Information Links
Related Conferences
Previous Issues Volume 7, Issue 3 - 2023
The Impact of Leucocytospermia on Semen Parameters among Sudanese Sub-fertile Men
Mohammed Ahmed Ibrahim Ahmed1,*, Mubarak Elsaeed Mustafa Elkarsany2, Nahla Ahmed Mohammed Abderahman3, Elameen Elawad Ali4
1Assistant professor of Microbiology, Faculty of Medicine, Department of Microbiology, Nile Valley University, Atbara, Sudan
2Associated professor of Microbiology, Faculty of Medicine, Department of Microbiology, Karary University, Omdurman, Sudan
3Assistant professor of Biochemistry, Faculty of Medicine, Department of Biochemistry, Nile Valley University, Atbara, Sudan
4Consultant in Obstetrics and Gynecology, River Nile State, Atbara, Sudan
*Corresponding author: Mohammed Ahmed Ibrahim Ahmed, Assistant professor of Microbiology, Nile Valley University, Faculty of Medicine, Atbara, Sudan, Tel: +2490122570655, ORCID ID: 0000-0002-0076-6730; E-mail: [email protected].
Received Date: September 21, 2023
Published Date: October 18, 2023
Citation: Ahmed MAI, et al. (2023). The Impact of Leucocytospermia on Semen Parameters among Sudanese Sub-fertile Men. Mathews J Gynecol Obstet. 7(3):29.
Copyrights: Ahmed MAI, et al. © (2023).
ABSTRACT
Background: Leucocytospermia impacts semen differently in different individuals. Semen parameter abnormalities may be influenced by underlying causes like infection and chronic diseases. Aim: To investigate leucocytospermia's and identify microorganisms in sub-fertile Sudanese males' semen and prevalence of leucocytospermia impact on sub-fertile Sudanese males’ semen characteristics. Methods: A descriptive cross-sectional hospital-based study was performed in Atbara-River Nile State, Sudan during August 2021 to August 2023 included 150 patients with sub-infertility. The participants were randomly selected and evaluated. Data was collected through direct personal interview with patients and a predesigned questionnaire was filled. Seminal fluid samples were aseptically collected from each participant after dry masturbation, followed by microscopically examination then cultured. The statistical analysis was done with the help of statistical software for social sciences SPSS 21. The characteristics of the semen, personal and demographic data were analyzed according to the standard protocols. Results: The mean age of respondents was 40.33 + 0.92 years old. 83(55.3%) of participants had leucocytospermia. There was significant difference between pus cell and occupation (p=0.005), motility (p=0.003), morphology (p=0.002), count (p=0.002), epithelial cells (p<0.0001), type of abnormalities (p=0.001) and, type of microorganism (p<0.0001). Conclusion: the study concluded that Escherichia coli, Enterococcus, and Staphylococcus were recognized as potential microorganisms and that sperm quality parameters were all adversely affected by leukocytospermia.
Keywords: Leukosytospermia, Infertility, Atbara.
INTRODUCTION
Infertility defined by the international committee for monitoring assisted reproductive technology (ICMART) and the world health organization [1] in the revised glossary as a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse, that means with natural conception process the achieved pregnancy is only 76% to 85%. It is classified as primary if no previous pregnancies have occurred and secondary infertility if it occurred after one or more pregnancies [1-3]. Infertility is a major concern for approximately 15% of reproductive age couples [4]. The inability to conceive naturally can stem from many factors including both male and female factor infertility. Approximately 10-20% of the cases of male factor infertility are being attributed to leucocytospermia [5,6], the remaining cases are due to variety of other factors, including varicocele, genetic and other systemic disease, lifestyle factors, gonadotoxin exposure, hormonal dysfunction, chromosomal disorders, testicular failure, ejaculatory disorders and obstruction [7].
The WHO defines leucocytospermia as the greater than or equal to one million leukocytes present in 1 ml of the semen [8].
Leucocytospermia is a condition in which there is an increase in the number of leukocyte in the ejaculate leucocytes play an important role in human immune system, their focus is in response to both infection and foreign materials, they are utilizing an oxygen based system to kill bacteria and other pathogens .Ongoing researches are currently investigating the clinical significance of increased leukocytes in semen and its relationship to male factor infertility [9,10]. Numerous studies support the notion that an increase of leucocytes in the semen is the detrimental to sperm parameters such as morphology and motility and impairment of sperm function [11,12].
In recent years, leucocytospermia has been shown to have adverse effect on sperm parameters through various mechanisms. It has been postulated that an increase in leucocytes in the ejaculate lead to an increase in reactive oxygen species (ROS) and subsequent oxidative stress (OS). Both ROS and OS have long been implicated in sperm dysfunction by way of lipid peroxidation [9,10,13]. Lipid peroxidation negatively influences the polyunsaturated fatty acids in the sperm cell membrane, thereby altering fluidity of the membrane and inflicting DNA damage. Unfortunately, mature sperm lack repair mechanisms after undergoing the maturation process. These cumulative effects lead to decreased sperm motility, abnormal sperm morphology and overall decrease in sperm fertilization capacity and viability [11,14].
