Information Links
Related Conferences
Current Issue Volume 10, Issue 1 - 2026
Treatment of Severe Maxillary Atrophy for Dental Implants in the Complete Edentulous Patient
John M Sisto D.D.S. FACD*
Former Chairman and Program Director, Oral and Maxillofacial Surgery Residency Program, Cook County Hospital, Chicago Ill, Park Ridge Center Oral, Maxillofacial and Dental Implant Surgery, 350 S. Northwest Hwy, Ste 118, Park Ridge, IL 60068, USA
*Corresponding author: John M Sisto, D.D.S. FACD, Former Chairman and Program Director, Oral and Maxillofacial Surgery Residency Program, Cook County Hospital, Chicago Ill, Park Ridge Center Oral, Maxillofacial and Dental Implant Surgery, 350 S. Northwest Hwy, Ste 118, Park Ridge, IL 60068, Phone: 847 696 4848, E-mails: [email protected]
Received Date: February 19, 2026
Published Date: March 18, 2026
Citation: Sisto JM. (2026). Treatment of Severe Maxillary Atrophy for Dental Implants in the Complete Edentulous Patient. Mathews J Dentistry. 10(1):63.
Copyrights: Sisto JM. © (2026).
ABSTRACT
The aim of this retrospective study is to investigate treatment outcomes for patients that underwent bilateral sinus lifts and vertical ridge augmentation of the maxilla prior to dental implant placement for patients who presented with a complete edentulous maxilla and severe maxillary atrophy, Cawood and Howell classification V or VI. Nine patients were treated by bone augmentation via bilateral sinus lifts and vertical ridge augmentation with a custom made titanium crib. Post-operative follow-up consisted of visual exam for evidence of infection (i.e. redness, swelling, and purulence), periapical radiographs and conebeam CT scans to evaluate bone loss and implant status. Cases studied were from 1998 -2018. Four patients had bone harvested from the anterior iliac crest and five had a tissue engineering triad approach with recombinant bone morphogenetic protein (rBMP). There were no graft failures or major complications. Healing times of the graft prior to implant placement was 5-9 months. A total of 68 implants were placed. Two patients had ten implants, three had 8 implants and four had 6 implants. The follow-up was 2 -12 years. Four implant failures occurred with three in one patient. The cumulative success rate was 94%. Bone heights remained stable with less than 1mm of bone loss on 65% of the implants. Five cases were restored with a fixed prosthesis and four with a removable. All remained in function at follow-up. Bilateral sinus lifts with vertical ridge augmentation reveals a high success rate for grafts and implants with long term stability of the implants and function of the prosthesis. This provides another viable solution for the treatment of severe maxillary atrophy in patients interested in rehabilitation to a functional occlusion through dental implant placement.
Keywords: Sinus Lift, Autogenous Bone Graft, Titanium Crib, Horizontal and Vertical Ridge Augmentation, Iliac Crest Bone Graft, Tissue Engineering.
INTRODUCTION
The management of severe maxillary atrophy in a complete edentulous patient presents a demanding surgical challenge for those patients interested in being restored to a functional occlusion through dental implant placement. The tridimensional resorptive pattern in severe maxillary atrophy leads to anterior-posterior deficiency in the sagittal plane with a class III jaw relationship (pseudoprognathism) and increased inter-arch distance as well as horizontal bone loss in the transverse dimension.
This article is the first to report a case series utilizing bilateral sinus lifts and ridge augmentation with a custom titanium crib for dental implant placement in complete edentulous severe maxillary atrophy, Cawood and Howell classifications V and VI [1]. These patients have inadequate bone in a horizontal and vertical dimension for placement of dental implants.
This technique of a titanium crib for ridge augmentation was originally described by Boyne in 1985 [2], to reconstruct the severely atrophic maxilla to increase alveolar ridge height and width for denture retention. The use of a titanium mesh acts as containment for a particulate graft and prevents collapse of the graft secondary to soft tissue tension. Boyne combined iliac crest bone with anorganic bovine particulate cancellous bone (ABCB). The bovine bone was utilized to maintain the graft volume. Ten-year follow-up on his cases showed less than 20% bone resorption under the pressure of a full denture. The technique used in this study evolved from harvesting bone from the anterior iliac crest to a tissue engineering triad approach with recombinant bone morphogentic protein (rBMP-2), allogenic bone and stem cells.
Sinus lift has proven to be a clinically dependable procedure with a low complication rate well documented in the literature. Implant survival rates in augmented sinus compare favorably to implants in the non-grafted posterior maxilla [3]. The posterior edentulous ridge in the severely atrophic V and VI classification have “egg shell” thin bone secondary to the pneumatization from the atrophy. The addition of bone to the sinus floor and ridge augmentation reconstructs both areas of atrophy resulting in increased bone density and quantity for implant placement.
Long term, well controlled randomized studies for SMA ridge augmentation are not found in the literature. One case series study by Louis et al, [4] reported on vertical ridge augmentation, included ten cases with particulate iliac crest bone and titanium mesh for the atrophic maxilla prior to dental implant placement. No sinus lifts were performed. The preoperative ridge heights in the ten cases ranged from 0 to 12 mm. The article did not stipulate Cawood-Howell classifications. A preoperative 12-mm vertical height ridge will not correlate with SMA, Cawood V or VI classification. The ten cases were not classified individually, therefore, we do not know how many were actually severe atrophy. The mean augmentation of the ridge was 14.3 mm plus or minus 1.39 mm. There were a total of three mesh exposures, but no information was given regarding the cases. A total of 68 implants were placed with an overall success rate of 97%. The article included complete mandibular grafts, partial mandibular grafts and partial maxillary grafts in addition to the complete maxilla, which is a much more difficult surgical procedure. This study does highlight a very high success rate of the implants in the grafted bone.
The progression of bone reconstruction into the area of tissue engineering has led to the use of the titanium crib technique for severe maxillary atrophy. Spagnoli and Marx [5] published a case report utilizing recombinant bone morphogenetic protein (rBMP-2), platelet-rich plasma and crushed cancellous allogenic bone with a titanium crib. The combination of these materials constitutes a tissue engineering triad. The rBMP-2 provides the signal to convert mesenchymal stem cells (MSC) into bone-forming osteoblasts. The platelet-rich plasma provides circulating stem cells from the blood and the allogenic bone a scaffold for the new bone to develop. In addition, there are MSC in bone marrow, periosteum and pericytes. The majority are found in the endosteum. BMP also induces vascular endothelial growth factor (VEGF). This couples bone production and angiogenesis which is important in long term bone maintenance. The newly formed osteoblast initiates bone formation by secreting osteoid, an unmineralized bone matrix. Osteoblasts then secrete apatite crystals and alkaline phosphatase located within special secretory vesicles called matrix vesicles. The contents of the matrix vesicles interact with collagen and other extracellular matrix proteins to create a mineral matrix. Early bone formation is referred to as woven bone. Stress and strain from dental implants lead to remodeling and mature bone. Eventually cortical and marrow components develop. The case reported showed an increased gain of ridge height of approximately 10 mm and a ridge width of 10mm. Implants were replaced six months later and all were integrated at the two years. The use of the tissue engineering triad has flourished over the last six years with more articles being published of case reports. However, to date we do not have adequate data of long-term follow-up on a large series of cases. Histomorphometric studies reveal new bone (de novo) is developed with this technique. This has led to a major paradigm shift in bone grafting.
MATERIALS AND METHODS
PATIENTS AND METHODS
This retrospective audit resulted from the treatment of nine maxillary complete edentulous patients with severe atrophy classified as Cawood and Howell V and VI. Bone reconstruction prior to dental implant placement was accomplished with bilateral sinus lifts and ridge augmentation with a custom titanium crib. The technique evolved from utilizing iliac crest autogenous grafts to a tissue engineering approach with recombinant bone morphogenetic protein (rBMP-2), mineralized cancellous allogenic bone and either platelet rich plasma(PRP) or bone marrow aspirate concentrate(BMAC) as a source of stem cells.
All nine patients in this study exhibited difficulty wearing a complete denture and were interested in a more permanent solution. None of the patients presented with significant medical comorbidities. No patients smoked. A preoperative CT scan, was performed on all patients to rule out sinus pathology or blockage of the ostial-meatal complex.
Study variables included, graft success, height of augmentation, implant success, functionality of prosthesis, marginal bone loss around implants and presence of inflammation/infection around implants.
