Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2023
The Role of Preoperative CONUT Score in Prognosis in Patients With Radical Cystectomy
Enis Mert Yorulmaz1,*, Serkan Özcan2, Sacit Nuri Görgel2, Osman Köse2, Yiğit Akın2
1Department of Urology, Bitlis State Hospital, Bitlis, Turkey
2Department of Urology, Izmir Katip Celebi University, Izmir, Turkey
*Corresponding author: Enis Mert Yorulmaz, Department of Urology, Bitlis State Hospital, Bitlis, Turkey, ORCID-ID: 0000-0003-2109-2015; E-mail: [email protected].
Received Date: February 04, 2023
Published Date: March 20, 2023
Citation: Yorulmaz EM. (2023). The Role of Preoperative CONUT Score in Prognosis in Patients With Radical Cystectomy. Mathews J Urol Nephrol. 5(1):14.
Copyrights: Yorulmaz EM. © (2023).
ABSTRACT
Background: We evaluated the prognostic significance of the controlling nutritional status (CONUT) score, which was evaluated preoperatively, on survival. We aimed to evaluate prognostic signifcance of preoperatively assessed controlling nutritional status (CONUT) score on survival in bladder cancer (BC) patients underwent radical cystectomy (RC). Materials and Methods: The clinical and pathological data of 232 patients who underwent RC for BC between January 2006 and January 2019 at a tertiary level hospital were evaluated respectively. The data of the patients participating in the study were collected retrospectively from the patient records. All patients gave consent during hospitalization so that their information could be used. The potential prognostic value of CONUT score was assessed by using ROC curve analysis. The Kaplan–Meier method and Cox regression hazard models were used to analyzed the effect of CONUT score for patients’ disease-specifc survival (DSS) and overall survival (OAS). Results: Totally, we had 232 BC patients. Mean age was 62,98 ± 9,3 years. Only 14 (6%) of the patients were female. According to ROC analysis, optimal threshold of CONUT score for DSS was 3,50. In Kaplan– Meier analyses, the high CONUT score group showed worse progression in DSS and OAS (all parameters, p < 0.05). On Cox regression models of clinical and pathological parameters to predict DSS, age (HR 1.04, 95% CI 1.01–1.07;p=0.009), pathological T stage (HR 5.53, 95% CI 2.09–14.46;p < 0.001) CONUT score (HR 5.44, 95% CI 2.48-11.92;p<0.001); and to predict OAS, only age (HR 1.04, 95% CI 1.01–1.07; p = 0.004) were determined as independent prognostic factors. Conclusions: Preoperative elevated CONUT score could be an independent prognostic factor in BC patients underwent RC.
Keywords: Bladder Cancer, CONUT score, Urothelial Carcinoma, Predictor.
INTRODUCTION
Bladder cancer (BC) is the 7th most commonly diagnosed cancer in males, whilst it drops to 10th position when both genders are considered [1]. Epithelial tumors constitute 95% of all bladder tumors, and approximately 80–85% is transitional epithelial cell carcinomas [2]. About 75% of patients with BC present with disease confined to the mucosa (stage Ta, carcinoma in situ [CIS]) or submucosa (stage T1), while the remainder present with muscle-invasive disease and more advanced stages [3]. For the treatment of these tumors, the first treatment stage is Transurethral Bladder Tumor Resection (TUR-B), which is accepted the optimum treatment approach. Around 70% of bladder tumors recur, and 20–30% progress to a more advanced or pathological grade [4]. Because of the poor prognosis in patients with metastatic and muscle-invasive bladder cancer (MIBC), it is important to control the progression of non-muscle-invasive bladder cancer (NMIBC). For this purpose, intracavitary treatments are used today. Because of all these, early diagnosis and treatment in bladder cancer is of great importance. Various nomograms have been used to estimate the prognosis of individuals by calculating scores for a large number of variables. The two scoring models of the European Agency for Research and Treatment of Cancer (EORTC) and the Spanish Association of Urology for Oncological Treatment (CUETO) are the most commonly used individual prognostic models of bladder cancer [5]. Today, although it has valuable clinical values, it is important to focus on the tumor characteristics of the patient and not include some hematological parameters. However, more precise nomograms are needed to predict prognosis in patients with MIBC.