Previous studies have demonstrated that a positive correlation between leucocytospermia and high sperm deformity index scores, a chromosomal damage, midpiece defects and tail deformities. Also infectious process leads to deterioration of spermatogenesis, impairment of sperm function, initiate a leucocyte response and/or anatomical obstruction of seminal tract. It is generally accepted that leucocytospermia may indicate infection or inflammation of the male sex glands and urogenital tract [4,5,15]. Therefore, broad spectrum antibiotics with potent antioxidants can reduce ROS produced inside cellular mitochondria as a result of inflammation by semen leucocytes. However, there is no clear consensus on the effects of each treatment or weather leucocytospermia needs to be treated or not. Furthermore, only one systematic review of the treatment of leucocytospermia is available published on 2003 and there is no adequate information on this scoop [3]. Bacterial infection of the male genital tract has been considered as one of the causes of male infertility for a long time. Different scientific reports pointed at leucocytospermia as a surrogate marker of these infections. Leucocytospermia has a substantial percentage in male factor infertility although it’s easily identified and treated. Treating these patients with suitable antibiotics and antioxidants appear to reduce temporally the leucocytes in semen and improve the fertility rates.
There are no sufficient researches or published papers in Sudan. There are very limited researches in Sudan on a small number of patients in a narrow time and limited resources.
RESEARCH METHODS
Study design, area and population: A prospective, cross-sectional, hospital based study was carried out at Modern Specialized laboratory lab Atbara, River Nile State, Sudan. One hundred fifty Sudanese patients attending to the Modern Specialized Laboratory, Atbara- having primary or secondary infertility during the study period from 2021-2023. Sudanese males at reproductive ages married for > 1 year, having primary or secondary infertility, without sexual disorders, and resident in the study area were included and patients outside the study area, married <1 year, patients diagnosed with other sexual disorders (e.g erectile dysfunction) or other causes of male infertility e.g trauma, varicocele, smoking and alcohol users, patients meet inclusion criteria and refuse to be enrolled in this study were excluded. Ethical approval was obtained from ethical committee of Nile Valley University as well as River Nile State Ministry of Health.
Sample size and selection technique: The following formula was used: N= (P x Q x Z2) / d2) + 10% (non-respondent rate). Randomized cluster design was used to sample participants. The suspected cases were numbered in regular manner. Seminal fluid samples were an aseptically collected from each participant after dry masturbation, and were examined by the microscope and cultured using specific antibiotic discs. Researchers were examined the seminal fluid of 150 sub-fertile men presenting with primary or secondary infertility. Seminal fluid were collected in a sterile, wide mouth container, by dry masturbation, after at least 48 hours of abstinence and brought immediately to the laboratory. Seminal fluid analysis was performed for 150 sub-fertile men. Color, viscosity, PH and volume were examined macroscopically, and motility was examined under the microscope within 20 minutes to one hour of collection time and was stained by10%, Giemsa stain after fixation by spirit 10-15min. Morphology and abnormal sperms were checked manually to assess the abnormalities in the head, midpiece and the tail of the sperm. This manual method was allowed the discrimination of immature sperm from white blood cells (WBCs) using Peroxidase test.
Two methods of counting WBCs in seminal fluid were employed. The number of WBCs per 100 sperm was counted on a direct smear of the semen stained by the method of Couture et-al, the number of WBCs per milliliter of fluid were determined by multiplying sperm concentration times the number of WBCs per 100 sperm and were divided by 100. The number of leukocytes were also determined by counting the number of WBCs and number of sperm 100 consecutive 400X high power fields or until at least 10 polymorphonuclear leukocytes had been counted. The ratio of the number of WBCs was divided by the number of the sperm then multiplied the number of sperm per milliliter to give the number of leukocytes per milliliter of semen.
Data collection: Data were collected by predesigned closed ended questionnaires, through direct personal interview with patients and questionnaires were filled then an informed consent was taken from each patient. Seminal analysis was performed in the lab, using the same batch and by the researcher for all patients. Gram stain was implemented for leucocytospermic patients. The sample populations were divided into two groups, sub-fertile patients with leucocytospermia and sub-fertile patients without leucocytospermia.
RESULTS
General characteristics of the study groups: 150 male couples participated in a cross-sectional study to evaluate the presence of leukocytospermia in River Nile State who were attending the Modern Special Lab in Atbara and suffering from primary or secondary infertility. The general characteristics of the participants included age, which ranged from 20 to 84 years, and different occupations, including farmers, government employees, workers, and others. Their minimum duration of liquefaction was 15 minutes and reached 130 in maximum with a mean of 34.4.The semen volume of respondents ranged from 0.4 to 7.5 ml, with a mean of 7.7 ml. The reaction of the study group ranged from 6.6 as acidic to 8.8 as alkaline, with a mean of 7.7.The counting of sperm among study couples ranged from azoospermia (0 sperm) to normospermia (90 millions), with a mean of 25.2 million (Table 1).
Table 1. General characteristics of the study groups
|
Variable |
Minimum |
Maximum |
Mean |
|
Age |
20 |
84 |
40.33 |
|
Liquefaction /minutes |
15 |
130 |
34.4 |
|
Volume |
0.4 |
7.5 |
2.92 |
|
Reaction |
6.6 |
8.8 |
7.71 |
|
Count |
0 |
90 |
25.23 |
Figure 3-1 revealed that 83 (16.0%) of the study participants had low sperm concentrations, whereas 125 (84.0%) of the individuals had normal sperm concentrations.