RECONSTRUCTIVE SURGERY
All patients except two received general anesthesia with nasal endotracheal intubation, the other two were intravenous sedation and were done in two sessions, sinus lift first followed by ridge augmentation eight weeks later. The first four cases had autogenous bone harvested from the anterior iliac crest. A block of bone was removed from the medial aspect followed by curettage of cancellous bone from the marrow space. The tissue engineering triad was used in the last five cases, BMAC in three cases and PRP in two, as a source of stem cells. Antibiotic prophylaxis was provided in each case with an intravenous dose of Unasyn or in penicillin allergic patients, Clindamycin. Oral antibiotic was continued after surgery for one week. Oral hygiene was maintained with 2% chlorhexidine mouth rinse twice a day for two weeks. A maxillary denture was made available after the seventh week for appearance only and no function until the bone graft was considered healed a minimum of five months. Some patients elected not to wear the denture.
The titanium crib was custom fabricated prior to surgery. Early on this was accomplished by taking impression of the arch. The study model was waxed-up to desired ridge dimensions and then an acrylic model was made of the wax up. The titanium crib was bent to desired shape on the model. With the development of cone beam CT scan, inexpensive 3-D printed models were produced which allow direct wax up on the representative bone anatomy (Case 1: Figures 1-5). More recent technology introduced by Geistlich Pharma called Yxoss CBR, utilizes a software program for virtual augmentation to create a titanium crib based on the surgeons preference. It also computes the volume needed in graft material. The authors have only recently started to use this technique, but it does not include any patients in this study.
The initial incision extends from the right to left tuberosity, mid-crestal with vertical releasing incisions at the tuberosity. Full mucoperiosteal flaps are developed to expose the full palate and up to the on the infraorbital nerves on both sides. The periosteum around the nerves was not elevated to prevent inadvertent nerve injury. Periosteal scoring incisions were made on the labial /buccal flap to completely release the flap for a tension free closure (Case 2: Figures 1-8). Flap release is the most important aspect of the procedure to provide a tension free closure. Bilateral sinus lifts were performed in in a standard fashion with the exception of extending the window to the most anterior recess of the sinus. Bone grafting material was placed in the sinus and the crib. The crib was secured to the maxilla with two titanium screws in the midline of the palate. It’s important to ensure there is no movement of the crib in order to provide optimal conditions for graft healing. PRP is placed under the incision which aids in preventing wound dehiscence. The incision was closed in an everted fashion with 3-0 chromic horizontal mattress sutures and a running 6-0 PDS suture. Graft healing time was in the range of six to nine months and was confirmed by observation of significant consolidation on a CT scan. The tissue engineering cases were left to heal longer than autogenous grafts. Implants were left to heal originally for six months and later four months. At uncovering all implants were reversed torqued at 25ncm. Fabrication of prosthesis was started within a 3-4 of weeks of uncovering (Case 3: Figures 1-4).
RESULTS
Nine patients (6 women 3 men) underwent the procedure from 1998 -2018. The age range was 34-67 (mean 53). Follow-up was a minimum of two years and a maximum of twelve and was measured from the surgery date to the last clinical encounter.
Four cases were treated with autogenous bone and five with rBMP-2. The vertical ridge augmentation minus the sinus graft was a range of 6-11mm as measured on post op CT scans. The sinus lifts measured 12-18mm. Healing time for the iliac bone grafts was 4-6 months prior to implant placement and 6-9 months for rBMP-2. There were no cases of graft failure. Wound dehiscence occurred in two cases after a few weeks, but did not result in bone loss. Exposed mesh was handled by daily application of .12% chlorhexadine.
A total of 68 implants were placed, 14 were 3i implants and 54 Biohorizon implants. The healing time for the implants was six months in the first five cases and was changed to nine months on the last four cases. The follow up ranged from 2-12 years. A total of four implants failed for a cumulative success rate of 94%. All four failures occurred in the anterior region and on class VI ridges. One patient accounted for the loss of three implants. This patient did not have his prosthetic work completed by us for economic reasons. He returned to see us six years later with a poorly designed fixed prosthesis. We successfully restored him on his remaining five implants with a removable prosthesis retained with a milled bar with locators.
Prosthetic restoration was removable in four cases and fixed in five. Bone height remained stable with minimal bone loss (<1mm) seen in 65% of the implants (44). There was 1-3mm bone loss in 30% of the implants (20). In both groups the implants were stable. Six implants (8%), showed signs of infection (redness, swelling, purulence). The four failures showed bone loss >3mm and signs of peri-implantitis(PI). Lack of PI in the majority of implants is more than likely attributed to the fact that no cement has been used on the restorations, only screw retained prostheses. All patients communicated positive feedback with their treatment and function, other than initial complaints of length of treatment time. All prostheses were in function at the time of the patient’s last examination.
Individual Patient-level data for the case series are presented in Table1. Descriptive statistics and group comparisons by gender, ridge class and graft types are presented in Table 2. Key outcome examined at the patient level included total implant failure rate, implant failure rate per implant-year and proportions of implants with bone loss<1mm, 1mm-3mm and >3mm. Due to the relatively small sample size, outcome distributions did not conform to assumptions of normality; therefore, the Mann-Whitney U test was used as a non-parametric alternative to ANOVA for group comparisons on these outcomes.
At the implant level, significantly more implants were placed in female patients, compared with males (6 vs 3) X2 [1] = 5.88, p=.015). At the patient level, the only statistically significant difference detected was for the mean number of follow-up years between the graft types; patients in the AICBG group had significantly longer mean follow-up compared with those in the TISSENG group (10.5 years vs.5.0 years, Z=2.09, p=.037). Additionally, there were several differences between male and female patients that were not statistically significant at the p>.05 level, but could nevertheless be characterized as having trend-level significance(p<.10), including total failure (1.33 vs. 0.0, Z=1.94, p=.052), failure rate (0.17 vs. 0.0, Z=1.94, p=.052, failure rate per implant-years (0.02 vs. 0.02, Z= 1.92, p=.052) and proportion of implants with bone loss >3mm (0.17 vs. 0.0, Z=1.94, p=.052).
Table 1. Individual Patient-level data for the case series
|
AGE |
GENDER |
RIDGE-CLASS |
GRAFT TYPE |
IMPLANTS |
IMPLANT FAILURES |
PROSTHESIS |
FOLLOW-UP (years) |
|
62 |
F |
V |
TISS ENG |
10 |
FIXED |
4 |
|
|
67 |
M |
VI |
TISS ENG |
8 |
1 |
REMOVABLE |
6 |
|
63 |
M |
VI |
AICBG |
8 |
REMOVABLE |
12 |
|
|
62 |
F |
VI |
AICBG |
6 |
REMOVABLE |
11 |
|
|
38 |
F |
V |
AICGB |
10 |
FIXED |
11 |
|
|
42 |
F |
VI |
TISS ENG |
6 |
FIXED |
10 |
|
|
34 |
F |
VI |
TISS ENG |
6 |
FIXED |
2 |
|
|
62 |
M |
VI |
AICBG |
8 |
3 |
REMOVABLE |
8 |
|
64 |
F |
V |
TISS ENG |
6 |
FIXED |
3 |
AICBG – anterior iliac crest bone graft
TISS ENG- tissue engineering triad with BMP-2
Table 2. Descriptive statistics with group comparisons by gender, ridge class, and graft type
|
Total |
Patient Gender |
p |
Ridge Class |
p |
Graft Type |
p |
||||
|
Male |
Female |
V |
VI |
AICBG |
TISS ENG |
|||||
|
Patients, N (%) |
9 |
3(33.3%) |
6(66.7%) |
.317 |
3(33.3%) |
6(66.6%) |
.317 |
4(44.4%) |
5(55.5%) |
.739 |
|
Implants, N (%) |
68 |
24(35.3%) |
44(64.7%) |
.015 |
26(38.2%) |
42(61.8%) |
.052 |
32(47.1%) |
36(52.9%) |
.628 |
|
Implant failures, N (%) |
4(5.9%) |
4(100.0%) |
0(0.0%) |
.005 |
0(0.0%) |
4(100.0%) |
.105 |
3(75.0%) |
1(25.0%) |
.249 |
|
Implants per patient, mean (SD) |
7.56(1.67) |
8.00(0.0) |
7.33(2.07) |
.490 |
8.67(2.31) |
7.00(1.10) |
.270 |
8.00(1.63) |
7.20(1.79) |
.513 |
|
Implant failures per patient, mean (SD) |
0.44(1.01) |
1.33(1.53) |
0.0(0.0) |
.052 |
0.67(1.21) |
0.0(0.0) |
.377 |
0.75(1.50) |
0.20(0.45) |
.867 |
|
Per patient follow-up years, mean (SD) |
7.44(3.81) |
8.67(3.06) |
6.83(4.26) |
.517 |
6.00(4.36) |
8.17(3.71) |
.604 |
10.50(1.73) |
5.00(3.16) |
.037 |
|
Failure rate, mean (SD) |
0.06(0.13) |
0.17(0.19) |
0.0(0.0) |
.052 |
0.0(0.0) |
0.08(0.15) |
.377 |
0.94(0.19) |
0.03(0.06) |
.867 |
|
Failure rate per implant-year, mean (SD) |
0.01(0.02) |
0.02(0.02) |
0.0(0.0) |
.052 |
0.01(0.02) |
0.0(0.0) |
.377 |
0.01(0.02) |
0.004(0.009) |
.867 |
|
Per patient proportion of implants with < 1mm bone loss, mean (SD) |
0.67(0.20) |
0.54(0.19) |
0.73(0.19) |
.191 |
0.68(0.13) |
0.66(0.24) |
.794 |
0.56(0.16) |
0.75(0.20) |
.172 |
|
Per patient proportion of implants with 1mm - 3mm bone loss, mean (SD) |
0.28(0.15) |
0.29(0.07) |
0.27(0.19) |
1.000 |
0.32(0.13) |
0.26(0.17) |
.601 |
0.35(0.12) |
0.22(0.17) |
.215 |
|
Per patient proportion of implants with > 3mm bone loss, mean (SD) |
0.06(0.13) |
0.17(0.19) |
0.0(0.0) |
.052 |
0.0(0.0) |
0.08(0.15) |
.377 |
0.09(0.19) |
0.03(0.06) |
.867 |
NOTE: p-values reflect chi-square tests (for frequencies) or Mann-Whitney U tests (for means)
DISCUSSION
The current management of severe maxillary atrophy for dental implant reconstruction is accomplished through bone augmentation procedures or placement of four zygomatic implants, Quad Zygomas (QZ). The clinically accepted bone augmentation techniques in the literature are one piece only bone grafts from the iliac crest, the LeForte I interpositional bone graft from the iliac crest and the technique presented in this article.
