Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2024
Unveiling Nosocomial Urinary Tract Infections: Insights from the University Hospital of Casablanca's Urology Department
Mahmoud Al-Affifi*, Yassine Larrache, Saleh Nedjim, Amine Moataz, Mohammed Dakir, Adil Debbagh, Rachid Aboutaieb
Department of Urology, Ibn Rochd HUC, Casablanca, Morocco
*Corresponding author: Dr. Mahmoud Al-Affifi, Department of Urology, Ibn Rochd HUC, Casablanca, Morocco, Phone: 00212700148612, E-mail: [email protected].
Received Date: February 29, 2024
Published Date: March 15, 2024
Citation: Al-Affifi M, et al. (2024). Unveiling Nosocomial Urinary Tract Infections: Insights from the University Hospital of Casablanca's Urology Department. Mathews J Urol Nephrol. 6(1):15.
Copyrights: Al-Affifi M, et al. © (2024).
ABSTRACT
Hospital-acquired urinary tract infections (UTIs) are increasingly prevalent, posing a significant challenge to public health due to their contribution to higher mortality rates and healthcare costs. This retrospective analysis spans one year, from January to December 2023, and excludes any patient admitted with an existing or active UTI. Out of 375 cases evaluated, the occurrence rate of hospital-acquired UTIs stood at approximately 14%. The average hospital stay was noted as 2.3 days, within a range of 3 to 5 days. E. coli was identified as the responsible pathogen in 37% of the instances. The patients had a mean age of 53.2 years, spanning from 17 to 87 years, with a male-to-female ratio of 2.9. Bladder cancer follow-ups emerged as the most common consultation reason. Significant risk factors included previous hospital stays, antibiotic use, bladder catheterization, and the use of JJ stents. Our findings align with existing literature on risk factors for hospital-acquired UTIs, the prevalence of enterobacterial infections, and the rise of resistant bacterial strains. Carbapenems were the most effective treatment, followed by amikacin, with a 65.33% rate of urine sterilization by day 3 post-treatment.
Keywords: Urinary Tract Infections, Antibiotic Use, Healthcare Costs, Mortality, Resistant Bacterial Strains.
LIST OF ABBREVIATIONS
UTIs: Urinary Tract Infections; CBUE: Cytobacteriological Urine Examination; BGN: Gram-Negative Bacilli; CGP: Gram-Positive Cocci; ESBLs: Extended-Spectrum Beta-Lactamases ; PCN: Percutaneous Nephrostomy ; TURP: Transurethral Resection of the Prostate; TURB: Transurethral Resection of Bladder Tumor.
D3, D7, D10 - Day 3, Day 7, Day 10 (related to treatment outcomes).
INTRODUCTION
Hospital-acquired urinary tract infections (UTIs) represent the most frequent type of infection within hospital settings, making up to 40% of all nosocomial infections. These infections are particularly significant in the field of urology, presenting a substantial public health issue due to the increased mortality and financial burdens they cause. Individuals in urology wards or those using bladder catheters are at an elevated risk of contracting these infections. The pathogens causing hospital-acquired UTIs can originate from both internal (endogenous) and external (exogenous) sources, with prevention being the cornerstone of management.
To enhance the scope of our study, we have also considered the impact of urinary tract obstruction on the prevalence of hospital-acquired UTIs. This expanded frame of reference allows for a more comprehensive analysis of the factors contributing to these infections, including how urinary tract obstructions may predispose patients to UTIs or complicate their clinical course.
Our study aims to assess the prevalence and complexity of nosocomial UTIs, identify associated risk factors, including the role of urinary tract obstruction, determine the proportion of pathogens responsible, evaluate antibiotic resistance patterns, and observe treatment outcomes.
MATERIALS AND METHODS
Study population
Our research is a retrospective descriptive study that encompasses all microbiologically confirmed urinary tract infections within the urology department at CASABLANCA University Hospital over a one-year span (January to December 2023). This study scrutinized cytobacteriological urine test data from adult patients aged between 17 and 87 years. We included urine samples collected in the CASABLANCA University Hospital's urology department. Any patients admitted with an existing or active urinary tract infection were excluded from this analysis.
Definitions And Methodology
An infection is classified as nosocomial under three conditions:
- No urinary tract infection was evident or incubating at the time of admission.
