Information Links
Related Conferences
Previous Issues Volume 7, Issue 3 - 2023
The Effectiveness of Guided Implant Placement and Bone Regeneration in the Aesthetic Area. Implant Therapy–A Case Report
Louati Moataz1,*,Bouslama Afif2, Gargouri Rania1, Oualha Lamia3 and Douki Nabiha3
1Department of Dentistry, University Hospital, Sahloul, Tunisia Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia. Research Laboratory LR12ES11, University of Monastir, Tunisia
2Associate Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia. Research Laboratory LR12ES11, University of Monastir, Tunisia
3Professor, Department Head of Dentistry, University Hospital, Sahloul, Tunisia Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia. Research Laboratory LR12ES11, University of Monastir, Tunisia
*Corresponding Author: Dr. MoatazLouati, DDS, Department of Dentistry, university hospital, Sahloul, Tunisia Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia. Research Laboratory LR12ES11, University of Monastir, Tunisia; Tel: +21623406096; Email: [email protected]
Received Date: August 12, 2023
Publication Date: October 24, 2023
Citation: Moataz L, et al. (2023). The Effectiveness of Guided Implant Placement and Bone Regeneration in the Aesthetic Area. Implant Therapy–A Case Report. Mathews J Dentistry. 7(3):38.
Copyright: Moataz L, et al. © (2023)
INTRODUCTION
The anterior maxilla is the most likely site to experience dimensional changes as a result of tooth loss due to trauma, periodontal disease, caries, etc. This bone atrophy of the edentulous ridge can present both functional and aesthetic challenges, and often requires preoperative or intraoperative bone augmentation surgery [1].
A wide range of bone augmentation materials have been proposed in the literature, including autogenous bone, xenografts, allografts, and alloplastic materials. However, autogenous bone is still considered the gold standard for bone augmentation [2].
The international consensus emphasizes that the aesthetic and functional success of dental implants depends essentially on the three-dimensional positioning of the implant, regardless of the implant system, bone augmentation materials, or surgical technique used [3].
Digital implantology, particularly guided implant surgery, offers numerous benefits. It simplifies surgical procedures, ensuring precise three-dimensional implant placement and optimizing clinical outcomes. Digital planning allows for accurate diagnosis of the implant site and virtual visualization of the final restoration. It also reduces surgical time and lowers complication rates. These advantages contribute to the steady growth and increasing interest in digital implantology [4].
Guided implantology can generally be classified into dynamic and static surgery. Dynamic surgery involves the use of a computer-assisted navigation system to allow for real-time implant placement. The main advantage of dynamic design is the ability to adjust the planned implant positioning intraoperatively. Although guided surgeries are gaining in popularity, static guides remain the most commonly used method to this day [5].
CASE REPORT CASE 1
A 24-year-old female, nonsmoker, with no significant medical history, allergies, or medications, consulted with a chief complaint of a missing left maxillary central incisor since 8 months. She was concerned about the aesthetic appearance of her smile and wanted to restore the missing tooth.
The anamnesis reveals a history of trauma; fell on the ground with a frontal hit to the face (figure 1).
-The patient's smile was asymmetrical due to the missing tooth. The adjacent teeth were healthy.
-At the periodontal examination, we observed a thick and scalloped periodontal phenotype. There was a nonharmonious mucogingival line (figure 2) and a slight gingival inflammation localized at the papilla and at the level of the collars of the 10 and 11.
-The occlusal view reveals a vestibular depression showing the lack of vestibulo-lingual thickness of the ridge. (Figure 3).
-The CBCT radiographic examination showed a 2 mm thick alveolar ridge (figure 4).
-The patient was informed about the risks and benefits of dental implant surgery. He elected to proceed with the procedure.
•The treatment plan includes:
• Initial periodontal therapy
• Guided bone regeneration
• Guided implant surgery
SURGICAL TECHNIQUE
The technique presented is an onlay bone graft with the use of corticopendulous allogeneic bone blocks to compensate for the horizontal bone defect and to avoid a second surgical site, followed by a deferred guided implantation and immediate temporization to achieve ideal placement of the implant in the three dimensions of space.
After a local para-apical and a palatal anesthesia (lidocaine), the incisions were performed. The incision pattern includes an intrasulcular incision extending two teeth on either side of the edentulous area with two vertical releasing incisions. (Figure 5)
The occlusal view shows a very thin alveolar ridge with an important vestibular depression. (Figure 6) After preparation of the recipient site and removal of mucosal or connective fibers, cortical perforations are made in the recipient bone site to promote sufficient vascular supply for the bone graft from the cancellous bone (Figure 7).

Figure 1: baseline-clinical situation.
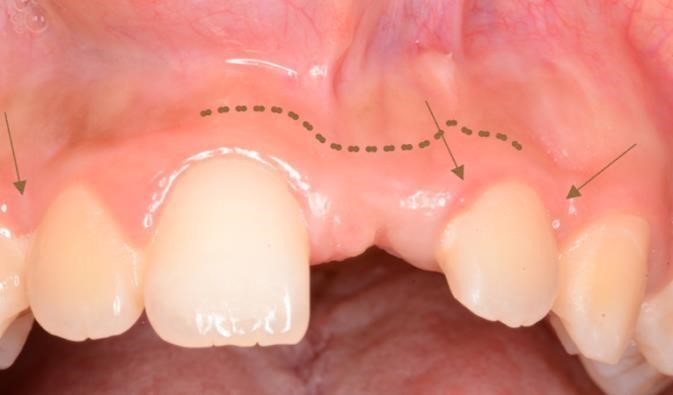
Figure 2: baseline-clinical situation.
Localized gingival inflammation
muccogingival line

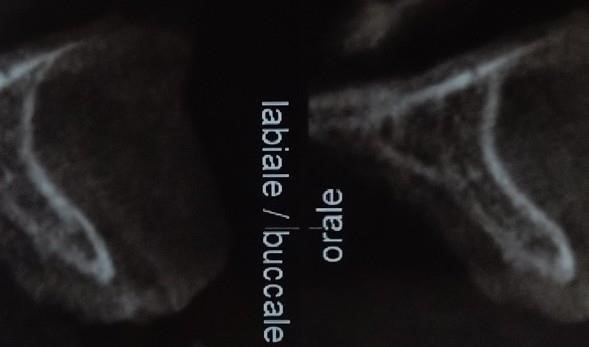
Figure 3: baseline- occlusal view Figure 4: baseline- radiographic situation ( CBCT)
The allogénic, cortico-cancellous block graft was prepared and adjusted to closely match the morphology of the recipient site and fixed with the using of two osteosynthesis screws (1.2 mm diameter and 9 mm length). The sharp edges of the block were smoothed with a diamond bur to avoid damaging the flap during sutures.