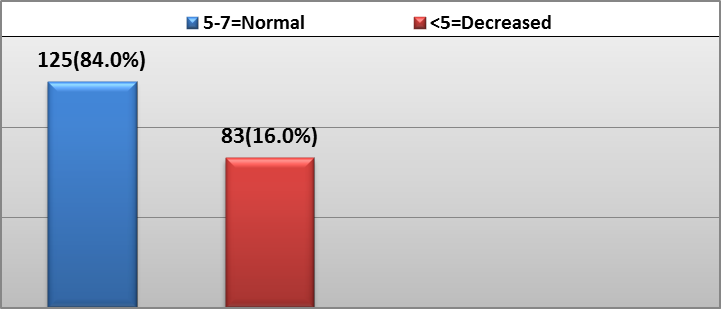
Figure 1. Study group distribution based on sperm concentrations.
Infertility persisted for more than five years in 114 (76.0%) individuals and for less than five years in 36 (24.0%), Figure 2.
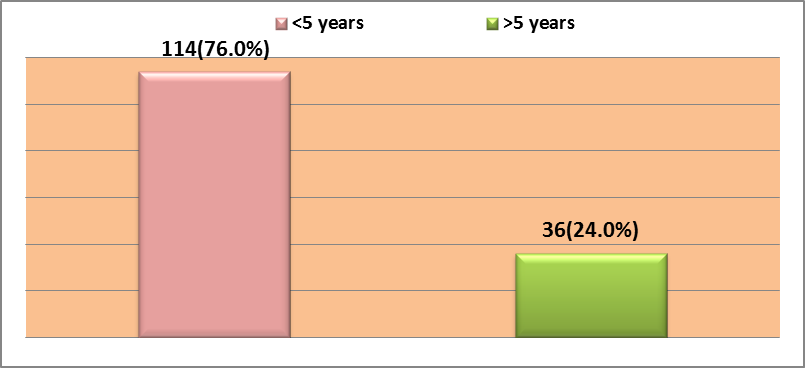
Figure 2. Distribution of research participants according to their duration of infertility.
25(1.6%) and 125 (83.3%) of the study's subjects demonstrated primary infertility, respectively Figure 3.
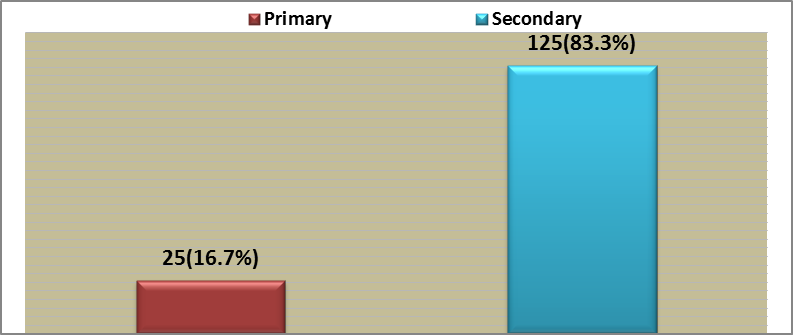
Figure 3: Distribution of research participants by infertility type.
As shown in Figure 4, 91 (60.7%) study participants had normal sperm motility, 31 (20.0%) had reduced sperm motility, and 28 (18.3%) had no sperm motility at all.
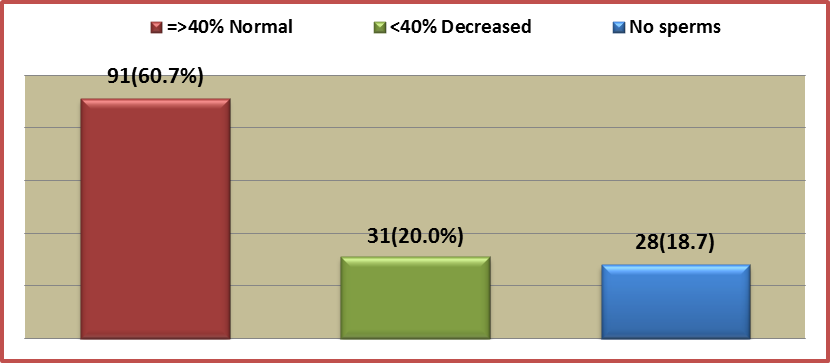
Figure 4. Distribution of the research group based on the sperm group's motility.
The distribution of sperm morphology among research participants was as follows: 94 (62.7%) had normal morphology, 29 (19.3%) had aberrant morphology and 27 (18.0%) had no sperm Figure 5.