Nutritional status can be impaired by cancer-induced chronic inflammation. Recently, a number of studies have reported that nutritional status and systemic inflammatory response have an impact on the prognosis of cancer patients. Accordingly, several systemic inflammatory or nutritional factors have been identified for prediction of patient survival and tolerability of surgery in various types of cancer [6,7]. Controlling Nutritional Status (CONUT) score is a scoring that shows both nutritional and immune status, which is calculated from the measurement of serum albumin level, total cholesterol level, and total peripheral blood lymphocyte count of patients. The CONUT score is a scoring that has been shown to be associated with prognosis in different types of cancer. Colorectal cancers, esophageal cancer, lung cancer and pancreatic cancer are just a few of the cancer types for which this scoring is used [8-11].
In the present study, we aimed to evaluate prognostic signifcance of preoperatively assessed CONUT score on survival in BC patients underwent radical cystectomy (RC).
MATERIALS AND METHOD
This study was carried out in the Urology Clinic of the İzmir Katip Çelebi University Atatürk Training and Research Hospital with the approval of the Local Ethics Committee.
Our study was designed retrospectively. In the study, while obtaining patient information, data in a database, where informed consent was obtained from each patient, were used. The clinical and pathological data of patients who underwent RC for BC in the Urology Clinic of the İzmir Katip Çelebi University Atatürk Training and Research Hospital between January 2006 and January 2019 at a tertiary level were analyzed retrospectively. A total of 232 patients who underwent RC for BC were included in the study.
Demographic and clinical data of patients, clinicopathological parameters as predictors of disease-specifc survival (DSS) and overall survival (OAS) were examined. Patients with preoperative data on serum albumin concentration, total cholesterol concentration, and total peripheral lymphocyte count, no history of other systemic autoimmune disease or cancer, no previous neoadjuvant chemotherapy or radiotherapy, any distant metastases, and full follow-up data was included in the study. Based on the previous study, the scoring criteria of CONUT are illustrated in Table 1 [12].
Table 1. Assessment of Undernutrition Degree by CONUT [12].
|
Parameter |
Undernutrition Degree |
|||
|
Normal |
Light |
Moderate |
Severe |
|
|
Serum Albumin (g/dl) |
3.5-4.5 |
3.0-3.49 |
2.5 - 2.9 |
<2.5 |
|
Score |
0 |
2 |
4 |
6 |
|
Total Lymphocytes/ml |
> 1600 |
1200-1599 |
800-1199 |
<800 |
|
Score |
0 |
1 |
2 |
3 |
|
Cholesterol (mg/dl) |
>180 |
140-180 |
100-139 |
< 100 |
|
Score |
0 |
1 |
2 |
3 |
|
Screening Total Score |
0-1 |
2-4 |
5-8 |
9-12 |
The potential prognostic value of the CONUT score was assessed by using ROC curve analysis. The effect of the CONUT score on patient disease-specific survival (DSS) and overall survival (OAS) was analyzed by the Kaplan-Meier method and log rank test was conducted to compare these parameters. To assess the effect of patient gender age, pathological T stage, tumor grade, lymphovascular invasion, lymph node involvement and CONUT score, Cox regression hazard models were used for univariate and multivariate analyses. A 5% type-I error level was used to infer statistical significance.
RESULTS
We included 232 patients to the study. The mean age was 62,98 ± 9,3 years. Only 14 (6%) of the patients were female. The mean CONUT score was 1.28±0.40. The most common pathological T stage was T3 (31.5%) and grade was G2 (70%). Only 34.9% of the patients had lymphovascular invasion and 35.6% of all had lymph node involvement. The demographic, clinical and laboratory parameters were summarized in Table 2.