The use of one piece only bone graft was first introduced by Branemark [6] and later by Kellar [7] and Barron and Conan [8,9]. Long term success of the implants ranged from 67 to 96% [6-10]. The success rate was based on whether a one stage or two stage approach was utilized, with the single stage approach having a higher failure rate. The long term fate of these grafts is predictable resorption based on our knowledge of the healing of nonvascular grafts,” creeping substitution”. This can adversely affect long term integration of implants as well as recession of soft tissue. With this understanding of the healing process and introduction of biologic growth factors, this technique can no longer be supported and should be considered obsolete.
The LeForte I interpositional downgraft was introduced by Sailer [11] in 1988. It is the only procedure that restores the vertical and the sagittal deficiency. The success rate of implants ranges from 76% to 97% [12-18]. Once again the use of a one stage technique over a two stage technique shows higher success with the two stage technique. Complications can include the development of the maxilla to fracture in two pieces during the down fracture of the maxilla. The length of time the segment is downfractured may influence ischemia of the maxilla and lead to long term resorption and implant failure. This can be prevented by utilizing two teams and proper storage of the harvested iliac bone. Both complications have a low occurrence rate. The ability to correct the sagittal deficiency as well as decrease the freeway space is an attractive feature of this technique and may be of benefit in a younger patient with preexisting skeletal deficiency and a long term life expectancy.
The Zygomaticus implant (ZI) was introduced by Branemark in 1988 [19]. Its use in the severely atrophic maxilla (Cawood V,VI) was first reported by Stevantd and Maleves in 2010 using four ZI implants a ”Quad Zygoma” (QZ) technique [20]. A number of publications with this procedure reveal a high success rate of over 95% [20-25]. The success of the implant is dependent on securing the apical portion in the zygoma in a bicortical fashion. There may or may not be anchorage in the alveolar ridge meaning a significant portion of the implant may be exposed to the sinus or soft tissue in the vestibule. This positioning is a function of the anatomy as discussed by Aparicio [26] and the ZAGA classification. Most patients with severe atrophy will present with ZAGA class 3 or 4, which means the implant will have exteriorized to the sinus and will be in soft tissue. This lack of bone coverage can lead to buccal/labial tissue retraction, peri-impant mucositis, peri-implantitis or oral- antral communication. All of these complications could comprise long term function and necessitate removal of the implant. Sinusitis has been reported as high as 20% of the cases but has not been implicated in implant loss. This constitutes a rather formidable list of complications irrespective of the frequency. The QZ technique is a highly desirable choice given the advanced age at which many patients present and the comorbidities that can complicate their treatment. It more expedient then other treatments and leads to quicker rehabilitation. However, its use should be tempered in cases where the anatomy is less favorable especially when the implant is not in bone in the alveolar crest area to prevent soft tissue complications. The second point is long term studies of QZ (>12 years) do not yet exist. Age expectancy of the patient should be taken into account before committing to this procedure. There is a possibility of severe complications, i.e., large O-A communications, cheek skin fistula and potential orbital trauma that need to be considered.
Our experience has demonstrated excellent results with a combination of ridge augmentation and bilateral sinus lifts. The advancements in the area of biologic growth factors have changed this technique to a less invasive treatment and therefore a more viable option. The elimination of bone harvest from the iliac crest not only decreases surgery time but eliminates another source of potential complications. Wound dehiscence of the graft site in the first two weeks could mean loss of the graft. As pointed out earlier, attention to detail in closure of the incision is paramount. This procedure will not correct the A-P deficiency and results in prosthesis with an anterior cantilever. This has not been shown to create a problem in terms of implant or bone loss. In cases where the cantilever is greater than 5mm the use of a removable appliance with a milled bar with locators or other types of attachments, may be mechanically beneficial. We believe that reconstructing both areas of atrophy, the pneumatization of the sinus and atrophy of the alveolar bone, not only increases the bone quantity but ultimately the bone density. In addition, we eliminate the increased freeway space which would lead to abnormally increased vertical height of the prosthesis. With the evolution of our technique we no longer place implants mesial to the canines and place three to four per side. This is based on the fact of a higher implant failure rate in this area. We continue to use a full arch titanium crib which allows easier augmentation as opposed to two posterior cribs.
Comparison of techniques for treatment of this problem would include the technical difficulty of the procedure, length of treatment time, complication rate, severity of the complication and the final prosthesis. This approach is less technical then the LeForte I osteotomy or the QZ. The treatment length is prolonged with grafting procedures and creates difficulty for some patients. However even with a QZ approach it may not be possible to provide immediate loading. Complication rates are similar for all the procedures but the QZ definitely can present with the most severe complications requiring a more complicated correction. The final prosthesis has more options with the grafting procedures over the QZ, which has limitations secondary to the placement which is often suboptimal. The use of conventional implants over QZ also allows for a much easier correction of implant related complications.
A limitation of this study and most bone grafting studies with SMA is a lack of case numbers. This is attributed to the rarity of severe maxillary atrophy patients presenting for treatment. Larger case studies are now being reported for QZ which has become a very popular treatment, but can present with complications that are difficult to manage.
CONCLUSION
The treatment of the complete edentulous patient with severe maxillary atrophy who is interested in rehabilitation of occlusal function with dental implants presents a significant challenge. This article presents our experience with nine patients who underwent bone augmentation with bilateral sinus lifts and ridge augmentation prior to implant placement. Graft success was 100% and implants were 94% with follow-up ranging from 2 to 12 years. The technique compares favorably to the other clinically accepted techniques for the treatment of severe maxillary atrophy. It provides reconstruction of the bone deficiency in a less technically demanding procedure. The advantage of using conventional implants versus QZ, results in diminished possibility of significant complications. The limitations of this study include retrospective design and only one center. The generalizability of this study might be compromised by limited sample size and lack of standardized follow-up times. We have demonstrated the efficacy and predictability of this approach which provides another solution in the armamentarium for the treatment of severe maxillary atrophy.
REFERENCES
- Cawood JI, Howell RA. (1988). A classification of the edentulous jaws. Int J Oral Maxillofac Surg. 17(4):232-236.
- Boyne PJ. (1992). Bone Graft and Bone Graft Substitutes. Saunders. pp. 291- 298.
- Wallace SS, Froum SJ. (2003). Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol. 8(1):328-343.
- Louis PJ, Gutta R, Said-Al-Naief N, Bartolucci AA. (2008). Reconstruction of the maxilla and mandible with particulate bone graft and titanium mesh for implant placement. J Oral Maxillofac Surg. 66(2):235-245.
- Spagnoli DB, Marx RE. (2011). Dental implants and the use of rhBMP-2. Oral Maxillofac Surg Clin North Am. 23(2):347-361.
- Breine U, Brånemark PI. (1980). Reconstruction of alveolar jaw bone. An experimental and clinical study of immediate and preformed autologous bone grafts in combination with osseointegrated implants. Scand J Plast Reconstr Surg. 14(1):23-48.
- Keller EE, Van Roekel NB, Desjardins RP, Tolman DE. (1987). Prosthetic-surgical reconstruction of the severely resorbed maxilla with iliac bone grafting and tissue-integrated prostheses. Int J Oral Maxillofac Implants. 2(3):155-165.