- An existing urinary tract infection was present, yet the identified microorganism differed, or the prior infection had been declared resolved.
- The patient's initial condition was uncertain, and the infection manifested more than 48 hours post-admission.
A nosocomial urinary tract infection (UTI) is identified by one or more of the following symptoms in the absence of any other cause, infectious or otherwise: Fever (> 38°C), urinary urgency, frequent urination, burning sensation, or suprapubic pain. Criteria include: Without bladder catheterization or recent urinary intervention, exhibiting ≥ 104 leukocytes/ml (leukocyturia) and a positive uroculture of ≥ 103 microorganisms/ml with no more than two distinct microorganisms. With recent bladder catheterization or urinary intervention, showing a positive uroculture of ≥ 105 microorganisms/ml with no more than two distinct microorganisms. A UTI is deemed complicated by the presence of certain conditions such as vesico-ureteral reflux, lithiasis, tumors, diabetes, renal failure, immunosuppression, male gender, pregnancy, or an elderly patient with comorbidities.
Statistical Analysis
The study analyzed both quantitative and qualitative variables, summarized in Table 1. Data collection was based on a detailed evaluation form that covered all necessary parameters to achieve our research goals. The essential paraclinical test was the CBUE, which included uroculture for germ enumeration, a direct examination for leukocyturia and urine sediment (e.g., red blood cells, crystals), and a direct examination for bacterial presence.
Ethical considerations were strictly observed during data collection, adhering to the deontology committee of Ibn Rochd Hospital's guidelines, including obtaining patient consent, ensuring data confidentiality, and maintaining patient anonymity regarding their condition, infection, and underlying diseases. Discrete variables were presented as numbers and percentages and analyzed using the Chi-square test, with statistical significance set at a p-value < 0.05.
RESULTS
In this study, we observed 375 cases of hospital-acquired urinary tract infections, consisting of 95 females (25.5%) and 280 males (74.5%), resulting in a male to female ratio of approximately 2.9:1. The participants' average age was 58.4 years, with a range from 17 to 87 years.
The primary reasons for seeking medical consultation were bladder tumors, accounting for 36% of the cases, followed by urinary stone disease at 21.3% (Table 1).
Table 1. Percentage of nosocomial UTIs by reason for hospitalisation
|
Motif of hospitalisation |
Number |
% |
|
Bladder tumour |
135 |
36% |
|
Renal lithiasis |
80 |
21,3% |
|
Prostate adenoma |
40 |
10,66% |
|
Urethral stenosis |
20 |
5 ,33% |
|
Cervical cancer |
30 |
8% |
|
Cancer of the prostate |
20 |
5.33% |
|
Neurological bladder |
8 |
2,13% |
|
Fournier's gangrene |
10 |
2,66 % |
|
Renal fracture |
2 |
0,53% |
|
Vesico-vaginal fistula |
10 |
2.66% |
|
Total |
375 |
100% |
Out of the total, 307 patients had a history of hospital admission (82.7%), whereas 68 had not been previously hospitalized (17.3%). The study noted the average hospital stay to be around 2.31 days (ranging from 2 to 5 days).
A notable 43.2% of the patients had undergone antibiotic therapy prior to the current episode. Hospital-acquired infections were particularly common among individuals with bladder catheters (44%) and those with ureteral stents (25%).
Symptoms
Upon hospitalization, fever was reported in 44.2% of the cases. Additionally, 36.5% of the patients experienced lower back pain, 62.5% displayed irritative symptoms, and obstructive symptoms were present in 39.4% of the cases.
Cytobacteriological Urine Examination (CBUE)
The examination revealed that 67.3% (252 patients) had cloudy urine, 17.6% (66 patients) had bloody urine, and 15.4% (57 patients) had slightly cloudy urine.
Direct Examination
The direct examination showed gram-negative bacilli (BGN) in 71.2% of the cases, gram-positive cocci (CGP) in 28.8%, and one instance where the examination yielded no bacterial growth.
Bacterial Ecology (Uroculture)
The culture results identified E. coli as the most prevalent bacterium in 37.3% of the cases, followed by Acinetobacter B. in 17.06% and Klebsiella P in 16.8% (Table 2). Notably, E. coli produced extended-spectrum beta-lactamases (ESBLs) in 50% of these instances (Graph I).