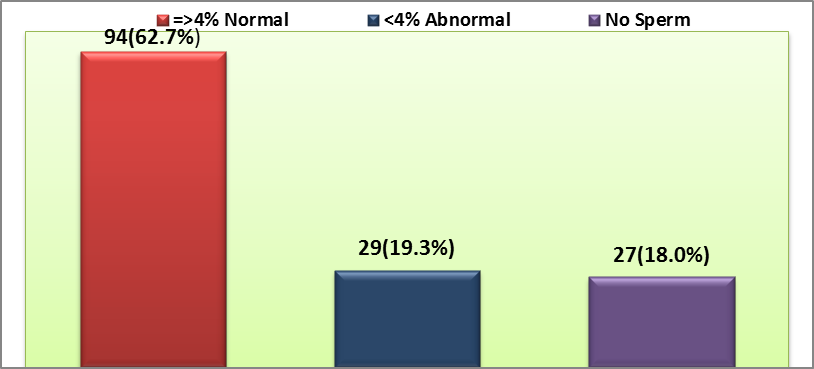
Figure 5. Distribution of the research group based on the sperm group's morphology.
In the research, 93 (62.0%) subjects exhibited normospermia, 29 (19.3%) azzospermia, and 28 (18.7%) oligo-asthenoterato-zoospermia Figure 6.
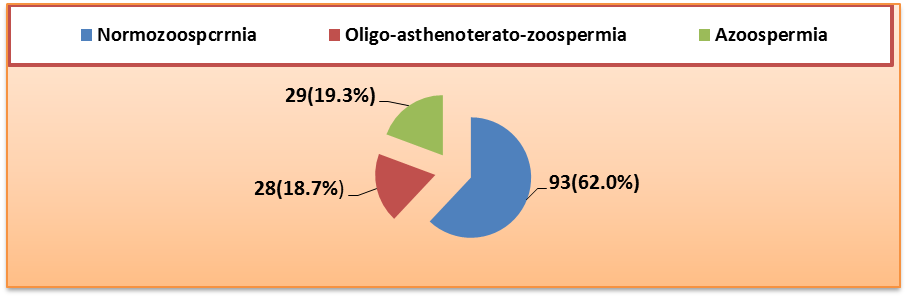
Figure 6. Distribution of study groups based on comment groups.
The following six species of bacteria were found in the research participants at the frequencies indicated by the presence of microorganisms: Figure 7. Escherichia coli was present in 23 (15.3%), Enterococcus in 14 (9.3%), Streptococcus and Staphylococcus in 2 (1.3%), and Neisseria and Corynebacterium in 1 (0.7%).
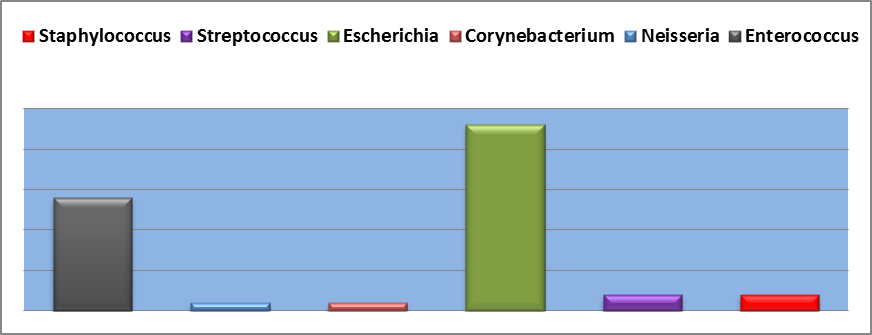
Figure 7. Distribution of study groups by species of microorganisms
Cross-tabulation of demographic and clinical data in the general study groups
The statistical significance of the correlation between two categorical variables (cross-tabulation) was evaluated using the chi-square test. P-values were considered significant when they reached (p≤0.05) or below. Table 2 shows the frequency distribution for various variables for the research participants in relation to pus cells with concept to p-value.
Table 2. Distribution of study participant’s variables according to pus cell group
|
Variable |
Group |
Pus Cells Groups |
Total |
P-value |
|
|
Normal <=5 |
Increased >5 |
||||
|
Age/Years |
20-40 |
57(48.3%) |
61(51.7%) |
118(78.7%) |
0.209 |
|
41-60 |
8(33.3%) |
16(66.7) |
24(16.0%) |
||
|
> 60 |
2(25.0%) |
6(75.0%) |
8(5.3%) |
||
|
Liquifaction/minutes |
=<60 |
60(45.5%) |
72(54.5%) |
132(88.0%) |
0.599 |
|
> 60 |
7(38.9%) |
11(61.1%) |
18(12.0%) |
||
|
Absent |
5-7=Normal |
55(43.0%) |
71(57.0%) |
126(84.0%) |
0.444 |
|
<5=Decreased |
12(50.0%) |
12(50.0%) |
24(16.0%) |
||
|
Occupation |
Farmer |
15(65.2%) |
8(34.8) |
23(15.3%) |
0.005 |
|
Government employee |
28(51.9%) |
26(48.1%) |
54(36.0%) |
||
|
Worker |
20(40.8%) |
29(59.2%) |
49(32.7%) |
||
|
Other |
4(16.7%) |
20(83.3%) |
24(16.0%) |
||
|
Infertility Duration/Years |
<5 years |
53(46.5%) |
61(53.5%) |
114(76.0%) |
0.424 |
|
>5 years |
14(31.6%) |
22(68.4%) |
36(24.0%) |
||
|
Infertility Type Group |
Primary |
12(48.0%) |
13(52.0%) |
25(16.7%) |
|
|
Secondary |
55(44.0%) |
70(56.0%) |
125(83.3%) |
||
|
Volume |
=>1.5=Normal |
55(43.7%) |
71(56.3%) |
126(84.0%) |
0.566 |
|
< 1.5= Decreased |
12(50.0%) |
12(50.0%) |
24(16.0%) |
||
|
Reaction |
<7.2 Acidic |
3(60.0%) |
2(40.0%) |
5(3.3%) |
0.217 |
|
>7.2 Alkaline |
62(43.3%) |
81(56.7%) |
143(95.3%) |
||
|
=7.2 Neutral |
2(100.0%) |
0(0.0%) |
2(1.3%) |
||
|
Motility |
=>40% Normal |
38(41.8%) |
53(58.2%) |
91(60.7%) |
0.003 |
|
<40% Decreased |
9(29.0%) |
22(71.0%) |
31(20.7%) |
||
|
No sperms |
20(71.4%) |
8(28.6%) |
28(18.7%) |
||
|
Morphology |
=>4% Normal |
41(43.6%) |
53(56.4%) |
94(62.7%) |
0.002 |
|
<4% Abnormal |
7(24.1%) |
22(75.9%) |
29(19.3%) |
||
|
No Sperm |
19(70.4%) |
8(29.6%) |
27(18.0%) |
||
|
Count/Million |
=<15=Normospermia |
40(42.6%) |
54(57.4%) |
94(62.7%) |
0.002 |
|