- Barone A, Covani U. (2007). Maxillary alveolar ridge reconstruction with nonvascularized autogenous block bone: clinical results. J Oral Maxillofac Surg. 65(10):2039-2046.
- Neyt LF, De Clercq CA, Abeloos JV, Mommaerts MY. (1997). Reconstruction of the severely resorbed maxilla with a combination of sinus augmentation, onlay bone grafting, and implants. J Oral Maxillofac Surg. 55(12):1397-401.
- Clayman L. (2006). Implant reconstruction of the bone-grafted maxilla: review of the literature and presentation of 8 cases. J Oral Maxillofac Surg. 64(4):674-682.
- Sailer HF. (1989). A new method of inserting endosseous implants in totally atrophic maxillae. J Craniomaxillofac Surg. 17(7):299-305.
- Cawood JI, Stoelinga PJ, Brouns JJ. (1994). Reconstruction of the severely resorbed (Class VI) maxilla. A two-step procedure. Int J Oral Maxillofac Surg. 23(4):219-225.
- Isaksson S, Ekfeldt A, Alberius P, Blomqvist JE. (1993). Early results from reconstruction of severely atrophic (Class VI) maxillas by immediate endosseous implants in conjunction with bone grafting and Le Fort I osteotomy. Int J Oral Maxillofac Surg. 22(3):144-148.
- Li KK, Stephens WL, Gliklich R. (1996). Reconstruction of the severely atrophic edentulous maxilla using Le Fort I osteotomy with simultaneous bone graft and implant placement. J Oral Maxillofac Surg. 54(5):542-546.
- Nyström E, Lundgren S, Gunne J, Nilson H. (1997). Interpositional bone grafting and Le Fort I osteotomy for reconstruction of the atrophic edentulous maxilla. A two-stage technique. Int J Oral Maxillofac Surg. 26(6):423-427.
- Kahnberg KE, Nilsson P, Rasmusson L. (1999). Le Fort I osteotomy with interpositional bone grafts and implants for rehabilitation of the severely resorbed maxilla: a 2-stage procedure. Int J Oral Maxillofac Implants. 14(4):571-578.
- Locher MC, Sailer HF. (1994). Results after Leforte I osteotomy in combination with titanium Implants: sinus inlay method. Oral Maxillofac Surg Clin North Am. 6(4):679-688.
- Chiapasco M, Zaniboni M, Boisco M. (2006). Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 17(Suppl 2):136-159.
- Brånemark PI, Gröndahl K, Ohrnell LO, Nilsson P, Petruson B, Svensson B, et al. (2004). Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long-term results. Scand J Plast Reconstr Surg Hand Surg. 38(2):70-85.
- Stiévenart M, Malevez C. (2010). Rehabilitation of totally atrophied maxilla by means of four zygomatic implants and fixed prosthesis: a 6-40-month follow-up. Int J Oral Maxillofac Surg. 39(4):358-363.
- Araújo RT, Sverzut AT, Trivellato AE, Sverzut CE. (2017). Retrospective Analysis of 129 Consecutive Zygomatic Implants Used to Rehabilitate Severely Resorbed Maxillae in a Two-Stage Protocol. Int J Oral Maxillofac Implants. 32(2):377-384.
- Neugarten J, Tuminelli FJ, Walter L. (2017). Two Bilateral Zygomatic Implants Placed and Immediately Loaded: A Retrospective Chart Review with Up-to-54-Month Follow-up. Int J Oral Maxillofac Implants. 32(6):1399-1403.
- Fortin Y. (2014). Placement of zygomatic implants into malar prominence of the zygoma: Clinical report of 5-13 years. Int J Oral Maxillofac Implants. 32(3):633-638.
- Davo R, Pons O. (2015). 5-year outcome of cross-arch prostheses supported by four immediately loaded zygomatic implants: A prospective case series. Eur J Oral Implantol. 8(2):169-174.
- Wang F, Monje A, Lin GH, Wu Y, Monje F, Wang HL, Davó R. (2015). Reliability of four zygomatic implant-supported prostheses for the rehabilitation of the atrophic maxilla: a systematic review. Int J Oral Maxillofac Implants. 30(2):293-298.
- Aparicio C. (2011). A proposed classification for zygomatic implant patient based on the zygoma anatomy guided approach (ZAGA): a cross-sectional survey. Eur J Oral Implantol. 4(3):269-275.
FIGURES
CASE ONE
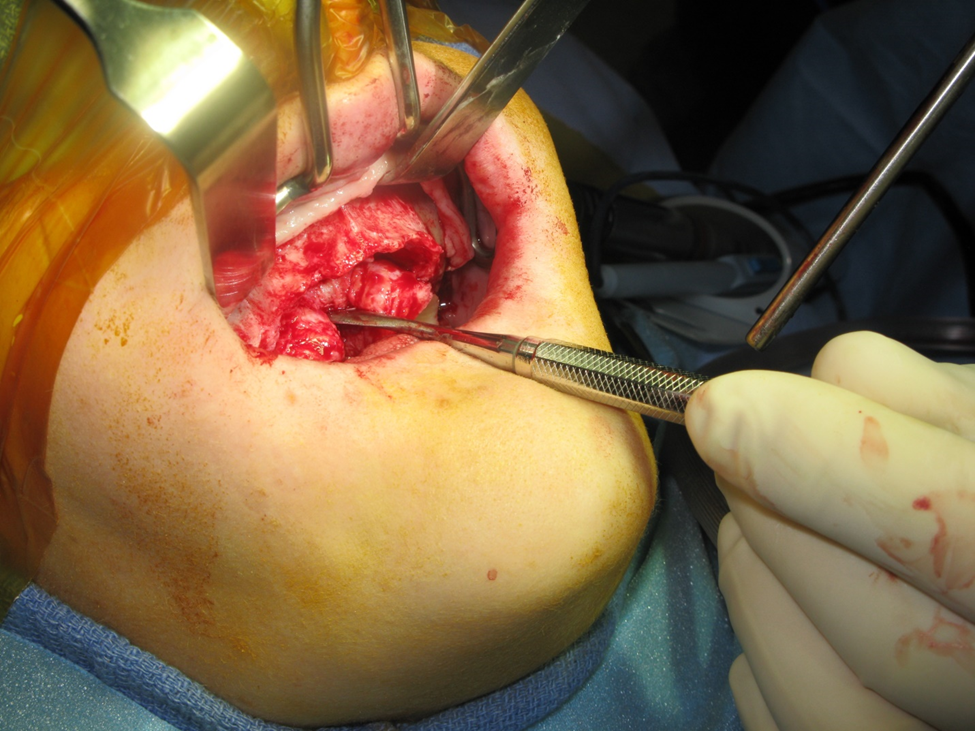
Figure 1a. Photo demonstrating Class V ridge after flap elevation. This was a 38-year-old female, who demonstrated significant atrophy in the buccal-lingual dimension. The vertical height was also insufficient for implant placement.
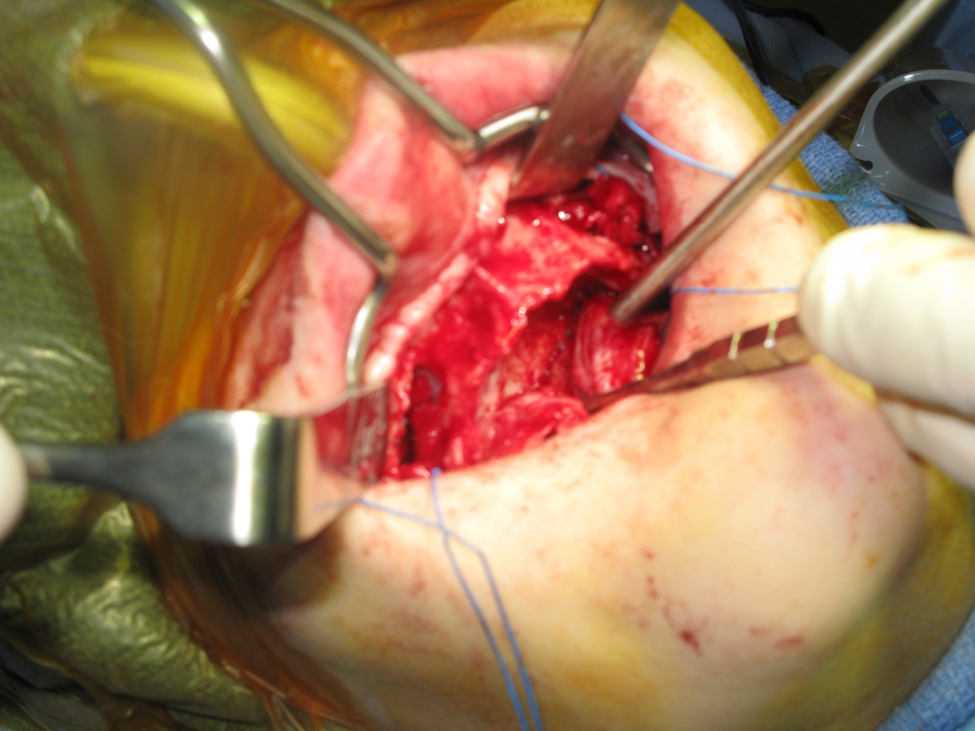
Figure 1b. Completion of bilateral sinus lift dissection. Note elevation of full palatal flap. This is necessary to relieve tension on the wound closure in addition to labial and buccal full muco-periosteal reflection as high as the infraorbital rims. The periosteum is then scored to allow flap mobilization. The sinus lifts were performed in the standard fashion.