Table 2. Type of Germin nosocomial UTIs
|
Germs |
Number |
% |
|
E.coli |
140 |
37,3 |
|
Klebsiella.P |
63 |
16,8 |
|
Enterococcus. F |
62 |
16,53 |
|
Enterococcus. C |
16 |
4,26 |
|
Acinobacter B |
64 |
17,06 |
|
Proteu .M |
16 |
4.26 |
|
Pseudomonas. A |
4 |
1.06 |
|
Morganella. M |
3 |
0.8 |
|
E.coli, Morganela. M, Staphyloccocus. A |
3 |
0.8 |
|
Citrobacter. F, Pseudomonas. A |
2 |
0,53 |
|
Candidat ALbicans |
2 |
0,53 |
|
Total |
375 |
100 |
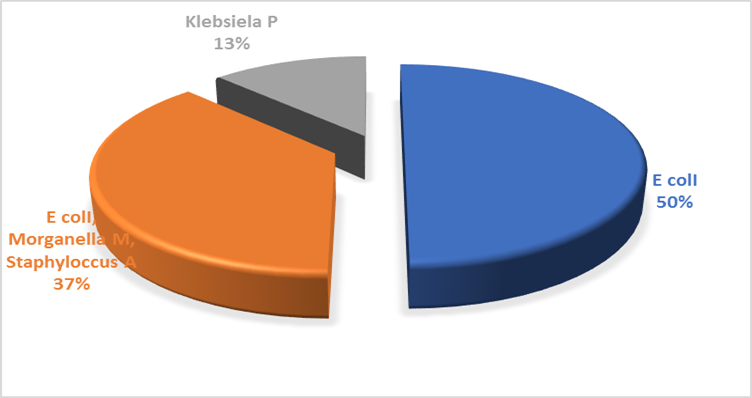
Graph I. Distribution of organisms secreting Beta Lactamases (ESBL).
A further analysis of bacterial ecology relative to risk factors (Graph II) indicated that E. coli was particularly common in 50% of patients with percutaneous nephrostomy (PCN), 44.4% with bladder catheters, and 16% with ureteral stents. The distribution of Klebsiella pneumoniae SSP pneumoniae and Enterococcus Faecalis varied based on the type of urinary intervention. Acinetobacter B. showed a significant presence in PCN patients and those with bladder catheters.
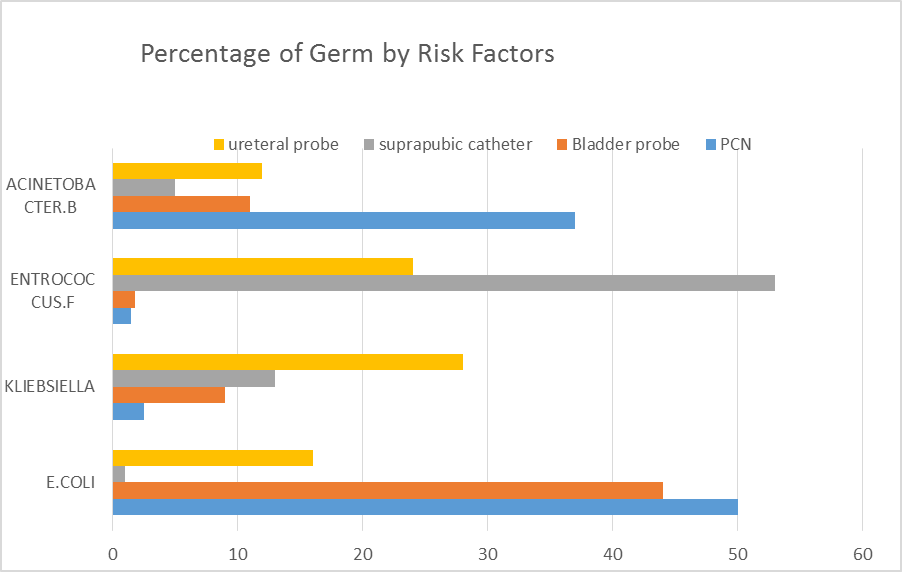
Graph II. Germ ecology as a function of risk factors
Antibiotic Sensitivity Profile
E. coli demonstrated a high sensitivity to carbapenems (95%) and moderate sensitivity to amikacin (37.5%). A small proportion (5%) of E. coli strains were resistant to all tested antibiotics, except for colimycin and rifampicin (Table 3). Acinetobacter B. exhibited resistance to most antibiotics in 62.35% of the cases but was somewhat sensitive to imipenem and amikacin (Table 4). Klebsiella pneumoniae SSP showed good sensitivity to carbapenems but also had a resistance rate to the antibiotics tested (Table 5).