The remaining bone block was particulated and condensed at the space between the grafted bone block and the recipient site (Figure 8).
An absorbable collagen membrane was adjusted and applied to the surgical site (Figure 9).
The flap was then released from all muscle tension and sutured with Vicryl 5/0 absorbable suture (Figure 10).
After one month of healing, satisfactory healing can be seen (Figure 11) and the disappearance of the vestibular depression, initially present pre-operatively (Figure 12)
An Intraoral scanner for soft tissue was performed to obtain the STL files. (Figure 13) also CBCT was performed after the bone surgery to obtain the DICOM files (Figure 14).
Digital matching of DICOM and STL files allows for implant planning taking into consideration the length of the implant, the width of the implant and the 3D orientation of the implant (Figure 15).
After the planification, the adapted surgical guide is created. (Figure 16) and a guided implant surgery with a static navigation was realized (figure 16). After 2 months the Temporary crown was readapted (Figure 17-26
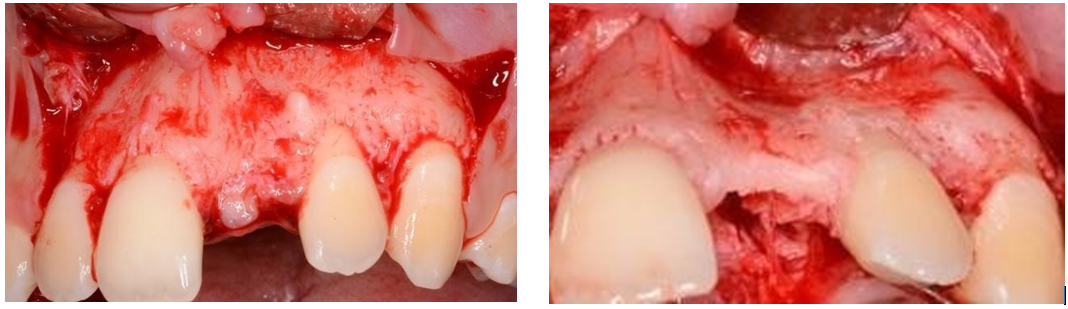
Figure 5: Full-thickness mucoperiosteal flap elevation Figure 6: occlusal view( horizontal alveolar bone loss )
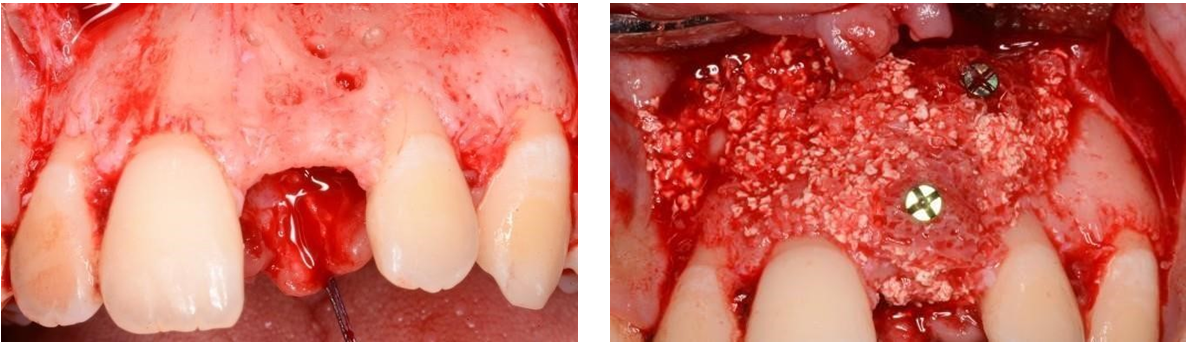
Figure 7: cortical perforations Figure 8: block graft fixation + Bone Chip
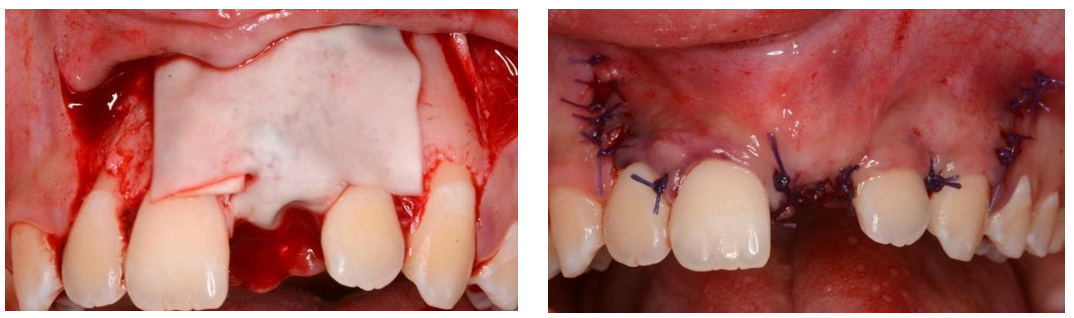
Figure 9: Double-layer collagen membrane adaptation. Figure 10: sutures
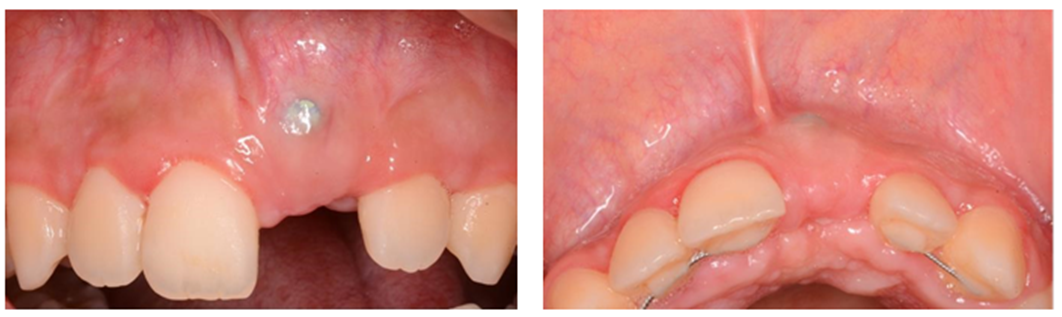
Figure 11: Clinical situation: one month of healing Figure 12: post-operative occlusal view.