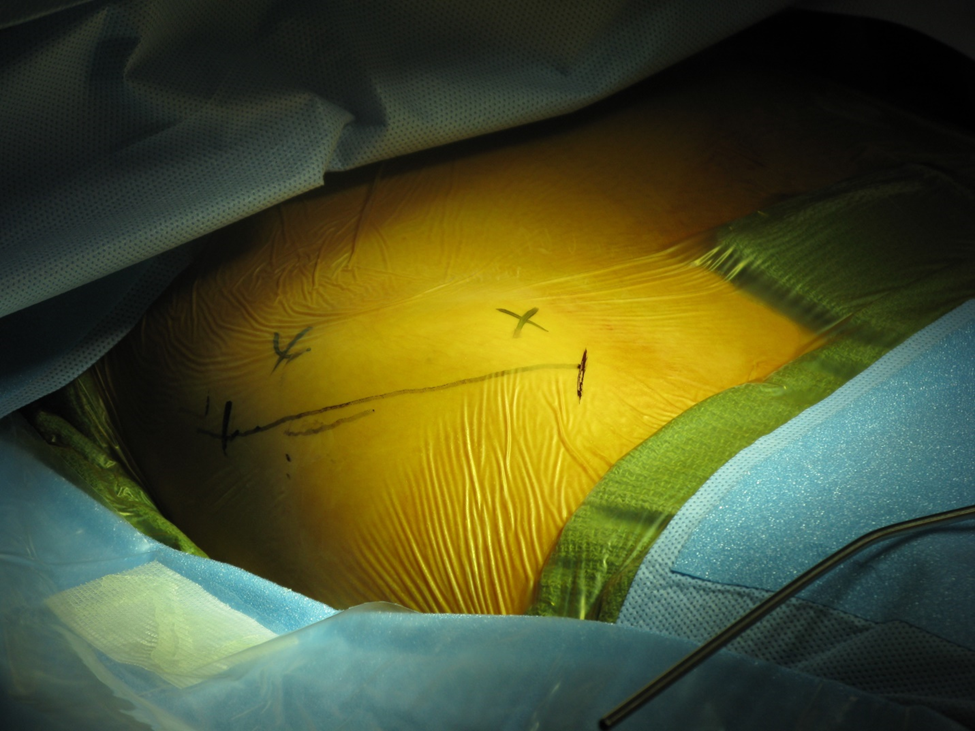
Figure 2a. Incision marking for harvesting of iliac crest bone. The incision is placed lateral to the boney prominence of the ridge. This prevents potential irritation.
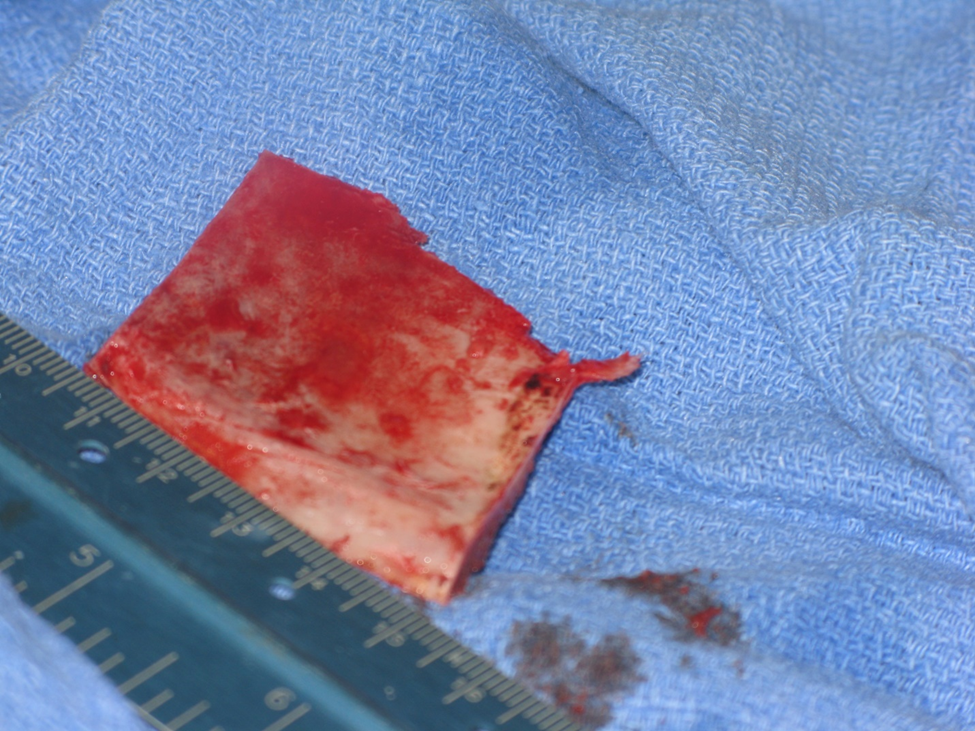
Figure 2b. Harvest of block cortical-cancellous bone. This bone will be morselized in a bone mill. In addition, cancellous bone is also removed from the site with bone curretes.
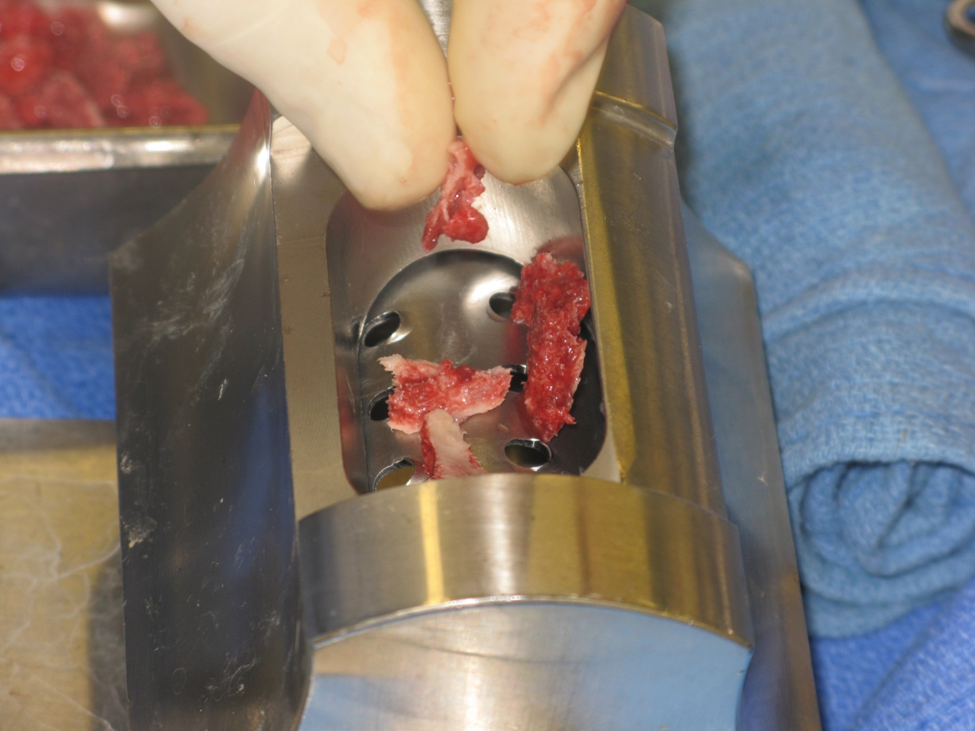
Figure 3a. Bone mill to particulate cortical –cancellous bone chips. This increases the capacity to increase the density of bone graft and thus increase the number of osteoblast cells to the site.

Figure 3b. Bone mill bone on left, bone prior to mill on right.

Figure 3c. Condensing of milled bone to increase density of viable osteoblasts.