Table 2. Demographic and clinical data of patients.
|
Age (Mean±SD)
|
62.98± 9.30 years |
|
Sex(%) Female Male |
14(6) 218(94) |
|
Diabetes mellitus Negative Positive |
201(86,6) 31(13,4) |
|
Hypertension Negative Positive |
135(58,2) 97(41,8) |
|
Coronary artery disease Negative Positive |
155(66,8) 77(33,2) |
|
Smoking (Mean±SD) |
37.03±20.31 package/year |
|
Lymphovascular invasion (%) Negative Positive |
151(65.1) 81(34.9) |
|
Lymph node involvement (%) Negative Positive |
154(66,4) 78(33,6) |
|
Pathological T stage (%) T0 T1 T2 T3 T4 |
1(0.4) 49(21,1) 65(28) 73(31,5) 44(19) |
|
Tumor grade (%) G0 G1 G2 |
1(0.4) 20(8,6) 211(90) |
|
Metastasis (%) Negative Positive |
96(64.4) 53(35.6) |
|
Lymphocyte(Mean±SD) |
2,06±0,68 Lym/ml |
|
Albumin (Mean±SD) |
3,25±0,75 (g/dl) |
|
Total cholesterol (Mean±SD) |
154,61±46,46 (mg/dl) |
|
CONUT Score (Mean±SD) |
1.28±0.40 |
|
CONUT Score (%) Normal Light Moderate Severe |
36(15.5) 115(49.6) 33(14.2) 48(20.7) |
We performed an ROC analysis to determine whether the preoperative CONUT score has diagnostic value of the patient’s clinical prognosis and which cutoff value could predict this for the DSS. According to ROC analysis, optimal threshold of CONUT score for DSS was 3.50 (Figure 1;AUC:0,752 95% CI:0.681-0.823; p<0,001).
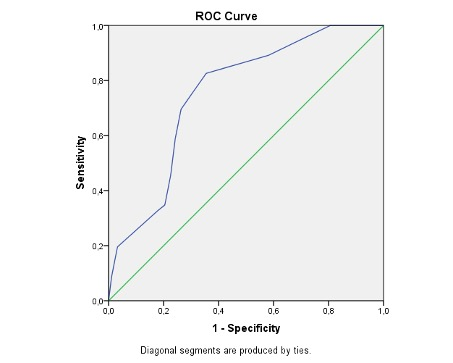
Figure 1. ROC analysis for DSS preoperative CONUT score.
In Kaplan-Meier analyses the high CONUT score group showed worse progression in DSS and OAS (p <0.001 and p=0,022, respectively) (Figure 2 and 3). 93.8% (120) of the patients with an CONUT score 3.5 or less than 3.5 and 60.7% (37) of the patients with an CONUT score greater than 3.5 are alive among DSS. 82% (105) of the patients with an CONUT score 3.5 or less than 3.5 and 71.2% (74) of the patients with an CONUT score greater than 3.5 are alive among OAS.
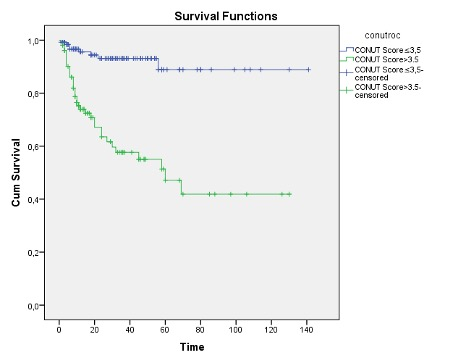
Figure 2. Kaplan Meier Analysis of Disease Spesific Survival According to CONUT Score After Cystectomy.
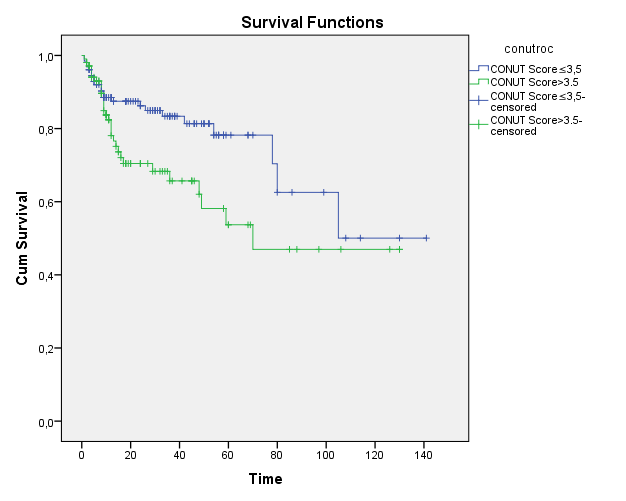
Figure 3. Kaplan Meier Analysis of Overall Survival According to CONUT Score After Cystectomy.