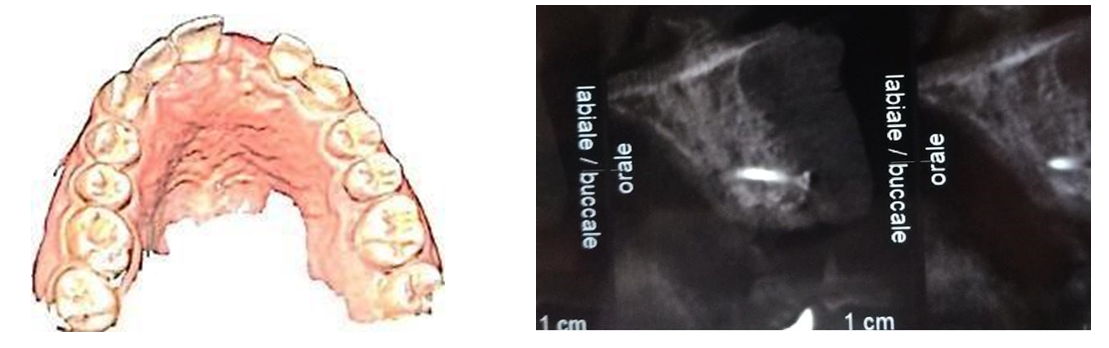
Figure 13: STL file Figure 14: post-operative radiography
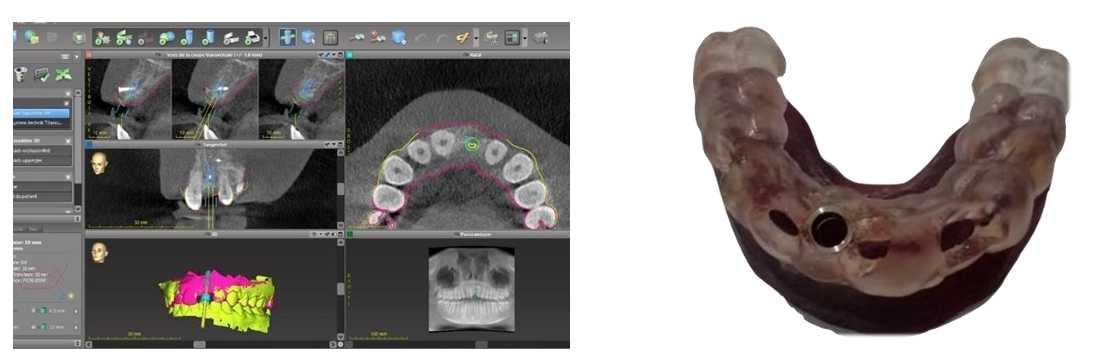
Figure 15: Software planification Figure 16: implant surgical guide
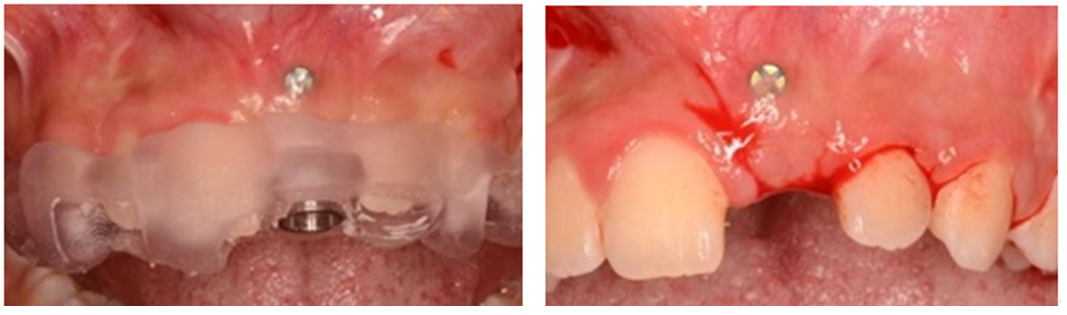
Figure 17: adaptation of the surgical guide Figure 18: incisions lines with papilla preservation
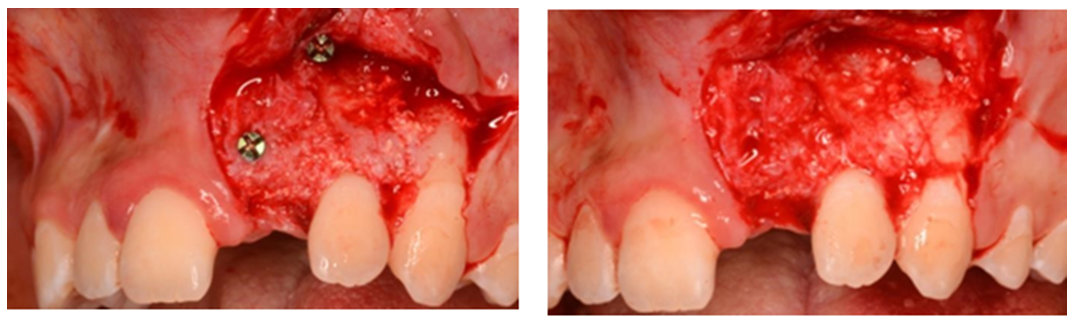
Figure 19: bone screw removal Figure 20: guided implant placement.