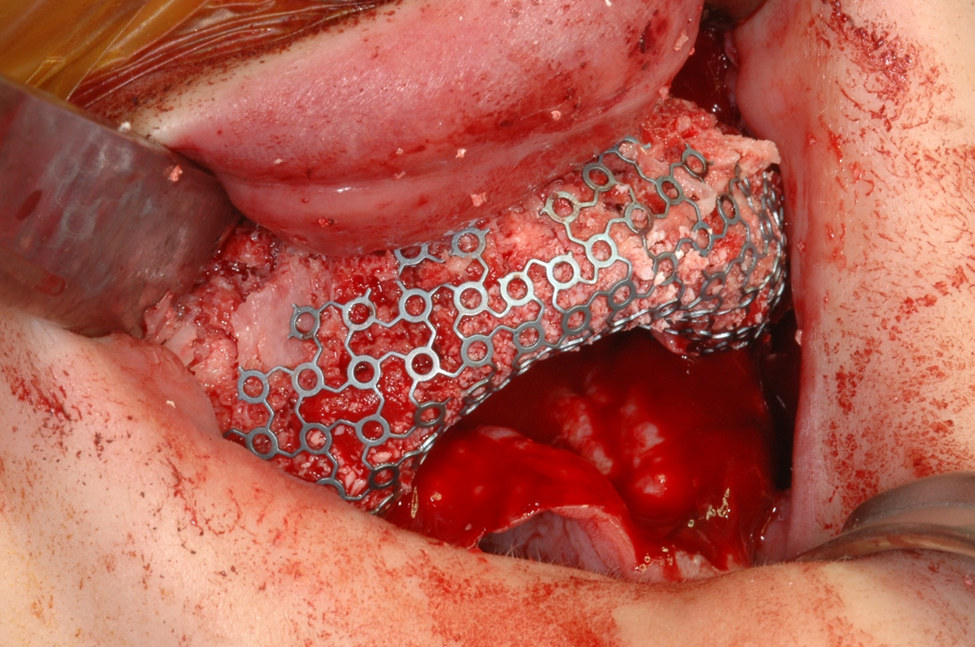
Figure 4a. Titanium tray secured to palate with two screws containing particulated cortico-canccellous bone.
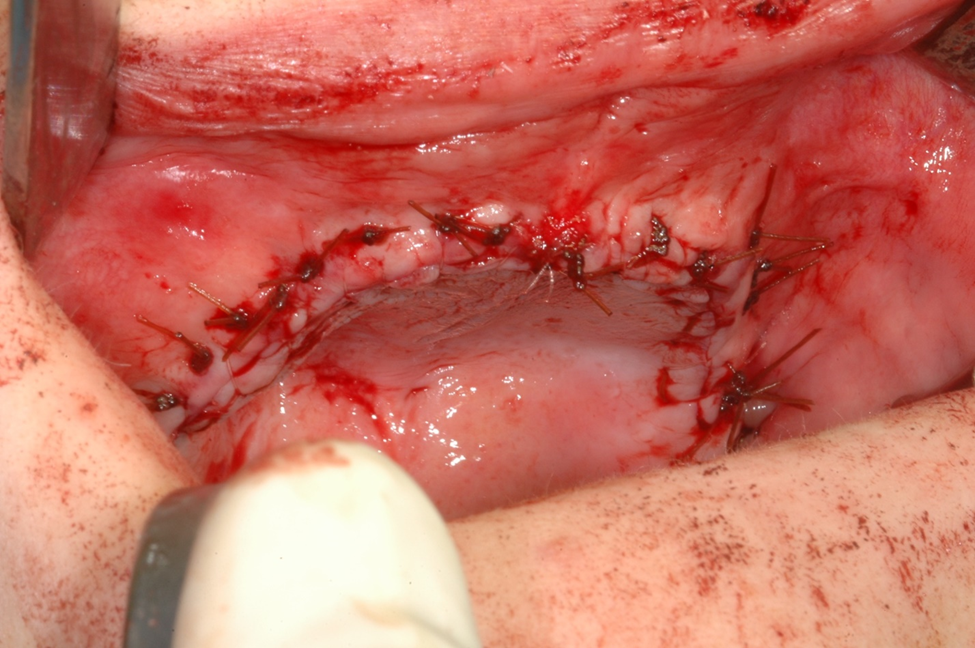
Figure 4b. A water tight tension free closure. PRP is placed under the incision to help prevent wound dehiscence. Note how wound edges are everted with horizontal mattress sutures.
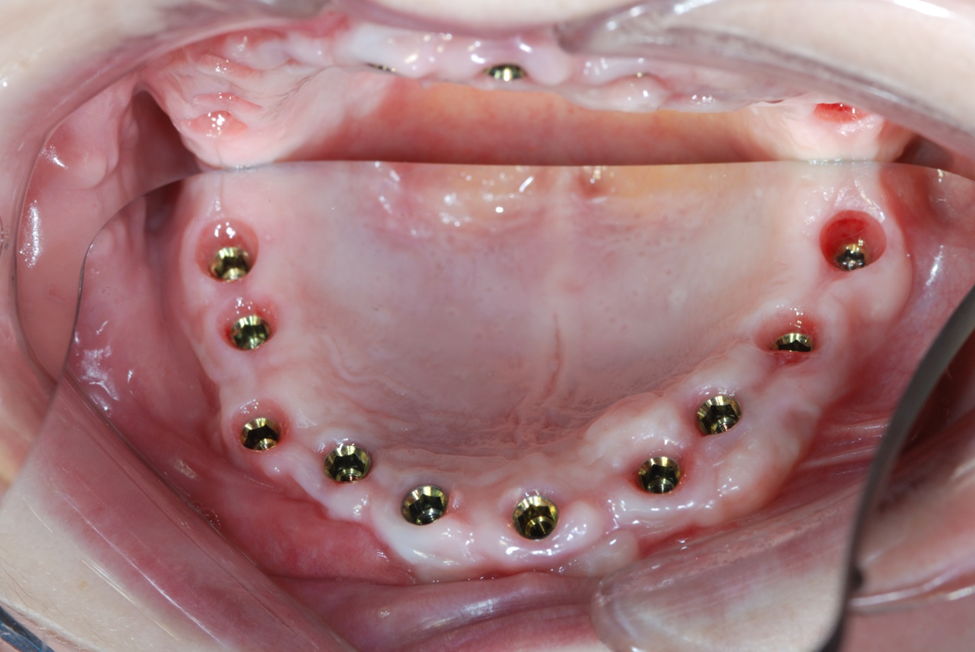
Figure 5a. Occlusal view of implants placed showing excellent keratinized tissue and good thickness.
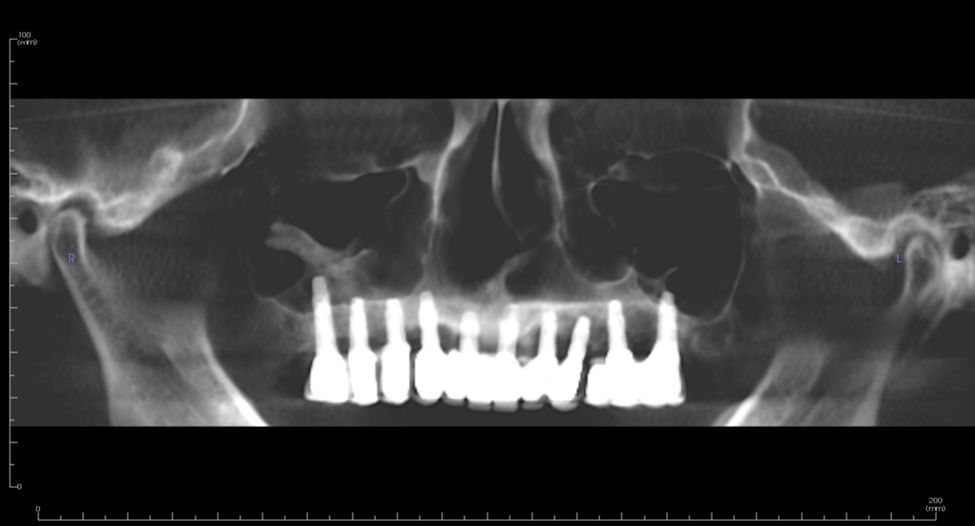
Figure 5b. 12-year follow-up panoramic radiograph revealing good bone support for implants and prosthesis. Three individual fixed bridges were placed.

Figure 5c. Occlusal view of porcelain to metal prosthesis.
