |
NS |
Figure 3
DISCUSSION
The fastest filling was with the oral route. The slowest was with the IV route. The difference in filling (in the direction of faster filling) was highly statistically significant in reference to the oral vs. the IV route. (p=0.001) There was no statistical significance in reference to the comparison of the combined route (IV/PO) vs oral or IV, and hence no advantage seen for the combined routes in reference to filling speed.
This is supported by data concerning the total change in amount (in cc) by route. The greatest change was seen with the oral route and the slowest was with the IV route. (Table below). The oral route was showed a statistically significant difference, in the direction of a larger filling delta with the oral route in comparison to both the IV route (p=0.001) as well as in comparison to the combined PO/IV route (p=0.03)
The ultrasound bladder scan approach to determining bladder volume has been shown to be accurate [5,6].
No comparable studies are available for comparison.
CONCLUSIONS
The fastest filling was with the oral route. The slowest filling was with the IV route. The difference in filling (in the direction of faster filling) was highly statistically significant in reference to the oral vs. the IV route. (p=0.001) There was no statistical significance in reference to the comparison of the combined route (IV/PO) vs oral or IV, and hence no advantage seen for the combined routes in reference to filling speed. This is supported by data concerning the total change in amount (in cc) by route. The greatest change was seen with the oral route and the slowest was with the IV route. (Table below). The oral route was showed a statistically significant difference, in the direction of a larger filling delta, with oral route in comparison to both the IV route (p=0.001) as well as in comparison to the combined PO/IV route (p=0.03) The data suggest that the oral filling route if preferable when clinically possible and that there is no advantage to the combined IV/PO route.
REFERENCES
- Woo J. A short history of the development of ultrasound in Obstetrics and Gynecology.
- Cosgrove DO, Meire HB, Lim A, Eckersley RJ. (2008). Ultrasound: general principles. In: Adam A, Dixon AK. (5Th) Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging. New York, NY: Churchill Livingstone.
- http://www.hopkinsmedicine.org/healthlibrary/test_procedures/gynecology/pelvic_ultrasound_92,P07784/
- Benacerraf BR, Shipp TD, Bromley B. (2000). Is a full bladder still necessary for pelvic sonography? J Ultrasound Med. 19:237–241.
- Poston GJ, Joseph AE, Riddle PR. (1983). The accuracy of ultrasound in the measurement of changes in bladder volume. Br J Urol. 55(4):361-363.
- Al-Shaikh G, Larochelle A, Campbell CE, Schachter J, Baker K, Pascali D. (2009). Accuracy of bladder scanning in the assessment of postvoid residual volume. J Obstet Gynaecol Can. 31(6):526-532.