On univariate analyses predicting DSS age (HR:1.01, 95% CI:1.00-1.07, p=0.012), CONUT score (HR:6.82, 95% CI:3.17-14.66, p<0.001), pathological T stage (HR:9.98 95% CI:4.36-22.83, p<0.001), lymphovasculer invasion (HR:4.13, 95% CI:2.23-7.67, p<0.001), lymph node involvement (HR:4.66, 95% CI:2.18-9.94, p<0.001) and to predict OAS age (HR:1.04, 95% CI:1.01-1.07, p=0.002), pathological T stage (HR:2.27, 95% CI:1.28-4.02 p=0.004), lymphovasculer invasion (HR:2.31 95% CI:1.30-4.13, p=0.004) CONUT score (HR:1.86, 95% CI:1.08-3.21, p=0.024)) are defined as significant predictors (Table 3).
Table 3. Univariate analyses of various parameters for DSS and OAS.
|
|
DSS |
OAS |
||
|
HR(95%CI) |
P Value |
HR(95%CI) |
P Value |
|
|
Age
|
1.012(1.009-1.074) |
0,012 |
1.048(1.018-1.079) |
0.002 |
|
Sex (male vs female)
|
2.074(0.815-5.278) |
0.126 |
1.047(0.325-3.374) |
0.938 |
|
Lymphovascular invasion (negative vs.positive)
|
4.137(2.230-7.678) |
<0.001 |
2.317(1.300-4.130) |
0.004 |
|
Pathological T stage (T1-T2 vs. T3-T4)
|
9.984(4.365-22.837) |
<0.001 |
2.278(1.288-4.029) |
0.004 |
|
Tumor grade (G0-G1vs. G2)
|
2.422(0.586-10.006) |
0.222 |
1.116(0.443-2.816) |
0.815 |
|
Lymph node involvement (negative vs positive)
|
4.661(2.186-9.941) |
<0.001 |
1.721(0.980-3.023) |
0.059 |
|
CONUT Score ( <3.5 vs. 3.5 ≤)
|
6.827(3.179-14.662) |
<0.001 |
1.864(1.081-3.215) |
0.024 |
Table 4. Multivariate Cox models of clinicopathological parameters as predictors of DSS and OAS.
|
|
DSS |
OS |
||
|
HR(95%CI) |
P Value |
HR(95%CI) |
P Value |
|
|
Age |
1.043(1.011-1.076) |
0,009 |
1.045(1.014-1.077) |
0.004 |
|
Sex Male Female |
l(referent) 0.718(0.274-1.882) |
0.500 |
l(referent) 0.636(0.191-2.114) |
0.460 |
|
Lymphovascular invasion Negative Positive |
l(referent) 1.746(0.508-2.483) |
0.152 |
l(referent) 1.766(0.859-3.631) |
0.122 |
|
Pathological T stage T1-T2 T3-T4 |
l(referent) 5.535(2.091-14.468) |
0.001 |
l(referent) 1.700(0.844-3.421) |
0.137 |
|
Tumor grade G0-G1 G2 |
l(referent) 0.837(0.175-4.013) |
0.824 |
l(referent) 0.958(0.360-2.623) |
0.933 |
|
Lymph node involvement Negative Positive |
l(referent) 1.932(0.918-4.066) |
0.083 |
l(referent) 1.116(0.563-2.213) |
0.754 |
|
CONUT Score 3.50 or less than greater than 3.50 |
l(referent) 5.447(2.488-11.928) |
<0.001 |
l(referent) 1.765(0.999-3.118) |
0.050 |
In EAU Guidelines nomograms on CSS following RC have been developed and externally validated, but their wider use cannot be recommended until further data become available [13]. Today, there are searches for prognostic markers regarding the survival of patients who underwent RC for BC. The CONUT score is a value calculated from serum albumin concentration, total lymphocyte count, and total cholesterol concentration. Serum albumin level, which is an important component of serum total protein, reflects nutrition and inflammation status. Lymphocytes suppress cancer cell growth and migration, as well as promote apoptosis of cancer cells. Serum cholesterol levels have been shown to be a predictive or prognostic factor in cancer, but how it does so has not been demonstrated [14-16]. In this study revealed that DSS and OAS following RC for BC were significantly shorter in patients with high CONUT score than in those with low CONUT score. Multivariate analysis further showed that the CONUT score was an independent factor for these survival outcomes.