Table 3. Frequency of sensitivity of Escherichia coli to antibiotics
|
Antibiotics active on E. coli |
Number |
Frequency of sensitivity |
|
Ertapenem |
54 |
95% |
|
Imipenem |
48 |
95% |
|
Amikacine |
27 |
80% |
|
Gentamycine |
5 |
60% |
|
3rd generation cephalosporins |
3 |
60% |
|
No active antibiotic |
3 |
0% |
|
Antibiotiques actifs sur Acintobacter.B |
Number |
Frequency |
|
Amikacine |
4 |
6,25% |
|
Imipenem |
10 |
15,7% |
|
Ertapenem |
10 |
15,7% |
|
No active antibiotic |
40 |
62,35% |
|
Antibiotique actif sur Klebsiella Pneumonie SSP |
Number |
Frequency |
|
Ertapeneme |
21 |
32,8% |
|
Imipenem |
21 |
32.80% |
|
Amikacine |
14 |
21.80% |
|
Aucun antibiotique actif |
8 |
12.60% |
Carbapenems were the most commonly prescribed antibiotics, used in 56% of the cases, followed by amikacin in 26% (Graph III).
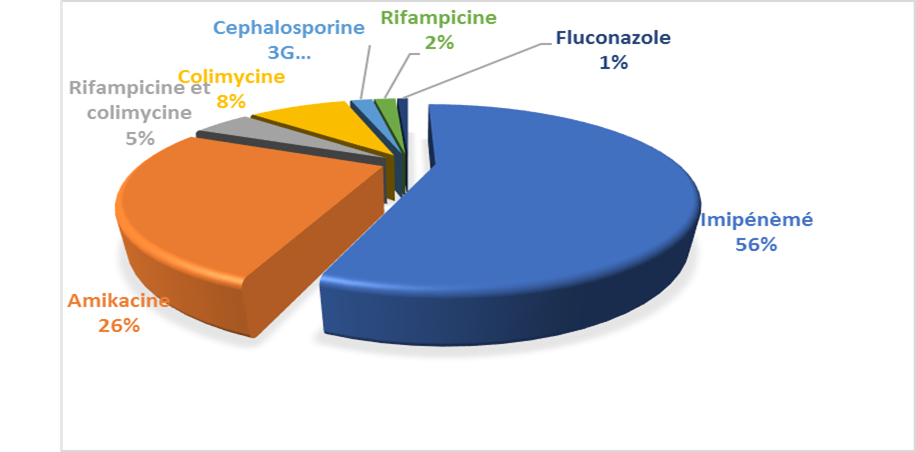
Graph III. Profile of antibiotics used for the management of nosocomial infections
Treatment outcomes showed that by day 3 (D3), 65.33% of patients had sterile urine samples. By day 7 (D7), this increased to 29.7%, and by day 10 (D10), 3.20% achieved urine sterilization, with 1.80% of the cases still presenting with infected urine samples (Graph IV).