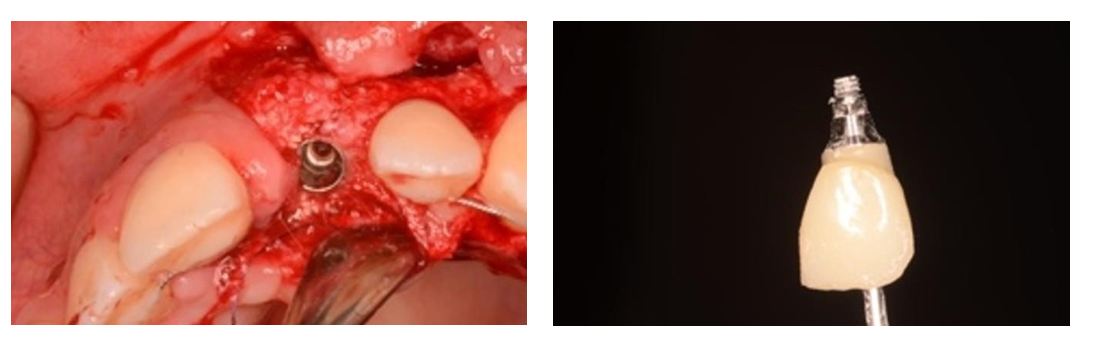
Figure 21: guided implant placement Figure 22: Provisional Crown
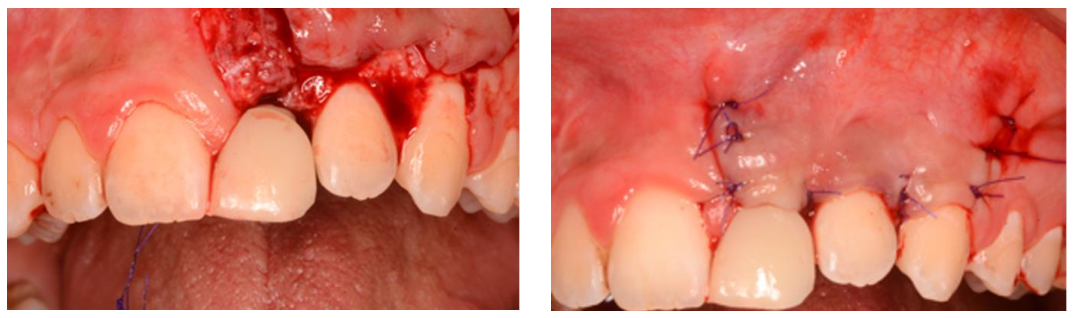
Figure 23: Screw-retained provisional crown adaptation Figure 24: Sutures
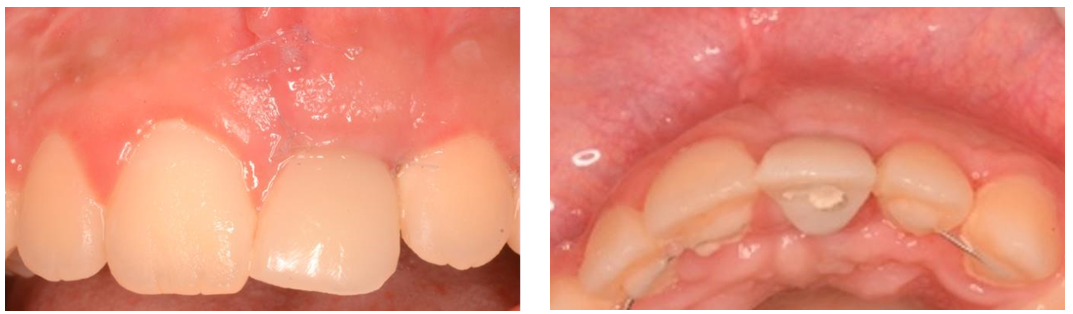 Figure 25: clinical situation (2 months of healing ) Figure 26: Occlusal view ( 2 months of healing )
Figure 25: clinical situation (2 months of healing ) Figure 26: Occlusal view ( 2 months of healing )
CASE REPORT CASE
A 42-year-old male patient, dissatisfied with his mesially extended anterior bridge replacing the right maxillary central incisor, which frequently debonds, consults for better implant supported rehabilitation.
The patient's medical history was unremarkable. He had no history of systemic diseases or medications. His oral hygiene was good.
The anamnesis reveals that the bridge had been placed five years ago to replace the missing tooth.
The clinical examination revealed that the bridge had debonded from the abutment teeth. The abutment teeth were healthy and showed no signs of decay or periodontal disease. The underlying cause of debond was not clear, but it was possible that the abutm. The anamnesis reveals that the bridge had been placed five years ago to replace the missing tooth.
The clinical examination revealed that the bridge had debonded from the abutment teeth. The abutment teeth were healthy and showed no signs of decay or periodontal disease.
The underlying cause of debond was not clear, but it was possible that the abutment teeth had shifted position over time.
The clinical and radiological examination revealed a horizontal and vertical bone defect with an accentuated buccal depression (figure 27-31).
Our therapeutic decision was to replace the tooth #8 with an implant-supported crown and to restore the teeth #9 and #10 with two crowns. ent teeth had shifted position over time. The clinical and radiological examination revealed an horizontal and vertical bone defect with an accentuated buccal depression (figure 27-31).
Our therapeutic decision was to replace the tooth #8 with an implant-supported crown and to restore the teeth #9 and #10 with two crowns.
Surgical technique:
The treatment plan includes fully guided implant placement associated with Guided bone regeneration using a titanium mesh (type SMART BUILDER: Osstem) and xenograft bone substitute and guided implant surgery.

Figure 27: baseline-clinical situation
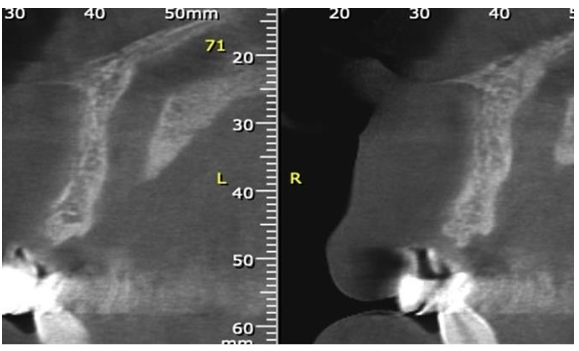
Figure 28: baseline-radiographic situation ( CBCT)

Figure 29: baseline- occlusal view (accentuated buccal depression)
The surgical technique was chosen because the bone crest was wide enough (4 mm) to allow for simultaneous implant placement and guided bone regeneration. This avoided the need for a second surgery, saving time.
We chose to place a 3 mm diameter implant, so we had to regenerate the bone in the vestibular area to have a sufficient width of the vestibular bone crest.
After a local para-apicaland a palatal anesthesia (lidocaine 2% with vasoconstrictor), the incisions were performed. The incision pattern included an intrasulcular incision extending two teeth on either side of the edentulous area with one vertical releasing incision. (Figure 32) A full-thickness flapwasraised (figure33).
Guided implant surgery with a static navigation was performed (figure 34-36).
After the implant placement, the titanium mesh (figure 37) was adapted to the surgical site and screwed to the implant with the cover screw (figure 38). Then, the xenograft was placed (Figure 39).