These findings showed us that the CONUT score is significantly associated with survival in BC patients undergoing RC. In the literature, the relationship between CONUT score and prognosis was investigated in some urological cancers as well as in different clinical branches. In a study conducted by Chen et al. involving 3529 patients, it was found that the CONUT score is a valuable preoperative index to predict the survival of patients with upper urinary tract urothelial cancer or renal cell carcinoma. undergoing nephrectomy [17]. Another study showed significantly shorter Relapse-free survival, cancer-specific survival and overall survival in the group with a high CONUT score than in the group with a low score [18]. The CONUT score was also an independent prognostic factor in prostate cancer with oligometastasis [19]. Another study showed the prognostic significance of the CONUT score in advanced urothelial carcinoma patients. The CONUT score indicates a patient's general condition from the aspect of nutritional status, and appears to be independent of performance status as a prognosticator [20].
CONCLUSIONS
In our study, the optimal threshold of the CONUT score for DSS was measured as 3.50 according to the ROC analysis. However, the higher CONUT score group showed worse progression in DSS and OAS. These results were supported by literature data. Considering that the CONUT score can be easily evaluated using blood samples taken in daily clinical practice, it may be a less invasive and effective predictor.
A high preoperative CONUT score may be an independent prognostic factor in BC patients undergoing RC.
STATEMENTS AND DECLARATIONS
All methods were carried out in accordance with the relevant guidelines and regulations in the 'DECLARATION' section of the article. Informed consent was obtained from all subjects for participation in the study.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was carried out in the urology clinic of İzmir Katip Çelebi University Atatürk Training and Research Hospital with the approval of the Local Ethics Committee. Izmir Katip Celebi University Ethics Committee Decision Number: 0140.
CONSENT FOR PUBLICATION
Informed consent was obtained from all subjects for participation in the study.
COMPETING INTERESTS
The authors declare that they have no competing interests.
FUNDING
Not applicable.
AUTHORS' CONTRIBUTIONS
EMY determined the hypothesis of the study. In addition, as the main author, he analyzed and interpreted the data of patients who underwent Radical Cystectomy for bladder cancer. SNG contributed to the evaluation of the resulting data. OK made the statistics of the study and interpreted the results. YA compared the results found in the study with the literature data. SO significantly revised the study.
ACKNOWLEDGEMENTS
Not applicable.
REFERENCES
- IARC. (2021). Cancer Today. Estimated number of new cases in 2020, worldwide, both sexes, all ages.
- Baltacı S, Bozlu M, Yıldırım A, Gökçe M, Tinay İ, Aslan G, et al. (2015). Significance of the interval between first and second transurethral resection on recurrence and progression rates in patients with high-risk non-muscle-invasive bladder cancer treated with maintenance intravesical Bacillus Calmette-Guérin. BJU Int. 116(5):721-726. DOI: 10.1111/BJU.13102.
- Compérat E, Larré S, Roupret M, Neuzillet Y, Pignot G, Quintens H, et al. (2015). Clinicopathological characteristics of urothelial bladder cancer in patients less than 40 years old. Virchows Arch. 466:589-594. DOI: 10.1007/s00428-015-1739-2.
- Babjuk M, Oosterlinck W, Sylvester R, Kaasinen E, Böhle A, Palou-Redorta J. (2008). EAU Guidelines on Non-Muscle-Invasive Urothelial Carcinoma of the Bladder. Eur Urol. 54(2):303-314. DOI: 10.1016/j.eururo.2008.04.051.
- Jobczyk M, Stawiski K, Kaszkowiak M, Rajwa P, Różański W, Soria F, et al. (2021). Deep Learning-based Recalibration of the CUETO and EORTC Prediction Tools for Recurrence and Progression of Non-muscle-invasive Bladder Cancer. Eur Urol Oncol. 5(1):109-112. DOI: 10.1016/J.EUO.2021.05.006.