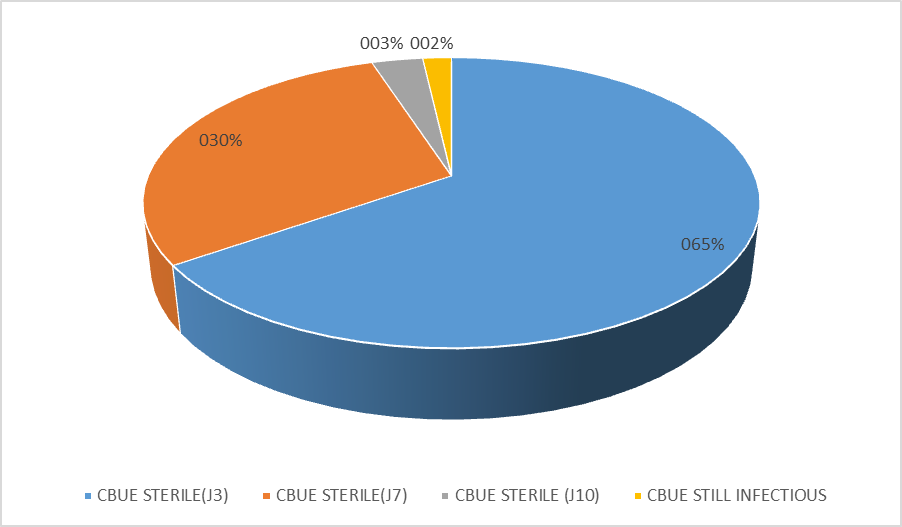
Graph IV. Progress with Antibiotics.
DISCUSSION
A urinary tract infection (UTI) is characterized by the presence of significant bacteriuria coupled with symptoms indicative of a UTI, in the absence of infection in other sites. This criterion sets it apart from urinary colonization, where significant bacteriuria exists without symptoms [1].
The manifestations of a UTI can range widely, from specific symptoms like dysuria and frequent urination to non-specific symptoms such as fever, chills, malaise, psychomotor slowdown, or even confusion in older adults [2].
UTIs are classified as community-acquired when they are not associated with medical intervention or healthcare settings [3]. The previous classifications of UTIs as either upper or lower have been replaced by the terms simple or complicated UTIs. A UTI is deemed complicated in the presence of at least one risk factor, which could be an anatomical or functional abnormality of the urinary system, specific conditions (pregnancy, immunosuppression, elderly, diabetes, etc.), or being male. The presence of urinary tract obstruction is also considered a significant risk factor for complicated UTIs, as it can impede urine flow and facilitate bacterial colonization and infection [4].
Nosocomial UTIs, identified not at admission but after 48 hours of hospital stay [5], primarily originate endogenously from the patient's own flora [6]. In patients without catheters, the ascending route is the typical mode of acquisition for nosocomial UTIs, while for catheterized patients, infection may arise extraluminally from perineal or urethral flora introduced into the bladder, or endoluminally from bacteria within the catheter [7]. Transmission through blood or lymph from an endogenous source has been proposed but remains uncertain [8]. Other nosocomial infection pathways include cystoscopy, suprapubic catheterization, and intravesical procedures [6].
UTI origins are categorized as either endogenous, involving the patient's bacteria, or exogenous, from germs transmitted via non-sterile equipment or the hospital environment (water, air, food, etc.) [9].
In this study, nosocomial UTIs constituted 14% of cases. Comparing this to other studies reveals a wide variability; one study at the UHC urology department in FES reported a 39% incidence, while another in TUNISIA found it to be below 10% [10,11].
Research in Morocco indicates a higher prevalence of nosocomial UTIs in men, likely due to the prevalence of prostate issues. The obstruction caused by enlarged prostate or other urinary tract obstructions significantly contributes to this gender disparity [12]. The incidence rises with age [13], as seen in our study with an average participant age of 53.2 years, which is attributed to decreased urinary flow, urinary tract hypotonia, and weakened immune defenses in older adults [14].
Diabetes predisposes individuals to nosocomial UTIs by causing bladder dysfunction through peripheral neuropathy and promoting bacterial growth via glycosuria [15]. In our research, 4% of cases involved diabetic patients. Other risk factors include a history of UTIs, anatomical or functional urinary tract abnormalities, immunosuppression, and pregnancy. Urinary tract obstruction, as a standalone factor or in conjunction with other conditions, markedly increases the risk of developing nosocomial UTIs [15].
Bladder catheterization is a standard practice in urology for urinary surgeries. The risk of UTI is associated with the catheterization method, catheter duration and type, and patient health status. Catheterization significantly influences UTI development, though opinions on its impact vary [16,17]. Our study noted catheter use in 44% of nosocomial UTI cases. Hospital stays alter the patient's skin flora. Extended pre-operative periods heighten the risk of decubitus complications and are often linked to invasive explorations, posing a significant risk of septic complications [15]. Our average hospitalization duration was 2.3 days. Endoscopic procedures, particularly TURP and TURB, carry the highest UTI risk, aligning with numerous urological studies identifying these as frequent postoperative UTI sources. The manipulation of the urinary tract during these procedures can exacerbate existing obstructions or create new ones, further elevating UTI risk [18]. Our study found UTIs commonly in patients treated for bladder tumors or renal lithiasis.