1-14.9=Oligospermia |
7(25.0%) |
21(75.0%) |
28(18.7%) |
||
|
Zero=Azoospermia |
20(41.4%) |
8(28.6%) |
28(18.7%) |
||
|
Red Blood Cell |
=< 2=Normal |
29(44.6%) |
36(55.4%) |
65(43.3%) |
0.991 |
|
>2=Hematospermia |
38(44.7%) |
47(55.3%) |
85(56.7%) |
||
|
Epithelial Cells |
<2 cells |
67(62.0%) |
41(38.0%) |
108(72.0%) |
<0.0001 |
|
>2 cells |
0(0.0%) |
42(100.0%) |
42(28.0%) |
||
|
Type of sperm abnormalities |
Normozoospcrrnia |
39(41.9%) |
54(58.1%) |
93(62.0%) |
0.001 |
|
Oligoasthenoteratozoospermia |
7(25.0%) |
21(75.0%) |
28(18.7%) |
||
|
Azoospermia |
21(42.4%) |
8(27.6) |
29(19.3%) |
||
|
Presence of microorganism group |
Staphylococcus |
0(0.0%) |
2(100.0%) |
2(1.3%) |
<0.0001 |
|
Streptococcus |
0(0.0%) |
2(100.0%) |
2(1.3%) |
||
|
Escherichia |
1(4.3%) |
22(95.7%) |
23(15.3%) |
||
|
Corynebacterium |
0(0.0%) |
1(100.0%) |
1(0.7%) |
||
|
Neisseria |
0(0.0%) |
1(100.0%) |
1(0.7%) |
||
|
Enterococcus |
0(0.0%) |
14(100.0%) |
14(9.3%) |
||
|
No microorganism isolated |
66(61.7%) |
41(38.3) |
107(71.3%) |
||
Table 3. Comparison of mean between Pus Cell group and other different variable
|
Variable |
Mean |
SE± |
SD |
df |
F |
Association |
p-value |
|
Age/year |
40.33 |
0.92 |
11.31 |
2 |
1.567 |
0.02 |
0.212 |
|
Liquefaction |
34.4 |
2.4 |
29.38 |
1 |
0.273 |
0.002 |
0.602 |
|
Absent |
- |
0.12 |
1.42 |
2 |
0.804 |
0.011 |
0.449 |
|
Occupation |
- |
0.08 |
0.94 |
3 |
4.604 |
0.086 |
0.004 |
|
Infertility Duration |
- |
0.04 |
0.43 |
1 |
0.634 |
0.004 |
0.427 |
|
Infertility Type |
- |
0.03 |
0.37 |
1 |
0.133 |
0.001 |
0.716 |
|
Volume |
2.92 |
0.12 |
1.47 |
1 |
0.325 |
0.002 |
0.569 |
|
Reaction |
7.71 |
0.03 |
0.36 |
2 |
1.527 |
0.02 |
0.221 |
|
Motility |
- |
0.06 |
0.79 |
2 |
6.098 |
0.077 |
0.003 |
|
Morphology |
- |
0.09 |
1.1 |
2 |
6.51 |
0.081 |
0.002 |
|
Count |
25.23 |
1.83 |
22.37 |
2 |
6.778 |
0.084 |
0.002 |
|
RBCs |
- |
0.041 |
0.497 |
1 |
0 |
<0.0001 |
0.991 |
|
Epithelial Cells |
- |
0.04 |
0.45 |
1 |
67.719 |
0.314 |
<0.0001 |
|
Comments |
- |
0.18 |
2.22 |
2 |
7.385 |
0.09 |
0.001 |
|
Types of Microorganism |
- |
0.11 |
1.31 |
6 |
9.832 |
0.292 |
<0.0001 |
DISCUSSION
Male infertility can be caused by various factors, but the negative effects of bacterial infection on male infertility remain debated [16]. Leukocytospermia is a complex and multifaceted subject with conflicting and inconsistent information of varying quality [17]. Leukocytospermia's impacts on semen parameters in Sudanese sub-fertile men were evaluated in research conducted in 2021. Semen quality and its possible significance for male infertility were also focused on. The study found substantial differences between leukocytospermia and seminal parameters in subfertile men, as well as significant effects on participant occupations, motility, morphology, epithelial cell presence, semen abnormalities, and microorganisms. Leukocytospermia was found to significantly positively correlate with a number of seminal characteristics, including age, liquefaction, absence, infertility duration, infertility type, semen volume, pH, and hematospermia.