The titanium mesh was covered by a collagen membrane and hermetic sutures were made. (figure 40-42).

Figure 30: baseline- occlusal view after removal of the bridge


Figure 31: anterior bridge Figure 32:incisions lines


Figure 33: full thickness flap elevation (important buccal depression and large incisive foramen ) Figure 34: surgical guide
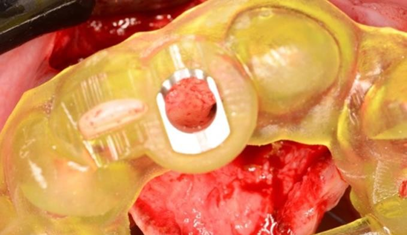

Figure 35: adaptation of the surgical guide. Figure 36: guided implant placement
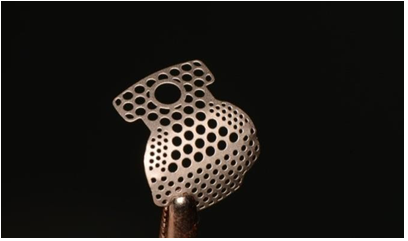
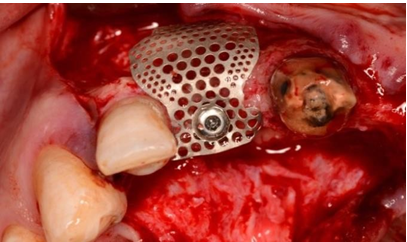
Figure 37: Titanium mesh (smart builder) Figure 38: adaptation and fixation of the titanium mesh ( smart builder)
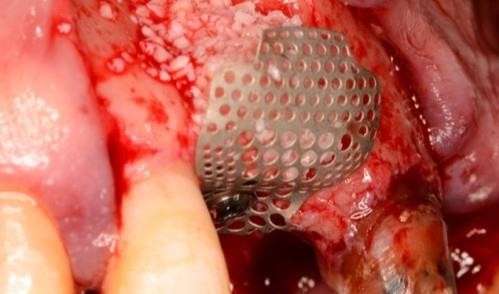
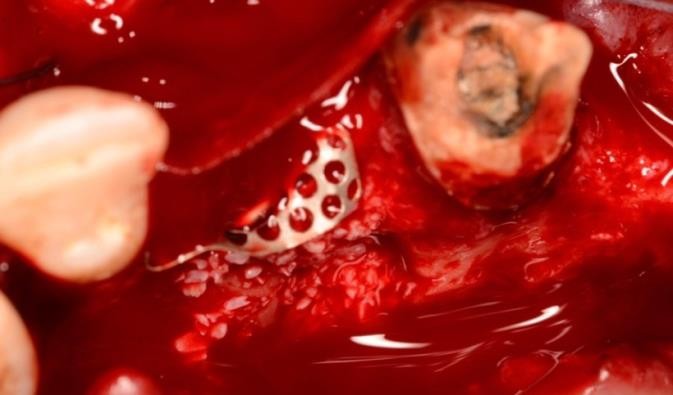
Figure 39: Bone filling materials Figure 40: collagenic membrane adaptation
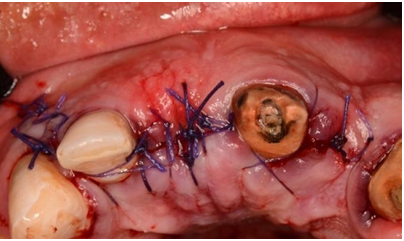

Figure 41: Sutures Figure 42: provisional bridge
DISCUSSION
Bone regeneration is one of the most challenging treatments in periodontal surgery. Bone remodeling following tumor excision, trauma, congenital anomalies, or infection can result in a large bone defect [6]
Autogenous bone grafts are considered the gold standard for bone grafting materials because of their osteoconductive, osteoinductive, and osteogenic properties, which allow for rapid and optimal bone healing [7–12].
The use of autogenous graft is therefore preferred whenever possible. However, harvesting an autogenous bone block can present several risks and disadvantages. These include donor-site morbidity, which refers to complications or issues at the site from which the bone is harvested. Additionally, patients may experience postoperative pain, increased blood loss, and an increased risk of infections. Moreover, there are limitations in terms of the quantity of bone that can be harvested and the unpredictable quality of the bone obtained [13].
To achieve effective and predictable guided bone regeneration, several principles must be respected [14].
- Flap passivation with tension Free Wound Closure
- Space Creation/Maintenance with exclusion of epithelial and Connective Cells
- Angiogenesis: Adequate Blood Supply and intra-marrow perforations
- Graft and wound stabilization during healing process
Tension-free wound closure is essential in this context because it ensures proper adaptation and stability of the flap and membrane over the graft site. By avoiding excessive tension on the flap, blood supply is maintained, promoting successful healing and integration of the bone graft. Moreover, tension-free wound closure reduces the risk of membrane exposure, infection, and graft failure, leading to improved clinical outcomes in GBR procedures [15].
Space creation and maintenance with the exclusion of epithelial and connective cells are important conditions to allow osteoblasts at the surgical site to produce and mineralize bone matrix, as well as to allow the migration of mesenchymal cells to the surgical site and their differentiation into mature osteoblasts [16].
It is now established that the main objective of guided bone regeneration (GBR) is to prevent the rapid growth of epithelial cells, fibrous tissue, and gingival connective tissue in the bone defect, and to promote the development of cells that will lead to new bone formation. Bone tissue with the slowest growth potential is the desired outcome. To achieve this objective, the appropriate membrane must be selected [17].
The choice between these two types of membranes depends on various factors, including the size and location of the bone defect, the expected healing time, and the surgeon's preference [17].
The major disadvantages of non-absorbable membranes are early exposure and the need for a second surgical procedure to remove the membrane. These disadvantages can impair the success of bone regeneration [16].
Considering the disadvantages of non-resorbable membranes, resorbable membranes, which are more biocompatible, are the gold standard in guided bone regeneration, especially in horizontal defects. However, it is important to maintain adequate space in the bone defect to prevent membrane collapse and ROG failure [16].
Titanium mesh has been shown to be effective in promoting the regeneration of sufficient bone volume for the ideal placement of dental implants, especially in the rehabilitation of complex atrophic sites, particularly those characterized by vertical bone defects associated or not with horizontal defects [18].