Antibiotic prophylaxis aims to decrease the incidence of surgical site infections, whether superficial or deep [19]. In our cohort, 43.2% had undergone prior antibiotic treatment. The study highlighted a predominance of enterobacteria, especially Escherichia coli, at 37.3%, followed by ACINTOBACTER B (17.6%), Klebsiella pneumoniae (16.8%), Enterococcus F (16.3%), among others. These findings align with several Moroccan studies reporting a higher prevalence of Escheria coli in UTIs: 65% in the study by Lahlou A et al. and 61% by Fettouh A et al. [17,20-24].
CONCLUSION
In conclusion, our comprehensive study sheds light on the significant burden of nosocomial urinary tract infections (UTIs) within the urology departments, highlighting an incidence rate of 14%. The research underscores Escherichia coli as the leading causative agent of these infections, a finding consistent with global patterns but crucial for tailoring local antibiotic stewardship programs. Among the myriad factors contributing to the prevalence of nosocomial UTIs, the utilization of bladder and urethral catheters stood out as predominant. This emphasizes the imperative need for stringent aseptic techniques during urinary interventions, whether conducted in the operating room, emergency departments, or within the inpatient setting.
Our study introduced several innovations to the field of urological research on nosocomial infections. For the first time, we incorporated a detailed analysis of urinary tract obstruction's role in predisposing patients to UTIs, thereby broadening our understanding of risk factors beyond the commonly acknowledged ones. This novel approach allows healthcare providers to identify at-risk patients more accurately and implement preventive measures proactively.
Moreover, our research contributes to the ongoing conversation about antibiotic resistance patterns. By evaluating the susceptibility of Escherichia coli to various antibiotics, we provide essential insights that can guide the development of more effective treatment protocols, addressing the growing concern of antibiotic-resistant pathogens. The finding that E. coli showed a significant resistance pattern, particularly the production of extended-spectrum beta-lactamases (ESBLs), underscores the urgency of adopting judicious antibiotic use in hospital settings.
The meticulous examination of treatment outcomes, highlighted by the proportion of patients achieving urine sterilization at various intervals post-treatment, offers a valuable benchmark for evaluating the efficacy of UTI management strategies in hospitalized patients. Our research suggests an encouraging success rate, with a substantial majority of patients responding positively to treatment by day 3 (D3). However, the persistence of infection in a small fraction of patients by day 10 (D10) underscores the need for ongoing vigilance and possibly reevaluation of treatment approaches in cases of delayed response.
In light of our findings, the importance of preventive strategies cannot be overstated. The implementation of rigorous infection control measures, including the proper disinfection of hospital environments and meticulous sterilization of medical equipment, is paramount. Additionally, our study advocates for the enhanced training of healthcare personnel in aseptic techniques and the judicious use of urinary catheters to mitigate the risk of nosocomial UTIs.
In summary, our research not only delineates the scope of nosocomial UTIs within the urology department but also introduces innovative perspectives on risk factors and antibiotic resistance patterns. These insights are instrumental in formulating targeted interventions and refining existing protocols to curb the incidence of these infections, ultimately enhancing patient safety and care outcomes in hospital settings.
REFERENCES
- Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM, et al. (2005). Infectious Diseases Society of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis. 40(5):643-654.
- Hooton TM, Bradley SF, Cardenas DD, Colgan R, Geerlings SE, Rice JC, et al. (2010). Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 50(5):625-663.
- Bruyère F, Cariou G, Boiteux JP, Hoznek A, Mignard JP, Escaravage L, Bernard L, Sotto A, Soussy J, Coloby P, et le CIAFU. (2008). Méthodologie. Progrès en Urologie. 18(Suppl 1):1-3.
- Agence Française de Sécurité Sanitaire et des Produits de Santé. (2008). Recommandations de bonne pratique. Diagnostic et antibiothérapie des infections urinaires bactériennes communautaires chez l’adulte.