Leukosytospermia was shown to have no significant impact on participant ages (p=0.209); however, it was present in 61 of the respondents (51.7%), ranging in age from 20 to 40 years. Age and leukosytospermia were shown to be positively correlated in the study, indicating that sperm quality and motility in subfertile Indian males may be considerably impacted by aging [18]. In a study conducted in Turkey, it was found that age significantly impacts male fertility by affecting the quantity of sperm, progressive motility rate, and normal morphology [19]. The investigation found that leukosytospermia significantly influenced various variables, indicating that male partner age should be considered a crucial factor in reproductive outcomes.
The study found a non-significant difference in seminal fluid liquefaction time (p=0.602) and a significant association with leukocytospermia (p=0.002). Another study in Egypt found higher semen hyperviscosity in leukocytospermia patients compared to non-leukocytospermia patients (p< 0.01) [20]. Leukocytospermia, a disorder that is more common in males with predicted infertility, was shown to cause prolonged liquefaction periods in men with suspected infertility, according to research by Muhamet Afşin and Ayşe Feyda Nursal [21].
The research found a non-significant difference (p=0.449) and a significant positive association between sexual abstinence days and leukocytospermia (p=0.011), aligning with Zülfü Sertkaya's report that all seminal parameters remained constant in Turkey, except for semen volume and total motile sperm count [22].
The study found that occupations were not significantly associated with leukocytospermia (p=0.086), but significantly different from other professions (p=0.004). It also revealed a link between unfavorable work behaviors and semen quality, suggesting that work habits may influence the evolution of semen parameters in semen donors. This highlights the importance of understanding the impact of occupations on semen quality [23]. Semen measurements in Wenzhou, China, were found to be influenced by personal lifestyle preferences and work-related exposures, and did not improve in line with environmental quality [24]. Both male and female fertility may be significantly impacted by the incorrect use of mercury in traditional gold mining in River Nile State and other regions of Sudan.
The study found a significant positive association between duration of infertility and leukocytospermia, and no significant difference. Shun Bai's 2021 [25] study found no correlation between leukocytospermia and infertility duration in sub fertile Chinese men [25]. The study group and case-control group showed consistent infertility durations, as reported by Rania Yahia Mohammad Shash (p=0.263 and p=0.291, respectively) [26]. The study found a significant positive connection between leukosytospermia and infertility type, with a non-significant difference (p=0.716) and a significant difference (p=0.001). Shun Bai and Rania Yahia Mohammad Shash's findings align with the current study [25,26].
The study found a non-significant difference in semen volume among research participants but a strong positive correlation with leukosytospermia (p=0.002). The study aligns with Shun Bai's research, which found that leukosytospermia significantly reduces total semen quality, including volume [25]. The study confirms that sperm parameters, particularly seminal volume, are declining in sub-fertile males in South Africa and Nigeria [27].
The study found a significant positive association between leukosytospermia and seminal pH, with no significant difference observed between participants. Shash's study revealed that the seminal pH was negatively impacted in Egyptian sub-fertile men with baceriospermia (p=1.00) [26]. Pergialiotis highlighted pH as a crucial signal in a meta-analysis of the influence of baceriospermia on semen parameters [28].
The study found a significant difference (p=0.003) and a non-significant positive association (p=0.077) in the impact of leukosytospermia on motility, a crucial semen characteristic. The study supports Rania Yahia Mohammad Shash 's findings that infertile Egyptian males with leukosytospermia exhibit poorer progressive and overall motility (p=0.001) [26]. The study on sub-fertile males in eastern Sudan found that leukosytospermia significantly impacted seminal motility (p<0.005) [29].
The study found that leukosytospermia significantly impacts sperm morphology (p=0.02).Furthermore, a non-significant positive association with leukosytospermia was concluded (p=0.081). Our results were consistent with the Egyptian study's evidence that leukoctospermia had an influence on the sperm's normal morphology (p=0.003) [26]. A significant decline in normal morphology was observed (P < 0.001) in South Africa and Nigeria [27]. A study on sub-fertile males in eastern Sudan found that leukosytospermia significantly impacted seminal morphology (p< 0.005) [29].
Liao's study revealed a significant difference in hematospermia, with a non-significant positive correlation with leukosytospermia, and supported the association between hematospermia and leukosytospermia in the current study (p=0.001) [30].