Titanium mesh provides several clinical advantages, including its ability to effectively address severe vertical atrophies and significant reductions in width. Additionally, in cases where soft-tissue dehiscence and mesh exposures occur, the overall incidence of major complications is significantly reduced [5].
Cortical bone perforation is an important step in ensuring adequate blood supply to the graft. In fact, it has been shown to have a favorable impact on the extent of new bone formation in grafted sites after a healing period of 7 months. Furthermore, this technique significantly enhances the number of new vessels (angiogenesis) in the treated areas. These findings highlight the beneficial effects of cortical bone perforation in promoting bone regeneration within the context of grafted sites, indicating its potential as an effective approach in supporting tissue growth and vascularization [18,19].
Cortical perforations also allow the migration of undifferentiated osteogenic cells and increase the release of growth factors [20].
Graft and flap stabilization is also an important step that should not be overlooked. The use of titanium osteosynthesis screws to fix the graft and membrane fixation screws to reinforce the graft is a good idea. The use of membrane fixation screws and bone titanium osteosynthesis screws to fix the graft provides additional stability to the surgical site during bone regeneration [16,22,23].
The surgical technique must be determined according to the amount of residual bone and the architecture of the bone defect. The surgical technique is basically divided into two categories: onlay grafting and interposition grafting. Onlay bone grafts are used to reconstruct ridges by placing an appositional graft directly on top of the cortical bone surface [28,29].
In this case, cancellous or corticocancellous grafts will be necessary. However, it is widely recognized that blocks of compact bone exhibit slower revascularization compared to corticocancellous blocks [30].
Alloplastic grafts or allogeneic grafts can be used instead of autogenous grafts due to their osteoconductive properties, the fact that they are well colonized by blood from the recipient site, and the avoidance of donor site morbidity [31].
Interpositional grafts involve the placement of graft material within a 3-, 4-, or 5-walled cancellous compartment. Socket preservation, sinus floor elevation, and splitting ridge technique are examples of interpositional grafting [32].
The success of implant-supported rehabilitation depends on the three-dimensional (3D) positioning of the implants. Indeed, poor implant positioning is considered a cofactor of peri-implantitis [33].
The problem of bone trophicity due to the absence of desmodont can be compensated for by better three-dimensional positioning of the implant, leaving a sufficiently thick vestibular wall [34].
The establishment of guided implant surgery reduces the margin of error in the three-dimensional orientation of the implant by ensuring a precise and faithful reproduction of the planning decided by the surgeon [10,35,36].
Currently, there are two approaches to implant navigation: dynamic guided implant surgery and static guided implant surgery. Dynamic navigation is a system that allows the surgeon to visualize in real time the development of the implant site on the virtual plan as the implant drills are in operation [37,38]
For static implant surgery, several levels of guidance are used [39]:
• The Full-guided (FG) approaches: guides the entire drilling sequence and implant placement,
• The Half-guided (HG) approach with Drilling guided: guides the entire drilling sequence
• The Half-guided (HG) approach with Pilot-drill guided: guides only the pilot drill.
Conforming to the type of the guide support, several guides are proposed [39]:
• Mucosa-supported guide enables flapless implant surgery, which guarantees less morbidity and minimal postoperative pain [40]. This procedure also implies a high level of patient satisfaction as well as a significant reduction in surgery time compared to flap surgery [41,42]. The use of a mucosa-supported guide with flapless implant surgery does not allow for any bone augmentation surgery and limits the surgical procedures of mucosal tissue augmentation to the tunneling technique [43]
• Tooth/crown supported guide improves the stability of the guide for partially edentulous patients throughout the surgical procedure and allows both flapless and flap surgery [44].
According to the visibility of the guide support, closed surgical guides cover the entire surgical field and do not allow visibility of the flap and edentulous ridge during the drilling sequence and implant placement. Therefore, the result obtained depends essentially on the pre-surgical planning and the effectiveness of the type of guidance system used. A wrong drilling sequence or a wrong positioning of the implant will not be detected intraoperatively [39-45].
Full-guided (FG) implant surgery, which guides the entire surgical procedure, from the drilling sequence to implant placement, offers high accuracy and reliability in the clinical reproduction of the three-dimensional implant positioning of the pre-surgical planning [46]. FG flapless implant surgery also significantly reduces operative time, which in turn reduces postoperative pain [47].
The major disadvantage of this protocol is the higher cost and the impossibility to change any decision intraoperatively because the entire surgery is planned and guided. Any error in the pre-surgical planning or in the surgical guide will systematically lead to a bad implant Positioning [48].
Half-guided (HG) approach with drilling-guided implant surgery has the same advantages as FG implant surgery with a better accuracy of implant placement compared to conventional surgery [37].
The half-guided (HG) approach with pilot-drill guided allows performing the first drilling. Guiding only the pilot drill also allows making up for a possible error in the presurgical planning [37]. The disadvantage of pilot-drill guided surgery is that the rest of the drilling sequence as well as the implant placement is operator-dependent and implies a lower precision of the implant placement compared to the pre-surgical planning [49].
A study published in the journal Clinical Oral Implants Research found that surgical templates (STs) without metallic sleeves exhibited a high level of accuracy across all three-dimensional dimensions [50].
CONCLUSION
A broad range of surgical procedures of bone augmentation is available to allow implant-supported rehabilitation under favorable conditions. The cost, availability, and expectation of the patient, the surgical technique, and the used biomaterials are the four main factors that affect the outcome of guided bone regeneration (GBR) treatment.
•Strict biological principles guide the ROG:
•Primary Wound Coverage with Tension Free Wound
CLOSURE
•Space Creation/Maintenance with exclusion of epithelial and Connective Cells
•Angiogenesis: Adequate Blood Supply and Intra-marrow perforations
•Graft and wound stabilization during healing process
Failures due to lack of knowledge or violation of the underlying biological principles, and inappropriate selection of the biomaterials used, can lead to the failure of GBR and the entire prosthetic project.
Guided surgery optimizes implant treatment by providing greater precision in the three-dimensional positioning of the implant. However, this technique requires thorough training in order to master the planning software as well as the specific surgical kit for guided implantology.
REFERENCES
1. Chappuis V, Engel O, Reyes M, Shahim K, Nolte LP, Buser D. (2013). Ridge Alterations Post-Extraction in the Esthetic Zone: A 3D Analysis with CBCT. J Dent Res. 92(12 Suppl):195S-201S.