- Kamat US, Fereirra A, Amonkar D, Motghare DD, Kulkarni MS. (2009). Epidemiology of hospital acquired urinary tract infections in a medical college hospital in Goa. Indian J Urol. 25(1):76-80.
- Conférence de consensus co-organisée par la SPILF et AFU. Infections urinaires nosocomiales 2002.
- Dhaouadi née Gadhoum L. (2009). Infections urinaires associées aux soins. Hygiène hospitalière et lutte contre les infections associées aux soins. Les risques infectieux en milieu de soins. 2:51-60.
- Schaeffer AJ. (1986). Catheter-associated bacteriuria. Urol Clin North Am. 13(4):735-747.
- Barbut F. (2005). Les infections nosocomiales de l'adulte: bilan et Perspectives. Revue Francophone des Laboratoires. 376:27-36.
- Belmokhtar M. (2004). La surveillance des infections nosocomiales au service d'urologie. Casablanca: Université Hassan II, Faculté de Médecine et de Pharmacie.
- Fakhfakh H, Bahloul AT, Gassara M, Ben Abdallah I, Hadj Slimen H, Bahloul A, et al. (2010). Profil épidémiologique des infections urinaires nosocomiales; Service d'Urologie. CHU Habib Bourguiba, Sfax, Tunisie.
- Mouwafaq S, Adarmouch L, Amine M, Moudouni S, Bajaddoub Z, Dahmani Z, et al. (2009). Sondage urinaire et infection urinaire nosocomiale en urologie. Revue d’épidémiologie et de santé publique. 57:43.
- Lobel B, Soussy C. (2007). Les infections urinaires. Monographie en urologie. 36:3-76.
- Jeandel C, Blain H. Antibiotiques chez le sujet âgé. EMC, Médecine Akos 1999; 54-59.
- Lobel B, Patard JJ, Guille F. (2003). Infection nosocomiale en urologie. Hospital-acquired urinary tract infections in a surgical environment. Whom to treat, when and how? Annales d’Urologie. 37:339-344.
- Michelet C, Tattevin P. (2003). Infections urinaires nosocomiales chez l’immunocompétent en milieu médical: qui traiter, quand traiter et comment traiter? Méd Mal Infect. 33:457-468.
- Merle V, Germain JM, Bugel H, Nouvellon M, Lemeland JF, Czernichow P, et al. (2002). Nosocomial urinary tract infections in urologic patients: assessment of a prospective surveillance program including 10,000 patients. Eur Urol. 41(5):483-489.
- CHOUAÏB Ali M. (2007). Les infections urinaires nosocomiales en urologie. (Thèse de médecine). Fés: Université Hassan Ben Abdellah, Faculté de Médecine et de Pharmacie.
- Bruyère F, Sotto A, Escaravage L, Cariou G, et al. (2010). Recommandations de bonnes pratiques cliniques: antibioprophylaxie en chirurgie urologique, par le Comité d’infectiologie de l’association française d’urologie (CIAFU).
- Lahlou Amine I, Chegri M, L’Kassmi H. (2009). Épidémiologie et résistance aux antibiotiques des entérobactéries isolées d’infections urinaires à l’hôpital militaire Moulay-Ismail de Meknès. Antibiotiques. 11(2):90-96.
- Sekhsokh Y, Chadli M, El Hamzaoui SA. (2008). Fréquence et sensibilité aux antibiotiques des bactéries isolées dans les urines. Méd Mal Infect. 38(6):324-327.
- Lazrak MA, El Bardai G, Jaafour S, Kabbali N, Arrayhani M, Houssaini TS. (2014). Profil de l'infection urinaire nosocomiale dans un service de nephrology [Profile of nosocomial urinary tract infection in a nephrology ward]. Pan Afr Med J. 19:59.
- Butreau-Lemaire M, Botto H. (1997). Infections urinaires nosocomiales. Progrès en urologie. 7:674-682.
- 5e Conférence de consensus: Prévention des infections nosocomiales en Réanimation-Transmission croisées et nouveau-né exclus. Société française d'anesthésie et de réanimation et Société de réanimation de langue française. Janvier. 2010.