The study found a significant difference in epithelial cells among subjects (p< 0.0001), with no significant positive correlation with leukocytospermia (p=0.314), contradicting Suresh C Sikka's findings [31]. Maria A. Battistone discovered epithelial cells in sperm, hypothesizing their diverse functions could signify a broader phenomenon affecting mucosal immunity, communication, and signal processing [32].
The study involved 62% normospermia and 58.1%) leukocytospermia, with 18.7% of cases involving oligo-asthenoterato-zoospermia and 75% accompanied by leukocytospermia. The study revealed a significant difference (p=0.001) and a non-significant positive association with leukocytospermia (p=0.09). Rania Yahia Mohammad Shash highlighted bacteriospermia's negative impact on sperm quality indicators like semen volume, sperm motility, and typical sperm morphology [26].
The study revealed a significant variation (p=0.0001) and a non-significant positive association (p=0.292) with leukocytospermia, irrespective of the type of microorganism. Our study identified Escherichia coli, Enterococcus, and Staphylococcus as potential microorganisms. A study by Tingshuai Cao in China discredited Collinsella, Bifidobacterium, Blautia, and Lactobacillus as viable probiotics. The study revealed that Staphylococcus and Bacteroides are potential infectious microorganisms [33]. Staphylococcus, despite conflicting with other recognized organisms, aligns with our findings that it may be a potential bacterium for leukocytospermia. The study found that Staphylococcus aureus and Escherichia coli were the most common infectious organisms in a case-control study examining the impact of bacteriospermia on semen parameters in infertile Egyptian men [26].
CONCLUSIONS
- Leukocytospermia has detrimental effects on various sperm quality measures of sub fertile men in Atbara-River Nile State-Sudan, including sperm motility, morphology, concentration, presence of epithelial cells, type of sperm abnormalities, type of isolated microorganism, and research subjects' occupations.
- The predominant isolates found in the seminal fluid of research participants were Escherichia coli and Enterococcus.
- Azoospermia and oligo-asthenoterato-zoospermia comprised greater than thirty percent of study respondents.
- Leukocytospermia has been linked in a study to seminal bacterial contamination in sub fertile males.
RECOMMENDATIONS
- The precise detailed clinical characteristics of the patients, their demographics, and their hormone profiles were outside the purview of this study and are thus suggested for future research.
- The literature that is now accessible does not fully address several issues:
- How long will patients need to receive treatment?
- Are the results long-lasting, or May patients need more than one session of treatment?
- What is the long-term impact on pregnancy and live birth rates, even though bulk semen characteristics seem to improve with different treatments?
- Performing studies on factors that may increase the risk of developing infertility, such as diabetes, smoking, obesity, physical activity, and environmental pollution, particularly mercury, which is misused in traditional gold-mining activities in the River Nile State as well as throughout Sudan.
LIMITATIONS
The research under consideration has inherent constraints. This study may have biases due to the fact that it is a single center-based cross-sectional study. Moreover, a control group of healthy, fertile males is lacking. The study's small sample size is its last challenge, rendering it necessary to confirm the conclusions with further patients.
REFERENCES
- World Health Organization. WHO laboratory manual for the examination of human semen and sperm-cervical mucus interaction. Cambridge university press; 1999 May 13. Cambridge University Press is the publishing business of the University of Cambridge. WHO Laboratory Manual for the Examination of Human Semen and Sperm-Cervical Mucus Interaction. 4th Edition. https://www.cambridge.org/gb/knowledge/isbn/item1160163/?site_locale=en_GB
- Kassa EM, Kebede E. (2018). Time-to-pregnancy and associated factors among couples with natural planned conception in Addis Ababa, Ethiopia. Afr J Reprod Health. 22(3):33-42.
- Oates R. (2012). Evaluation of the azoospermic male. Asian J Androl. 14(1):82-87.
- Zini A, San Gabriel M, Baazeem A. (2009). Antioxidants and sperm DNA damage: a clinical perspective. J Assist Reprod Genet. 26(8):427-432.
- Aitken RJ, De Iuliis GN, Finnie JM, Hedges A, McLachlan RI. (2010). Analysis of the relationships between oxidative stress, DNA damage and sperm vitality in a patient population: development of diagnostic criteria. Hum Reprod. 25(10):2415-2426.
- Mirończuk-Chodakowska I, Witkowska AM, Zujko ME. (2018). Endogenous non-enzymatic antioxidants in the human body. Adv Med Sci. 63(1):68-78.
- Dupree JM. (2016). Insurance coverage for male infertility care in the United States. Asian J Androl. 18(3):339-341.
- Bachir BG, Jarvi K. (2014). Infectious, inflammatory, and immunologic conditions resulting in male infertility. Urol Clin North Am. 41(1):67-81.
- Gambera L, Serafini F, Morgante G, Focarelli R, De Leo V, Piomboni P. (2007). Sperm quality and pregnancy rate after COX-2 inhibitor therapy of infertile males with abacterial leukocytospermia. Hum Reprod. 22(4):1047-1051.
- Liversedge NH, Jenkins JM, Keay SD, McLaughlin EA, Al-Sufyan H, Maile LA, et al. (1996). Antibiotic treatment based on seminal cultures from asymptomatic male partners in in-vitro fertilization is unnecessary and may be detrimental. Hum Reprod. 11(6):1227-1231.