2. Chavda S, Levin L. (2018). Human Studies of Vertical and Horizontal Alveolar Ridge Augmentation Comparing Different Types of Bone Graft Materials: A Systematic Review. J Oral Implantol. 44(1):74–84.
3. Fu PS, Wu YM, Wang JC, Huang TK, Chen WC, Huang JW, et al. (2012). Optimizing Anterior Esthetics of a Single-Tooth Implant through Socket Augmentation and Immediate Provisionalization: A Case Report with 7-Year Follow-Up. Kaohsiung J Med Sci. 28(10):559–563.
4. Schmid J, Wallkamm B, Hämmerle CH, Gogolewski S, Lang NP. (1997). The Significance of Angiogenesis in Guided Bone Regeneration. A Case Report of a Rabbit Experiment.: The Significance of Augiogenesis. Clin Oral Implants Res. 8(3):244–248.
5. Briguglio F, Falcomatà D, Marconcini S, Fiorillo L, Briguglio R, Farronato D. (2019). The Use of Titanium Mesh in Guided Bone Regeneration: A Systematic Review. Int J Dent. 2019:1–8.
6. Laubach M, Suresh S, Herath B, Wille ML, Delbrück H, Alabdulrahman H, et al. (2022). Clinical Translation of a Patient-Specific Scaffold-Guided Bone Regeneration Concept in Four Cases with Large Long Bone Defects. J Orthop Transl. 34:73–84.
7. Taheri Otaghsara SS, Joda T, Thieringer FM. (2023). Accuracy of Dental Implant Placement Using Static versus Dynamic Computer-Assisted Implant Surgery: An in Vitro Study. J Dent. 132:104487.
8. da Silva Salomão GV, Chun EP, Panegaci RDS, Santos FT. (2021). Analysis of Digital Workflow in Implantology. Case Rep Dent. 2021:1–7.
9. Giannoudis PV, Dinopoulos H, Tsiridis E. (2005). Bone Substitutes: An Update. Injury. 36(3):S20–S27.
10. Dioguardi M, Spirito F, Quarta C, Sovereto D, Basile E, Ballini A, et al. (2023). Guided Dental Implant Surgery: Systematic Review. J Clin Med. 12(4):1490.
11. Sammarco VJ, Chang L. (2002). Modern Issues in Bone Graft Substitutes and Advances in Bone Tissue Technology. Foot Ankle Clin. 7(1):19–41.
12. Tahmaseb A, Wu V, Wismeijer D, Coucke W, Evans C. (2018). The Accuracy of Static Computer-aided Implant Surgery: A Systematic Review and Metaanalysis. Clin Oral Implants Res. 29(S16):416– 435.
13. Kloss FR, Offermanns V, Kloss-Brandstätter A. (2018). Comparison of Allogeneic and Autogenous Bone Grafts for Augmentation of Alveolar Ridge Defects—A 12month Retrospective Radiographic Evaluation. Clin Oral Implants Res. 29(11):1163–1175.
14. Cucchi A, Chierico A, Fontana F, Mazzocco F, Cinquegrana C, Belleggia F, et al. (2019). Statements and Recommendations for Guided Bone Regeneration: Consensus Report of the Guided Bone Regeneration Symposium Held in Bologna, October 15 to 16, 2016. Implant Dent. 28(4):388–399.
15. Roccuzzo M, Roccuzzo A, Marruganti C, Fickl S. (2023). The Importance of Soft Tissue Condition in Bone Regenerative Procedures to Ensure Long-term Periimplant Health. Periodontol. 2000:12496.
16. Ren Y, Fan L, Alkildani S, Liu L, Emmert S, Najman S, et al. (2022). Barrier Membranes for Guided Bone Regeneration (GBR): A Focus on Recent Advances in Collagen Membranes. Int J Mol Sci. 23(23):14987.
17. Elgali I, Omar O, Dahlin C, Thomsen P. (2017). Guided Bone Regeneration: Materials and Biological Mechanisms Revisited. Eur. J Oral Sci. 125 (5):315–337.
18. Poli PP, Beretta M, Cicciù M, Maiorana C. (2014). Alveolar Ridge Augmentation with Titanium Mesh. A Retrospective Clinical Study. Open Dent J. 8 (1):148–158.
19. Lee SH, Lim P, Yoon HJ. (2014). The Influence of Cortical Perforation on Guided Bone Regeneration Using Synthetic Bone Substitutes:A Study of Rabbit Cranial Defects. Int J Oral Maxillofac. Implants. 29 (2):464–471.
20. Shih MS, Norrdin RW. (1985). Regional Acceleration of Remodeling during Healing of Bone Defects in Beagles of Various Ages. Bone. 6(5):377–379.
21.Greenberg AM. (2019). Localized Ridge Augmentation Using Guided Bone Regeneration. In Craniomaxillofacial Reconstructive and Corrective Bone Surgery; Greenberg AM, Schmelzeisen R, Eds. Springer New York: New York, NY:177–196.
22. Liu J, Kerns DG. (2014). Mechanisms of Guided Bone Regeneration: A Review. Open Dent J. 8(1):56–65.
23. Urban I, Montero E, Sanz-Sánchez I, Palombo D, Monje A, Tommasato G, et al. (2023). Minimal Invasiveness in Vertical Ridge Augmentation. Periodontol 2000. 91(1):126–144.
24. Dam VV, Trinh HA, Rokaya D, Trinh DH. (2022). Bone Augmentation for Implant Placement: Recent Advances. Int J Dent. 2022:1–7.
25. Alagl AS, Madi M. (2018). Localized Ridge Augmentation in the Anterior Maxilla Using Titanium Mesh, an Alloplast, and a Nano-Bone Graft: A Case Report. J Int Med Res. 46(5):2001–2007.
26. Caggiano M, D’Ambrosio F, Giordano F, Acerra A, Sammartino P, Iandolo A. (2022). The “Sling” Technique for Horizontal Guided Bone Regeneration: A Retrospective Case Series. Appl Sci. 12(12):5889.
27. Elnayef B, Porta C, Suárez-López Del Amo F, Mordini L, Gargallo-Albiol J, Hernández-Alfaro F. (2008). The Fate of Lateral Ridge Augmentation: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 33(3):622–635.