CASE TWO
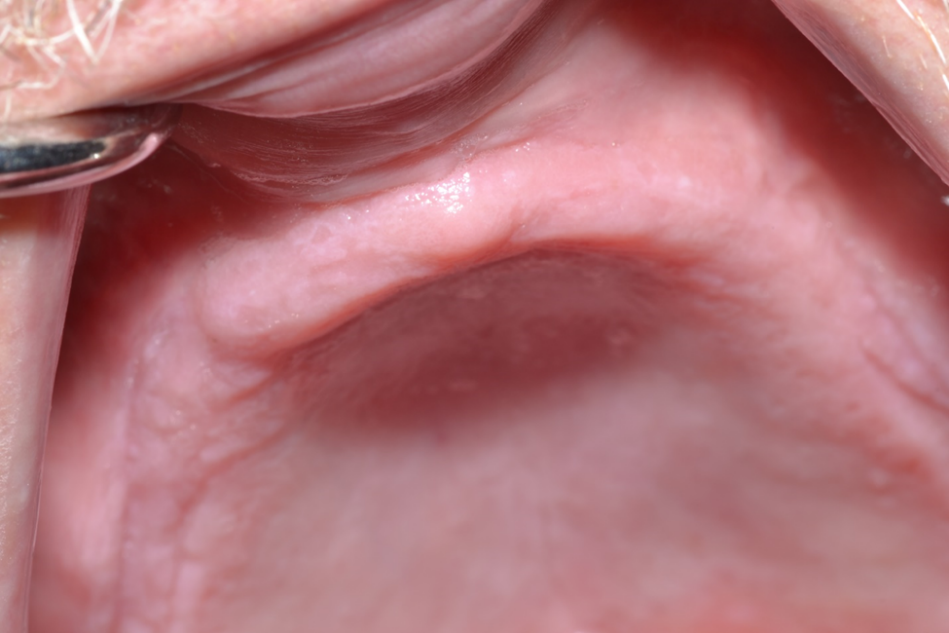
Figure 1. 67-year-old male with class VI ridge and pneumatized sinuses with 1mm residual ridge height. Bilateral sinus lifts with ridge augmentation were performed with a tissue engineering approach utilizing bone marrow aspirate concentrate (BMAC) and rBMP-2.
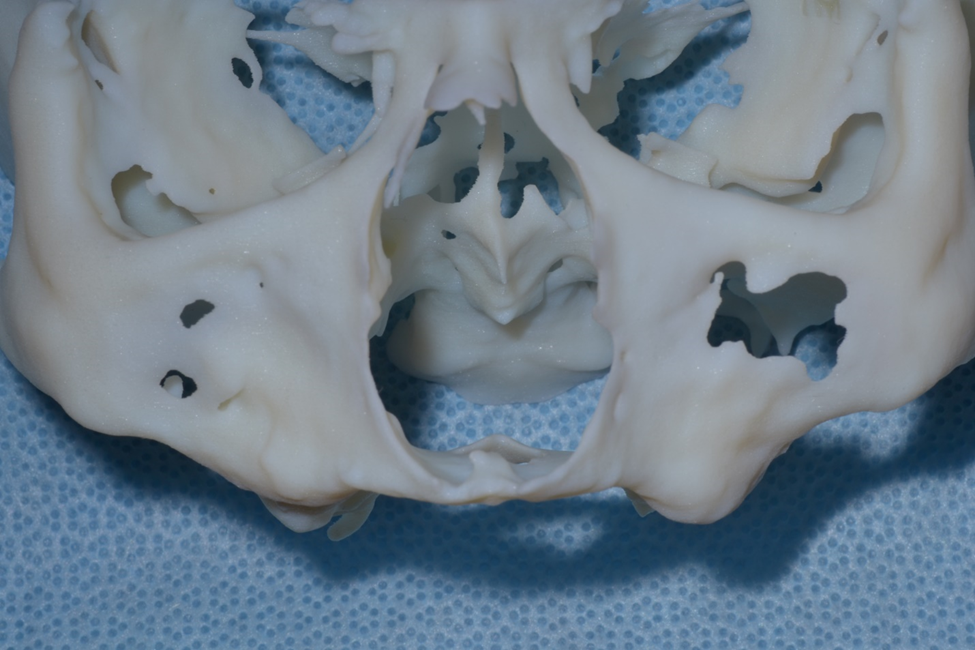
Figure 2a. 3-D model reconstructed from preoperative conebeam ct scan revealing severe atrophy down to the nasal floor.
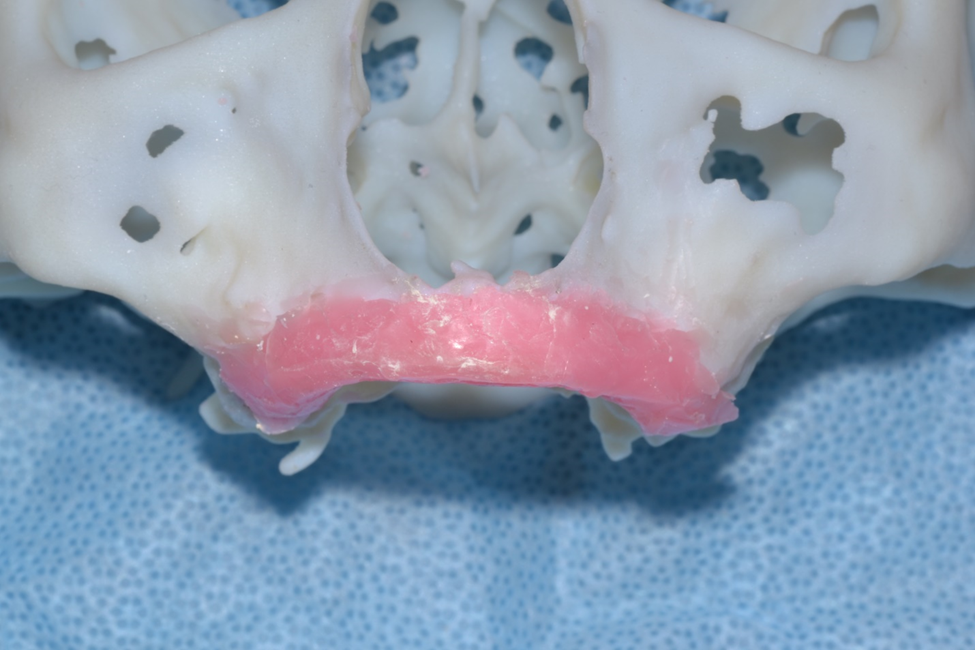
Figure 2b. Wax up of desired ridge height and width. An impression is made and poured up in acrylic for bending of titanium crib for graft containment.
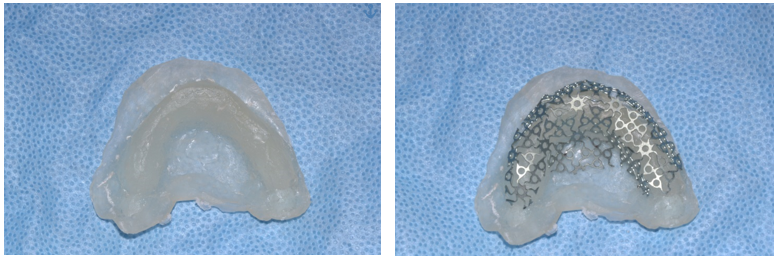
Figure 3 (a & b). Acrylic model with creation of titanium crib contoured and trimmed.
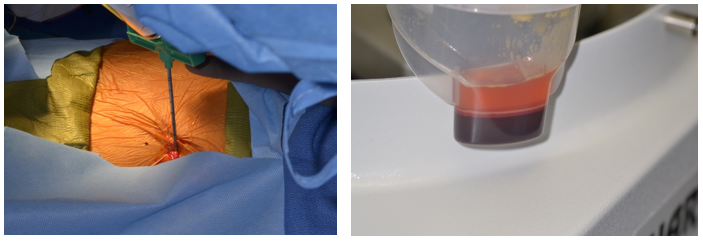
Figure 4(a & b). Aspiration of bone marrow from iliac crest. Bone marrow aspirate concentrate after it was centrifuged. The concentrated mesenchymal stem cells in the marrow are signaled by the rBMP-2 to produce osteoblasts to lay down denovo bone formation.
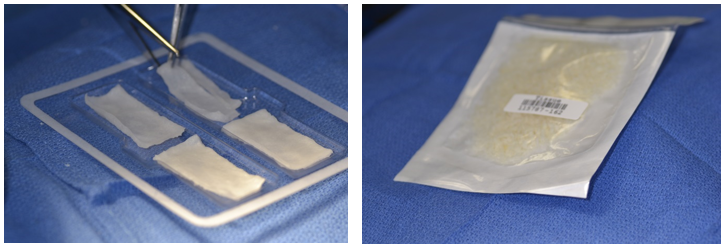
Figure 5(a & b). BMP-2 (left), the signal, applied to collagen sponge for 15 minutes to bind. Cancellous allogenic bone chips provide the scaffold for the development of denovo bone.