- Purvis K, Christiansen E. (1993). Infection in the male reproductive tract. Impact, diagnosis and treatment in relation to male infertility. Int J Androl. 16(1):1-3.
- Skau PA, Folstad I. (2003). Do bacterial infections cause reduced ejaculate quality? A meta-analysis of antibiotic treatment of male infertility. Behav Ecol. 14(1):40-47.
- Bonde JP. (1993). The risk of male subfecundity attributable to welding of metals. Studies of semen quality, infertility, fertility, adverse pregnancy outcome and childhood malignancy. Int J Androl. 16(Suppl 1):1-29.
- Gregoriou O, Botsis D, Papadias K, Kassanos D, Liapis A, Zourlas PA. (1989). Culture of seminal fluid in infertile men and relationship to semen evaluation. Int J Gynaecol Obstet. 28(2):149-153.
- Sanocka-Maciejewska D, Ciupińska M, Kurpisz M. (2005). Bacterial infection and semen quality. J Reprod Immunol. 67(1-2):51-56.
- Eini F, Kutenaei MA, Zareei F, Dastjerdi ZS, Shirzeyli MH, Salehi E. (2021). Effect of bacterial infection on sperm quality and DNA fragmentation in subfertile men with Leukocytospermia. BMC Mol Cell Biol. 22(1):42.
- Velez D, Ohlander S, Niederberger C. (2021). Pyospermia: background and controversies. F S Rep. 2(1):2-6.
- Asif M, Vijay AS, Maheshwari, Fyzullah S, Rani U, Swathi R, et al. (2023). Impact of chronological ageing on semen parameters in southern Indian men visiting infertility centre: A retrospective study. Asian Pac J Reprod. 12(1):10-15.
- Ulubay M, Bahaettin Ulu M, Akdeniz E. (2022). The effect of aging on semen parameters in normozoospermic men: A cross-sectional study. Int J Reprod Biomed. 20(11):955-962.
- Moubasher A, Sayed H, Mosaad E, Mahmoud A, Farag F, Taha EA. (2018). Impact of leukocytospermia on sperm dynamic motility parameters, DNA and chromosomal integrity. Cent European J Urol. 71(4):470-475.
- Afşin M, Nursal AF. (2022). The Impact of Leukocytospermia and Semen Hyperviscosity on Sperm Parameters Among Men with Suspected Infertility. Med J Bakirkoy. 18:273-277.
- Sertkaya Z, Akan S, Özdemir H, Ertaş K, Korkmaz E, Tokuç E, et al. (2022). Effect of sexual arousal on semen parameters during abstinence. Andrologia. 54(9):e14513.
- Tang F, Jiang Z, Jin M, Sheng H, Feng L, Chen J, et al. (2022). Association of occupations with decreased semen quality in eastern China: a cross-sectional study of 12 301 semen donors. BMJ Open. 12(8):e061354.
- Dai XC, Zhang MQ, Chen G, Mei K, Liu YL, Huang H, Wu ZG. (2023). Will male semen quality improve with environmental quality? Asian J Androl. 25(2):252-258.
- Bai S, Li Y, Wan Y, Guo T, Jin Q, Liu R, et al. (2021). Sexually transmitted infections and semen quality from subfertile men with and without leukocytospermia. Reprod Biol Endocrinol. 19(1):92.
- Shash RYM, Mohamed GAA, Shebl SE, Shokr M, Soliman SA. (2023). The Impact of Bacteriospermia on Semen Parameters Among Infertile Egyptian Men: A Case-Control Study. Am J Mens Health. 17(3):15579883231181861.
- Akang EN, Opuwari CS, Enyioma-Alozie S, et al. (2023). Trends in semen parameters of infertile men in South Africa and Nigeria. Sci Rep. 13(1):6819.
- Pergialiotis V, Karampetsou N, Perrea DN, Konstantopoulos P, Daskalakis G. (2018). The Impact of Bacteriospermia on Semen Parameters: A Meta-Analysis. J Family Reprod Health. 12(2):73-83.
- Abdel-Aziz DS, Ahmed MAI, Elghazali EEO, Ahmed ASAA, Ahmed TBM, et al. (2021). Impact of Leucocytospermia on Semen Parameters among Sudanese Sub-Fertile Men Port Sudan-2019. J Dermatol Res Rev Rep. 2(2):1-5.
- Liao LG, Li YF, Zhang Y, Li K, Zhu T, Li BJ, et al. (2019). Etiology of 305 cases of refractory hematospermia and therapeutic options by emerging endoscopic technology. Sci Rep. 9(1):5018.
- Sikka SC, Hellstrom WJ. (2016). Current updates on laboratory techniques for the diagnosis of male reproductive failure. Asian J Androl. 18(3):392-401.
- Battistone MA, Spallanzani RG, Mendelsohn AC, Capen D, Nair AV, et al. (2019). Novel role of proton-secreting epithelial cells in sperm maturation and mucosal immunity. J Cell Sci. 133(5):jcs233239.
- Cao T, Wang S, Pan Y, Guo F, Wu B, Zhang Y, et al. (2023). Characterization of the semen, gut, and urine microbiota in patients with different semen abnormalities. Front Microbiol. 14:1182320.