28. Rocchietta I, Fontana F, Simion M. (2008). Clinical Outcomes of Vertical Bone Augmentation to Enable Dental Implant Placement: A Systematic Review. J Clin Periodontol. 35:203–215.
29. Elnayef B, Monje A, Gargallo-Albiol J, Galindo-Moreno P, Wang HL, Hernández-Alfaro F. (2017). Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 32(2):291–312.
30. Rocchietta I, Simion M, Hoffmann M, Trisciuoglio D, Benigni M, Dahlin C. (2016). Vertical Bone Augmentation with an Autogenous Block or Particles in Combination with Guided Bone Regeneration: A Clinical and Histological Preliminary Study in Humans: GBR with Autogenous Block or Particulate Graft. Clin Implant Den Relat Res. 18(1):19–29.
31. Karalashvili L, Kakabadze A, Uhryn M, Vyshnevska H, Ediberidze K, Kakabadze Z. (2018). Bone grafts for reconstruction of bone defects (review). Georgian Med News. 282:44–49.
32. Nkenke E, Stelzle F. (2009). Clinical Outcomes of Sinus Floor Augmentation for Implant Placement Using Autogenous Bone or Bone Substitutes: A Systematic Review. Clin Oral Implants Res. 20:124–133.
33. Rosen PS, Froum SJ, Sarmiento H, Wadhawani CP. (2022). A Revised Peri-Implantitis Classification Scheme: Adding Three-Dimensional Considerations to Facilitate Prognosis and Treatment Planning. Int J Periodontics Restorative Dent. 42(3):291–299.
34. Monje A, Chappuis V, Monje F, Muñoz F, Wang HL, Urban IA, et al. (2019). The Critical Peri-Implant Buccal Bone Wall Thickness Revisited: An Experimental Study in the Beagle Dog. Int J Oral Maxillofac Implants. 34(6):1328–1336.
35. Block MS, Emery RW, Cullum DR, Sheikh A. (2017). Implant Placement Is More Accurate Using Dynamic Navigation. J Oral Maxillofac Surg. 75(7):1377–1386.
36. Qahash M, Susin C, Polimeni G, Hall J, Wikesjö UM. (2008). Bone Healing Dynamics at Buccal Peri-Implant Sites. Clin Oral Implants Res. 19(2):166–172.
37. Kühl S, Zürcher S, Mahid T, Müller-Gerbl M, Filippi A, Cattin P. (2013). Accuracy of Full Guided vs. HalfGuided Implant Surgery. Clin Oral Implants Res. 24(7):763–769.
38. Vercruyssen M, Fortin T, Widmann G, Jacobs R, Quirynen M. (2014). Different Techniques of Static/Dynamic Guided Implant Surgery: Modalities and Indications. Periodontol 2000. 66 (1):214–227.
39. Gargallo-Albiol J, Barootchi S, Salomó-Coll O, Wang HL. (2019). Advantages and Disadvantages of Implant Navigation Surgery. A Systematic Review. Ann Anat Anat Anz. 225:1–10.
40. Farley NE,Kennedy K, McGlumphy EA, Clelland NL. (2013). Split-Mouth Comparison of the Accuracy of Computer-Generated and Conventional Surgical Guides. Int J Oral Maxillofac Implants. 28 (2):563–572.
41. Amorfini L, Migliorati M, Drago S, Silvestrini Biavati A. (2017). Immediately Loaded Implants in Rehabilitation of the Maxilla: A Two-Year Randomized Clinical Trial of Guided Surgery versus Standard Procedure: Guided Surgery versus Standard Technique for Immediate Loading: A RCT. Clin Implant Dent Relat Res. 19(2):280–295.
42. Arısan V, Bölükbaşı N, Öksüz L. (2013). Computer-Assisted Flapless Implant Placement Reduces the Incidence of Surgery-Related Bacteremia. Clin Oral Investig. 17(9):1985–1993.
43. Romandini M, Ruales-Carrera E, Sadilina S, Hämmerle CHF, Sanz M. (2023). Minimal Invasiveness at Dental Implant Placement: A Systematic Review with Meta-analyses on Flapless Fully Guided Surgery. Periodontol 2000. 91(1):89–112.
44. Orentlicher G, Abboud M. (2011). Guided Surgery for Implant Therapy. Oral Maxillofac Surg Clin N Am. 23(2):239–256.
45. Boa K, Barrak I, Varga E Jr, Joob-Fancsaly A, Varga E, Piffko J. (2016). Intraosseous Generation of Heat during Guided Surgical Drilling: An Ex Vivo Study of the Effect of the Temperature of the Irrigating Fluid. Br J Oral Maxillofac Surg. 54(8):904–908.
46. Chen Z, Li J, Ceolin Meneghetti P, Galli M, Mendonça G, Wang HL. (2022). Does Guided Level (Fully or Partially) Influence Implant Placement Accuracy at Post-Extraction Sockets and Healed Sites? An in Vitro Study. Clin Oral Investig. 26(8):5449–5458.
47. De Santis D, Gelpi F, Zambotti T, Rossetto A, Luciano U, Zotti F, et al. (2020). The Use of Computer-Guided Flapless Dental Implant Surgery (Nobel Guide®) and Immediate Function to Support a Fixed Full-Arch Prosthesis in Fresh Frozen Homologous Bone Grafted Patients: A Retrospective Cohort Study with 5 to 8-Year Follow-Up. J Biol Regul Homeost Agents. 34(6 Suppl. 2):49–61.
48. Ravidà A, Barootchi S, Tattan M, Saleh MHA, Gargallo-Albiol J, Wang HL. (2018). Clinical Outcomes and Cost Effectiveness of Computer-guided versus Conventional Implant-retained Hybrid Prostheses: A Long-term Retrospective Analysis of Treatment Protocols. J Periodontol. 89(9):1015–1024.
49. Schulz MC, Hofmann F, Range U, Lauer G, Haim D. (2019). Pilot-Drill Guided vs. Full-Guided Implant Insertion in Artificial Mandibles—a Prospective Laboratory Study in Fifth-Year Dental Students. Int J Implant Dent. 5 (1):23.
50. Tallarico M, Czajkowska M, Cicciù M, Giardina F, Minciarelli A, Zadrożny Ł, et al. (2021). Accuracy of Surgical Templates with and without Metallic Sleeves in Case of Partial Arch Restorations: A Systematic Review. J Dent. 115:103852.