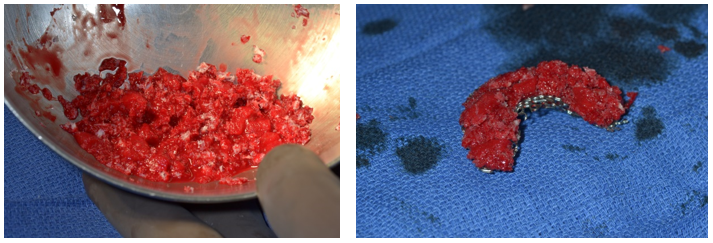
Figure 6(a & b). Mixture of rBMP-2, allograft and BMAC with placement into titanium crib. Slight overfill is necessary to ensure close contact of the grafted bone to the ridge.
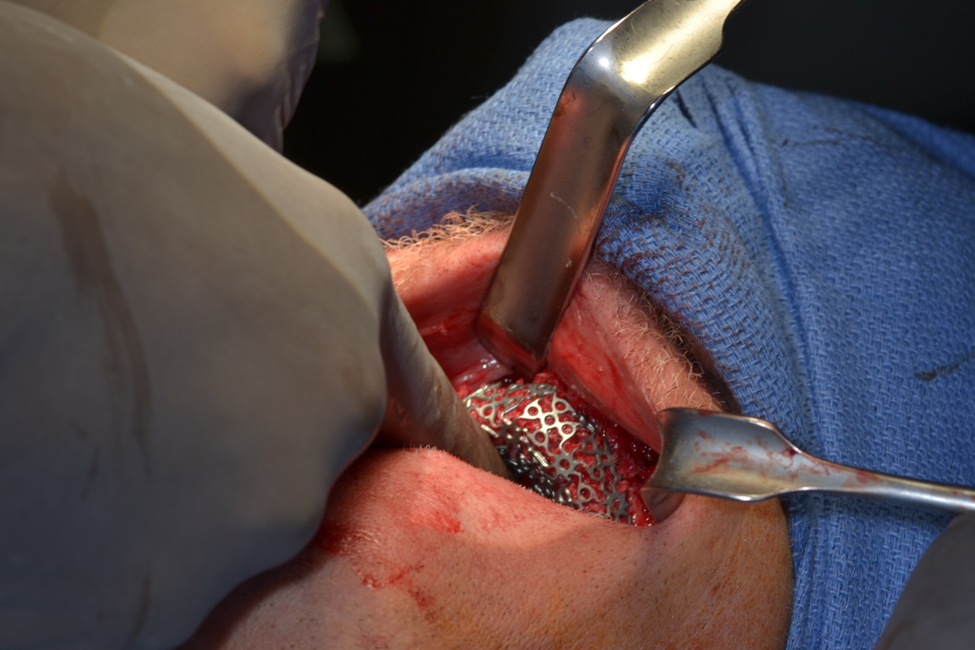
Figure 6c. Delivery of tray and graft to the maxilla. The tray is secured to the palatal bone with two 1.6mm titanium screws towards the mid-palate where the bone thickness is greatest. The incision is closed with 3-0 nylon horizontal mattress sutures in an everted fashion. The superior edges are then sutured with a running 6-0 PDS.
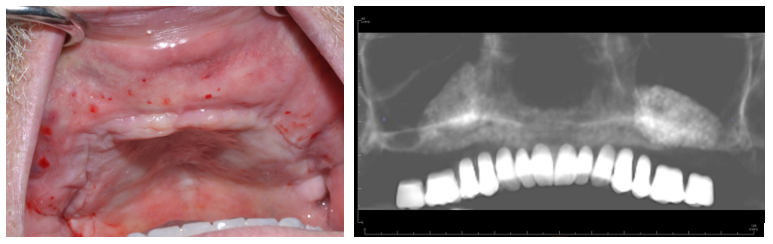
Figure 7 (a & b). Eight month follow up demonstrating graft volume in clinical photo (left). Imaging guide stent (right) to be utilized for treatment planning in Simplant software for creation of a surgical guide.
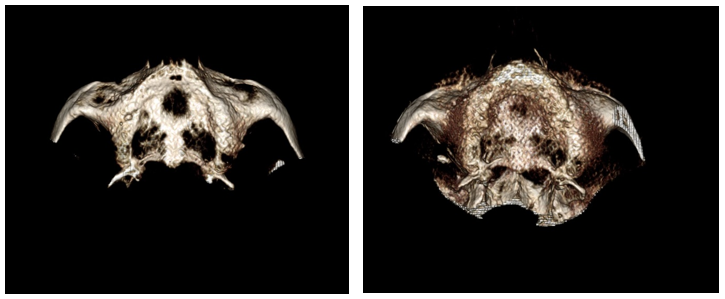
Figure 8 (a & b). Pre op 3-D reconstruction (left) and post op(right) demonstrating increased ridge thickness after grafting.
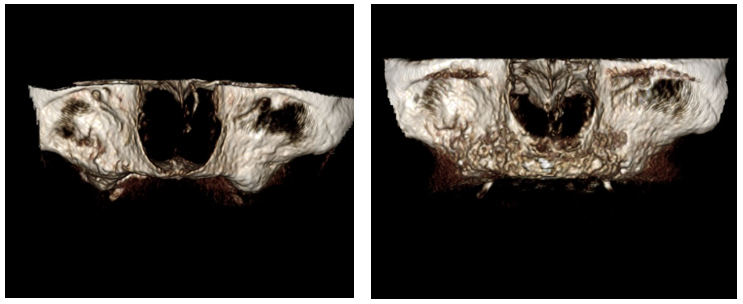
Figure 8 (c & d). Pre op (left) post op(right) demonstrating increased vertical bone height. This technique predictably produces the height planned.
CASE THREE

Figure 1. 62-year-old female with Class V ridge. Redundant flabby tissue on the ridge with little bone support and inability to wear a full denture. Patient underwent bilateral sinus lifts, vertical and horizontal ridge augmentation with a tissue engineering triad technique with PRP as the stem cell source. This patient was treated in the office.
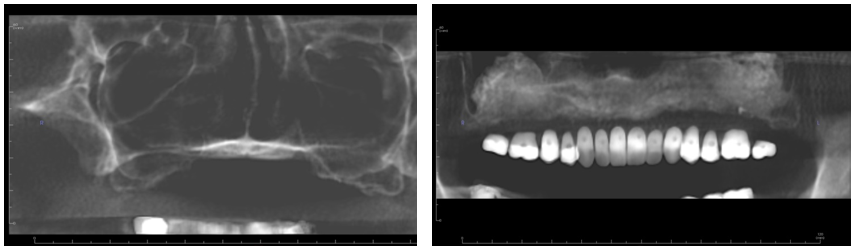
Figure 2 (a & b). Pre op panorex (left) showing highly pneumatized sinus short anterior ridge height anterior. Post op (right) panorex with imaging guide, bilateral sinus lifts and vertical and horizontal ridge augmentation.
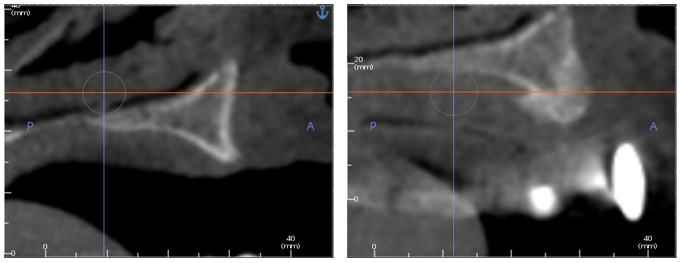
Figure 3 (a & b). Pre and post-operative sagittal cone beam views of ridge augmentation revealing excellent horizontal and vertical gains.
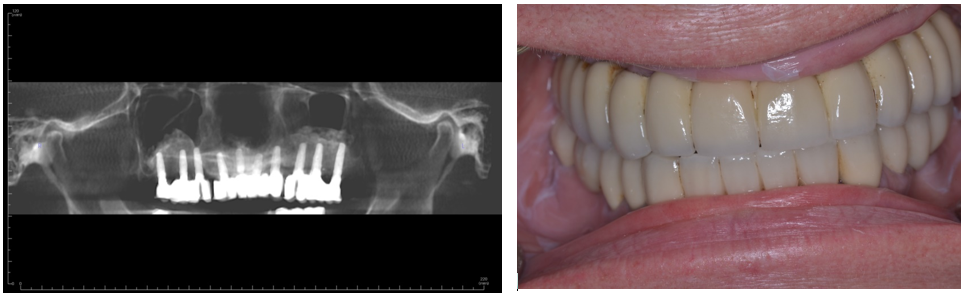
Figure 4 (a & b). Six-year follow-up demonstrating final prosthesis with three independent bridges. Good bone support has been maintained around the implants with only mild bone loss around one implant with signs inflammation. Our current philosophy would place only three to four implants per side avoiding implants in the incisor area.