- Pastore CA, Orlandi SP, González M. (2013). Association between an inflammatory-nutritional index and nutritional status in cancer patients. Nutr Hosp. 28(1):188-193. DOI: 10.3305/NH.2013.28.1.6167.
- Jagoe R, Goodship T, Gibson G. (2001). The influence of nutritional status on complications after operations for lung cancer. Ann Thorac Surg. 71(3):936-943. DOI: 10.1016/S0003-4975(00)02006-3.
- Pian G, Oh S. (2021). Comparison of nutritional and immunological scoring systems predicting prognosis in T1-2N0 colorectal cancer. Int J Colorectal Dis. 37(1):179-188. DOI: 10.1007/S00384-021-04043-0.
- Wang P, Chen X, Liu Q, Xu L, Zhang R, Liu X, et al. (2021). Application of four nutritional risk indexes in perioperative management for esophageal cancer patients. J Cancer Res Clin Oncol. 147(10):3099-3111. DOI: 10.1007/S00432-021-03585-8.
- Asakawa A, Ishibashi H, Matsuyama Y, Fujiwara T, Kobayashi M, Okubo K. (2021). Preoperative nutritional status is associated with the prognosis for lung cancer. Asian Cardiovasc Thorac Ann. 29(8):763-771. DOI: 10.1177/02184923211014002.
- Dang C, Wang M, Qin T, Qin R. (2021). Clinical importance of preoperative red-cell volume distribution width as a prognostic marker in patients undergoing radical surgery for pancreatic cancer. Surg Today. 52(3):465-474. DOI: 10.1007/S00595-021-02374-7.
- Ulíbarri JI de, González-Madroño A, Villar N de, González P, González B, Mancha A, et al. (2005). CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 20(1):38-45.
- Zaak D, Burger M, Otto W, Bastian P, Denzinger S, Stief C, et al. (2010). Predicting individual outcomes after radical cystectomy: an external validation of current nomograms. BJU Int. 106(3):342-348. DOI: 10.1111/J.1464-410X.2009.09138.X.
- McMillan D, Watson W, O’Gorman P, Preston T, Scott H, McArdle C. (2001). Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr Cancer. 39(2):210-213. DOI: 10.1207/S15327914NC392_8.
- Mantovani A, Allavena P, Sica A, Balkwill F. (2008). Cancer-related inflammation. Nature. 454(7203):436-444. DOI: 10.1038/NATURE07205.
- Kang H, Seo S, Kim W, Yun S, Lee S, Kim W, et al. (2018). Low preoperative serum cholesterol level is associated with aggressive pathologic features and poor cancer-specific survival in patients with surgically treated renal cell carcinoma. Int J Clin Oncol. 23(1):142-150. DOI: 10.1007/S10147-017-1172-4.
- Chen J, Cao D, Peng Z, Song P, Liu Z, Yang L, et al. (2021). The prognostic value of the controlling nutritional status (CONUT) score on patients undergoing nephrectomy for upper tract urothelial carcinoma or renal cell carcinoma: a systematic review and meta-analysis. Br J Nutr. DOI: 10.1017/S0007114521002889.
- Nemoto Y, Tsunenori K, Hiroki I, Toshio T, Hironiri F, Kazuhiko Y. (2021). The Controlling Nutritional Status CONUT Score in Patients With Advanced Bladder Cancer After Radical Cystectomy. In Vivo (Brooklyn). 35:999-1006. DOI: 10.21873/INVIVO.12343.
- Zhang W, Wu Y, Zhang Z, Guo Y, Wang R, Wang L, et al. (2019). Controlling Nutritional Status score: A new prognostic indicator for patients with oligometastatic prostate cancer. Curr Probl Cancer. 43(5):461-470. DOI: 10.1016/J.CURRPROBLCANCER.2019.02.001.
- Suzuki H, Ito M, Takemura K, Nakanishi Y, Kataoka M, Sakamoto K, et al. (2020). Prognostic significance of the controlling nutritional status (CONUT) score in advanced urothelial carcinoma patients. Urol Oncol. 38(3):76.e11-76.e17. DOI: 10.1016/J.UROLONC.2019.10.014.